


1Department of Dermatology, 2Center for Melanoma and Cancer Immunotherapy, Sharett Institute of Oncology, and 3Department of Pathology, Hadassah – Hebrew University Medical Center, 9112001 Jerusalem, Israel. E-mail: yael.renert@gmail.com
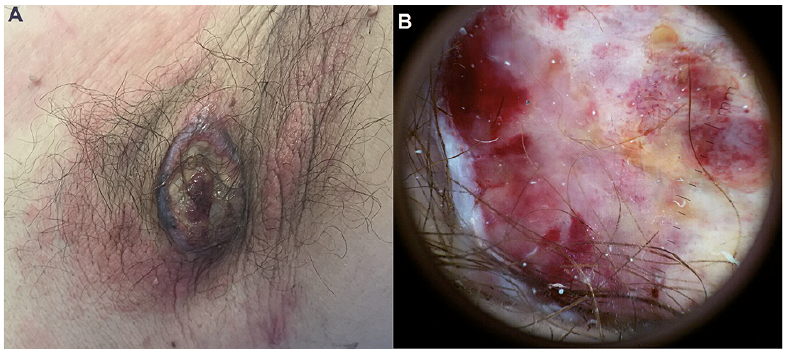
A 48-year-old healthy man presented to our dermatology outpatient referral clinic with a growing ulcer in his left armpit. The patient reported that the ulcer had developed following forceful hair plucking from this area. The lesion had appeared as a small papule one year earlier, with rapid growth and ulceration over the past 2 months. Clinical examination revealed an indurated, oval ulcer in the left armpit fold, measuring 5 cm in diameter, with a fibrotic ulcer bed and a hypergranulated, erythematous centre (Fig. 1A). The borders of the ulcer were undermined and darker than the surrounding skin tone, with colour ranging from pink to dark-purple/black. The skin around the ulcer showed erythematous plaques with no pustules or sinuses. Dermatoscopy revealed ulceration, with linear irregular vessels and milky-red blotches. No pigmented features were seen in the centre of the lesion (Fig. 1B). Previous treatment included oral and local antibiotics with no clinical response.
What is your diagnosis? See next page for answer.
Fig. 1. Clinical features. (A) Undermined, indurated ulcer in the patient’s left armpit with erythematous plaques in the surrounding skin. (B) Dermatoscopy showing an ulcerative lesion with milky-white blotches and linear irregular vessels.
Acta Derm Venereol 2018; 98: XX–XX.
Diagnosis: Nodular melanoma (NM)
Following detailed history taking and physical examination, a 3-mm punch biopsy was taken from the border of the ulcer. The biopsy revealed a dense infiltrate of neoplastic melanocytes with a single mitosis in an area of 1 mm2. The depth of invasion was at least 4 mm into the dermis (Fig. 2). Tumour cells stained positively for MART1 and SOX10 (Fig. 3). Positron emission tomography – computed tomography (PET-CT) showed a positive axillary lymph node. Excisional surgery and sentinel lymph node biopsy were performed. Pathology revealed 12-mm Breslow depth of invasion in the primary NM lesion, and melanoma metastases were found in the 3 resected lymph nodes. The largest metastasis diameter was 16 mm. Further work-up demonstrated activating mutation in BRAF. The treatment plan includes complementary axillary lymph node dissection and radiotherapy, as recommended for selected patients with involvement of 2 or more axillary lymph nodes, according to the updated National Comprehensive Cancer Network (NCCN) guidelines (Version 1.2017). Accrual to a clinical study of pembrolizumab vs. placebo after complete resection of high-risk stage III melanoma will be considered.
Since the thickness of the primary lesion is strongly associated with disease mortality, and more than 50% of thick melanomas (> 4 mm) are NM, this rapidly progressive subtype has particularly poor prognosis (1, 2). In one large cohort, NM was responsible for 43% of deaths due to melanoma, although accounting for only 14% of invasive melanomas (2). NMs are diagnosed more commonly in older men, on the lower limbs, head and neck, and have a greater association with a history of solar keratoses than do superficial spreading melanoma (1). Early detection is crucial for survival. Dermatoscopy can sometimes be challenging in the diagnosis of NM. Ulceration, homogeneous disorganized pattern, and homogeneous blue-pigmented structureless areas are dermatoscopic patterns that are more often associated with NM compared with the other melanoma subtypes. Another diagnostic feature is black dots and globules, which are most significantly correlated with NM when peripherally distributed (3, 4). Peripheral light-brown structureless areas are associated with thin melanoma, and correlate negatively with NM (3). In general, fast-growing melanomas are associated with ulceration and an atypical vascular pattern. An atypical pigmented network is a less common feature (5). The relative symmetry of NM compared with other invasive melanomas makes the diagnosis more difficult (4, 5). Here, the atypical location in the armpit and the speculated trauma-induced undermined ulceration raised the differential diagnosis of hidradenitis suppurativa and pyoderma gangrenosum. Dermatoscopy showed only a few classical melanoma-related features. The Breslow score and the tumour’s ulceration predict a poorer prognosis, regardless of lymph node involvement. This highlights the need for a high index of suspicion and prompt histological examination in the case of rapidly growing ulcers.
Fig. 2. Biopsy of the border of the ulcer. (A) Tumour invasion is observed through the entire specimen (haematoxylin and eosin (H&E) staining, 40× magnification). (B) Higher magnification, showing a dense infiltrate of atypical melanocytes with hyperchromatic nuclei without signs of maturation (H&E staining, 200× magnification).
Fig. 3. Immunohistochemistry. (A) MART1 and (B) SOX10 staining, showing a dense melanocytic infiltrate, reinforcing the diagnosis of melanoma (100× magnification).


 Click to show fullsize
Click to show fullsize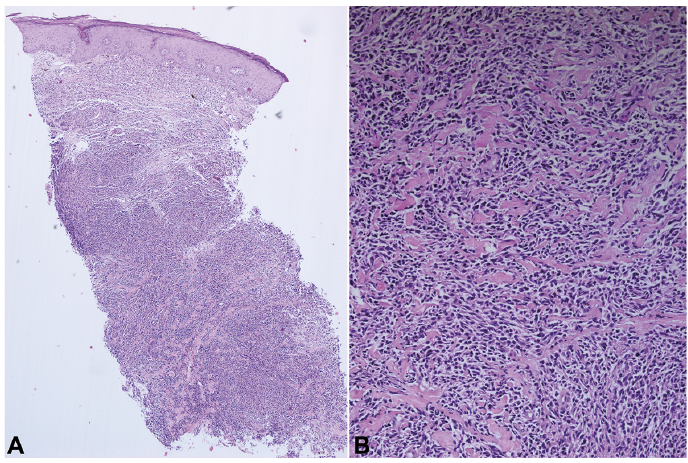 Click to show fullsize
Click to show fullsize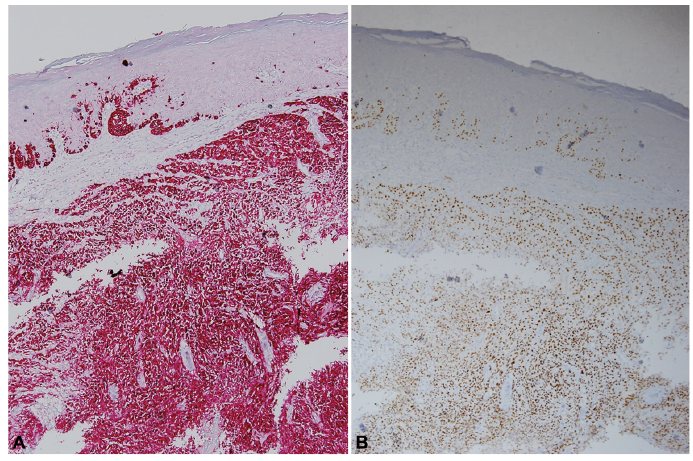 Click to show fullsize
Click to show fullsize