


1Department of Dermatology and Venereology, Sahlgrenska University Hospital, Gothenburg, Sweden, and 2Department of Dermatology, East Jeddah General Hospital, Jeddah, Saudi Arabia. E-mail: loai.salah@gmail.com
Accepted Nov 29, 2017; Epub ahead of print Dec 4, 2017
Methotrexate (MTX), a folic acid inhibitor, has been used to treat psoriasis since the 1970s (1). It is the first systemic drug of choice for treatment of moderate-to severe psoriasis or when topical and ultraviolet (UV) therapy is insufficient. MTX is highly effective with few side-effects (2). In recent studies, Psoriasis Area and Severity Index 75 (PASI 75) was reached by 36–40% of MTX-treated patients within 16–24 weeks of treatment (3, 4). This was considered a successful treatment response according to the definition established by the European Consensus Program (ECP) in 2011. The programme encouraged clinicians to consider the goal of treatment as a PASI reduction from baseline of 75% or more (PASI 75), or a PASI reduction of 50–75% (PASI 50) combined with Dermatology Life Quality Index (DLQI) ≤ 5, in terms of absolute value within the first 6 months of treatment. If these goals were not achieved, the ECP recommended modification of treatment by increasing the dosage, changing medication, or combining different therapies (5). Over the past decade biological therapy has been launched as an efficient alternative in management of psoriasis. Yet, studies have reported a tendency to undertreat and for patients to remain on conventional therapy for a long time, even when the results are sub-optimal (6–8). A study of 2,646 Swedish patients showed that, despite receiving systemic treatment, one in every 5 patients had ongoing moderate-to-severe psoriasis (9). However, efforts are being made to reach a consensus regarding the use of MTX as per the guidelines reported based on the Danish expert meeting (10).
The aim of the current study was to evaluate MTX treatment of psoriasis at the Department of Dermatology at Sahlgrenska University Hospital in Sweden, focusing on treatment effect and evaluating how cases with sub-optimal response were managed in relation to existing guidelines.
This retrospective, longitudinal study was based on PsoReg, a national quality register for systemic psoriasis treatment, and medical records (11). A list of all patients with psoriasis registered from 2007 in PsoReg was obtained in May 2014, including data on medication, dosages, PASI and DLQI values and demographics. All data were verified using medical records and missing information was supplemented from the records. Included subjects were MTX-naïve patients with plaque psoriasis, who were starting MTX treatment after having a registered PASI assessment. The maximal time from the first assessment until starting treatment was 3 months. In addition, at least one registered PASI value was required within 9 months after baseline. Any patient not fulfilling these criteria was excluded from entering the study (Fig. S1). The patients were followed for the first year of treatment, with follow-up points at 3, 6 and 12 months. Due to diversity of the follow-up pattern, these points were defined as 60–149, 150–270 and 300–540 days from the baseline date, respectively. Reported data outside of these time frames were excluded. At each assessment, available information on PASI, DLQI, treatment dosage and use of supplementary topical or UV treatment was documented. The majority of patients (n = 90, 94.7%) were orally treated with MTX, and, during that period, folic acid was given in a fixed dose of 5 mg/week to all patients, in accordance with the latest guidelines. The time of stopping MTX therapy during the study was 6 weeks or less. The main outcome was the frequency of successful therapy response according to the ECP definition (5) and PASI 75, since this is a frequently used measurement in randomized controlled trials (RCTs). Observations were made within the group that did not reach treatment goals; here outcomes of interest were changes in MTX dosage, supplementary therapy and switches to alternative treatment.
Descriptive and analytical statistical analyses were performed using R version 3.0.3 (The R Foundation for Statistical Computing, Vienna, Austria). A logistic regression was used to analyse attainment of successful treatment response (PASI 75 or PASI 50 and DLQI ≤5) at 3, 6 and 12 months vs. covariates.
The study was approved by the regional ethics committee in Gothenburg (protocol number 496-15).
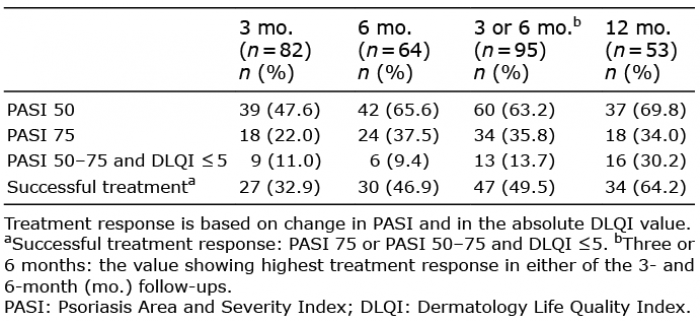
A total of 95 patients (60% males) were included in the study. The mean age was 49 years, and mean PASI at baseline was 11.2. Of the original 95 patients, 82, 64 and 53 had reported data on PASI values at 3, 6 and 12 months, respectively. Additional demographics are shown in Table SI. The effect of treatment on PASI and DLQI is shown in Table I and Figs S2 and S3. A successful treatment response was reached by 33%, 47% and 64% at 3, 6 and 12 months, respectively.
Table I. Response to methotrexate (MTX) treatment shown by the different points of follow-up visits
With regards to the group that did not reach the ECP treatment goals, 29% stayed on the same dose at 3 months, and 50% at 6 months. Eleven percent stopped treatment by 3 months, and 6% by 6 months. In addition, 32 patients (58.2%) with unsuccessful response at 3 months and 10 (29.4%) at 6 months, respectively, had their MTX doses increased. Finally, 6% changed to another systemic therapy by 6 months, but none at 3 months. Details of the actions at unsuccessful treatment are shown in Table II.
In the whole study group, 7 patients (7.4%) switched to another systemic treatment within the entire study period (540 days); of these, 4 patients received etanercept, 2 acitretin and 1 ustekinumab.
Table II. Actions at unsuccessful treatment
A logistic regression, with successful treatment outcome at 3, 6 and 12 months as the dependent variable versus sex, age, smoking, arthritis, body mass index (BMI) and MTX dose yielded a significant outcome only for BMI (i.e. more successful treatment outcomes for those with lower BMI) (3 months: p = 0.014, log odds ratio (OR)BMI= –0.16, 95% confidence interval (95% CI): (–0.30, –0.02), 6 months: p = 0.011, log ORBMI = –0.24, 95% CI: (–0.47, –0.01), 12 months: p = 0.019, log ORBMI = –0.24, 95%CI: (–0.47, –0.01)). The log ORs refer to partial log ORs.
The primary finding was that many patients remained on the same treatment regimen, even when it was deemed unsuccessful according to the ECP. Treatment response in the studied population was comparable to that in other trials, and treatment was managed, partly, in accordance with existing guidelines. Treatment response, measured as a PASI decrease, was most apparent within the first 3 months (33% of patients) and continued up to 6 months of treatment (47% of patients). Thereafter, little additional effect was seen. Similarly, in studies by Saurat et al. (4) and Reich et al. (3), PASI 75 was achieved by 36% of patients by 4 months, and 40% by 6 months, respectively. The introduction of PASI 75 was intended mainly for use in clinical trials whereas in clinical settings, it is easier to use an absolute PASI value as a treatment goal. There was a loss of follow-up over time, indicating either that treatment was stopped, or that there was a lack of data reported. In theory, this could result from poor response to therapy; however, it is also plausible that in cases with good stable therapy response, and no complications, follow-ups and registrations were considered less necessary.
According to the ECP, the induction phase can last for up to 6 months for a systemic treatment (5). Therefore, it is reasonable, at 3 months, to await increased clinical effect before making major changes in treatment (12). This tendency was seen in our study, as no additional or alternative systemic treatment was initiated at this point, with one-third of patients having no change in dosage, and approximately half receiving an increased dose. On the other hand, one can expect the optimal treatment response to be achieved by 6 months, and therefore any major intervention should be avoided up to this time point. This practice was supported by our findings, and other publications, including the updated European treatment guidelines from 2014 (3, 12). In our study, approximately 50% less attempts to increase dose were made at 6 months than in the first 3-month period. This might indicate that most patients were thought to have reached their expected highest treatment effect with MTX. Instead, therapy alterations at 6 months consisted largely of adding supplementary therapy. Change in treatment was rarely noticed, as the majority of those who did not reach treatment goals by 3 or 6 months still had MTX treatment at 12 months. In general, every third patient continued MTX treatment despite not achieving the recommended treatment goals. Failure to follow the guidelines in these cases could generally be attributed to multiple intertwining factors, including the skill, experience, knowledge and beliefs of the doctor in charge, as well as the characteristics of the patient being treated (13).
The authors have no conflict of interest to declare.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize