


1Department of Nursing, Gyeongnam National University of Science and Technology School of Nursing, South Korea, 2Duke University School of Nursing, Durham, North Carolina, USA, 3Seoul International School, Gyeonggi-do, South Korea, and 4JF Dermatology Clinic, Seoul, South Korea
Atopic dermatitis (AD), a common childhood skin disorder, can limit a child’s learning and physical activities. South Korean mothers, as primary caregivers, experience anxiety and helplessness when caring for their ill children. The aim of this study was to develop a hybrid AD education programme (consisting of a face-to-face session followed by 8 online sessions) and evaluate its effects on anxiety, caregiving efficacy and caregiving behaviour among mothers of children with AD. Twenty mothers of patients with AD treated in a South Korean hospital received one on-site session and 8 weekly online modules. After the intervention, mothers’ mean ± standard deviation anxiety reduced (from 50.3 ± 14.2 to 31.7 ± 6.3 points, t = 5.75, p < 0.001). Their caregiving efficacy and caregiving behaviour improved significantly, from 18.3 ± 3.5 to 29.4 ± 3.2 points (t = –9.64, p < 0.001) and from 47.7 ± 7.7 to 78.8 ± 4.9 points (t = –14.4, p < 0.001), respectively. The effects of the hybrid education programme for this population were significant. Healthcare providers should consider examining the programme nationwide, including in rural areas, while investigating its long-term effects.
Key words: atopic dermatitis; caregiving behaviour; caregiving efficacy; hybrid education programme; mother’s anxiety.
Accepted Dec 6, 2017; Epub ahead of print Dec 12, 2017
Acta Derm Venereol 2018; 98: xx–xx.
Corr: Je-Bog Yoo, Department of Nursing, Gyeongnam National University of Science and Technology, Gyeongsangnam-do, South Korea. E-mail: jbyoo@gntech.ac.kr
The rate of prevalence atopic dermatitis (AD) in South Korea has been increasing as a result of environmental contamination, consumption of instant foods (e.g. ramen), and the westernization of diets (1). According to data from the National Health Insurance Service (2), in 2014 a total of 86.9 million individuals were treated for atopic diseases; 54.5 million for allergic rhinitis, 22 million for asthma, and 10.4 million for AD incidence. Toddlers and pre-school children are disproportionately affected by AD, and in 2011, 41.7% of these children were diagnosed with AD, suggesting the need for management of AD symptoms in children under the age of 7 years (3). Poor dermatological conditions can affect children’s relationships with peers at school (4), as well as the quality of life of patients with AD and their parents (5). Hospitalization is necessary when AD is accompanied by viral, bacterial, or fungal infections (6). This, in turn, can inhibit the child’s normal growth and developmental process. Given this evidence, the importance of managing atopic diseases in children has been increasingly emphasized in recent years (5, 7).
Adopting a healthy lifestyle involves making the right choices regarding diet, exercise, and medication, and such choices are important for managing AD (8). In South Korean culture, mothers assume the role of care of their children, especially for those with chronic illnesses (9). Thus, mothers are in the unique position of ensuring that their children comply with their treatment plans (10). However, mothers of children with AD experience high anxiety and psychological pain due to feelings of responsibility and uncertainty about their children’s illness (6, 11). Formal AD education and support have proven effective in helping mothers deal with anxiety by improving their knowledge and confidence (12).
Online learning is recognized as an optimal method for providing health education because of its accessibility, ease of use, economic efficiency, and availability to a large number of people (13, 14). Due to the expansion of the learning environment to online education, parents of children with AD can use online learning methods to overcome obstacles to attendance at in-person educational programmes, such as lack of time, responsibilities at home and work, and physical and psychological difficulties (15, 16). Thus, mothers of children with AD may benefit from a standardized online education programme about disease management. However, a combination of online and offline education may be more effective than online learning alone to improve learning outcomes from the viewpoint of holistic education (17). Despite the fact that the review from 2014 by Ersser et al. (18) contained 10 studies showing that educational and psychological approaches helped caregivers to provide better at-home care for their children with AD, the studies lacked detail about intervention design. Therefore, it remains difficult to assess which intervention works best for this population. In addition, only a few of the studies included in Ersser et al.’s review addressed the topic of eHealth and how it can benefit patients with AD and their families. Moreover, in their pilot randomized controlled trial on self-care for families of children with eczema, using web-based interventions and healthcare professional support, Santer et al. (19) concluded that a full-scale study was feasible by quantifying the effective-ness of the intervention for this particular population. Therefore, the current study aims to fill these gaps in the literature by investigating changes in the degree of anxiety, perceptions of caregiving efficacy, and subsequent changes in caregiving behaviours among mothers of children with AD after the mothers participated in a novel online-offline AD education programme. The data gleaned from this study may be useful for developing or enhancing health education programmes aimed at assisting this population.
The quasi-experimental study was conducted using a 1-group, pre-and post-test design with mothers whose children had been diagnosed with AD. The children were patients in a hospital in Seoul, South Korea, between 1 July and 30 August 2016. The children’s mothers were invited to participate in the study if: (i) they planned for their children to undergo treatment for AD, (ii) their children did not have any medical, physical, or psychological problems that could interfere with the study protocol, (iii) they fully understood the purpose of the study, and (iv) they had never participated in any other treatment programmes for AD. The children and their mothers were recruited via advertisements in public health centres, kindergartens, and churches. A minimum sample size of 19 participants was calculated using G*power 3.1.9 with Cohen’s (20) formula of sample size estimation with an effect size of 0.80, alpha level of 0.05, and power of 95%. With a potential 20% drop-out rate in mind, 23 participants were recruited.
For protection of the participants as an ethical requirement, intervention and data collection were conducted after receiving approval from the Institutional Review Board of H University (IRB No. HIRB-2016-032) and consent forms were signed by participating mothers. An intervention team consisting of a dermatologist, nurse, nurse assistant, and programme coordinator affiliated with the hospital developed and delivered the hybrid learning programme, comprising both offline and online education components. Because improvements in dermatological conditions are usually detected after a minimum of 8 weeks of consistent care (21), the programme included 8 weeks of lessons, with objectives and contents delivered on a daily or weekly basis.
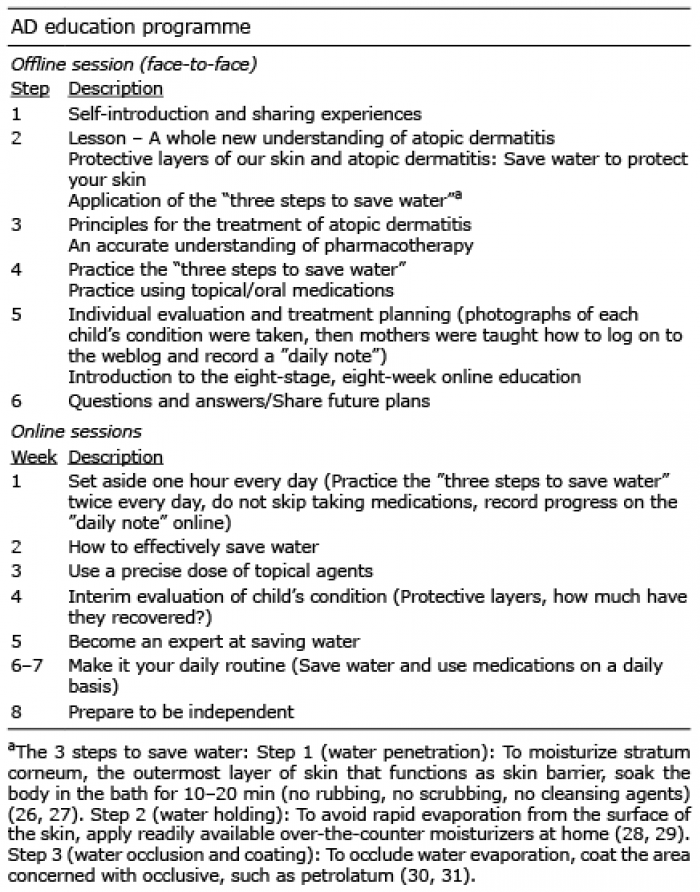
On the first day of the AD management programme, the education team and participating mothers and children met in person at the hospital. The research director introduced the programme to the mothers and provided them with information about the management of AD. The 4-h on-site orientation meeting consisted of practical information about managing AD, question-and-answer sessions with the education team, individual evaluation of the severity of each child’s condition by the dermatologist using the SCORing Atopic Dermatitis (SCORAD) index (22), and treatment planning. During this orientation, mothers were also encouraged to share their feelings of anxiety and uncertainty, with the intention that a support group of others facing similar stressors would reduce their anxiety (23). Mothers were also informed about online education lessons (http://cafe.naver.com/happyskin; site in Korean). The content of each week’s online session is described in Table I, as are the contents of the offline education session. In addition, Table II illustrates the recommended dosing and method of applying topical corticosteroids that mothers were given. At the offline education session, the programme coordinator distributed a paper survey to all mothers to be completed during the session.
Table I. Description of the hybrid atopic dermatitis education programme for mothers of children with atopic dermatitis (AD)
Table II. Precise recommended dosage of topical corticosteroids for applying to children’s skin (22, 32)
A week after the on-site orientation meeting, mothers participated in 8 weeks of online lessons at home. Every Saturday during their online lessons, mothers were encouraged to ask questions or upload pictures of their children’s skin conditions on the group’s weblog, which featured areas for uploading images and care diaries and for asking questions. Dermatologists responded to all participants’ questions on the weblog so that all the participating mothers had access to the information. In addition, the weblog administrator uploaded brief weekly reports to communicate individually with each participant. These reports were made accessible to other participants to help them gain insight into others’ experiences. Post-intervention surveys were posted to each mother’s house one week after completion of the 8-week programme. The surveys are described below.
Anxiety. An anxiety measurement tool developed by Spielberger (24) and translated into Korean by Kim & Shin (25) was used to measure the participating mothers’ level of anxiety. The survey consists of 20 questions rated on a 4-point Likert scale (1 = strongly disagree, 2 = disagree, 3 = agree, 4 = strongly agree) with a possible total score of 20–80. High scores indicate high levels of anxiety. Cronbach’s α for internal consistency reliability was 0.88 in a study by Kim & Shin (25) and 0.96 in the present study. The tool was used after obtaining permission from its developer.
Caregiving efficacy. We also used the Parenting Sense of Competence Scale (PSOC), developed by Gibaud-Wallston & Wandersman (33), modified by Johnston & Mash (34), and further modified by Lee & Han (35), to measure the perceptions of caregiving competence of mothers whose children have AD. The tool consists of 7 questions rated on a 6-point Likert scale (1 = strongly disagree, 2 = disagree, 3 = slightly disagree, 4 = slightly agree, 5 = agree, 6 = strongly agree) with a possible total score of 7–42. High scores indicate mothers’ perceptions that their caregiving competence is high. Cronbach’s α for internal consistency reliability was 0.79 in a study by Lee & Han (35) and 0.81 in the present study. The PSOC was used after obtaining permission from its author.
Caregiving behaviours. A 16-item tool used by Kwon & Seo (36) and the Ministry of Environment (3) to assess at-home caregiving behaviours of parents of children with AD was modified to address the topic of AD care, and its reliability and validity were verified. This modified tool consisted of 25 questions about measures that mothers should implement to prevent and alleviate symptoms of AD at home: life management (7 items), cleansing and bath (9 items), skin care (4 items), and medication (5 items). Five mothers who had children with AD were invited to complete a preliminary survey in which they reviewed the tool in terms of vocabulary, comprehension difficulty, ease of responding to items, and room for improvement. Their opinions were considered when we revised and completed the modification of the tool. To ensure content validity of the tool, each question was reviewed by 2 professors of paediatric nursing, who specialize in care for children with AD, and a paediatric dermatologist. Also, factor analysis showed that the questions explained 74% of overall variability of the tool. Cronbach’s α for reliability stood at 0.85. Sample items included, “When washing my face, I do not rub it hard”; “I finish the shower or bath by rinsing my skin with lukewarm water”; “I use a moisturizer that is thick enough not to slop around when shaken strongly”; “For a lightly or extensively affected area, I mix moisturizer and Vaseline® with a specific amount of topical steroid, and apply the mixture on the area.” Each of the 25 of questions on the modified tool was rated on a 4-point Likert scale (1 = strongly disagree, 2 = disagree, 3 = agree, 4 = strongly agree) with a range of 25–100. High scores indicate high levels of engagement in care management and completion of expected caregiving tasks by mothers.
All collected data were analysed with SPSS software, version 21.0 (SPSS, Chicago, IL, USA). Numbers, percentages, means, and standard deviations (SD) were calculated for the demographic characteristics of the mothers and their children, and additional subgroup analyses were performed according to mothers’ characteristics to determine if any of the characteristics were individually associated with the mothers’ anxiety, caring efficacy, and caring behaviour towards their children with AD. To analyse the effects of the AD management programme, participating mothers’ levels of anxiety, caregiving efficacy, and caregiving behaviour before and after the education programme were compared in terms of their mean and SD by using a paired t-test.
Of the 23 mothers who consented to the study, 20 completed the programme (Fig. 1). Three mothers were aged 35 years or less, 8 were aged 36–40 years, and 9 were aged 41 years or older. Thirteen participants had completed university, and 11 were unemployed. All 20 participants agreed that there was a need for education on AD. Among the 20 children, 12 were boys and 8 were girls. Twelve children were younger than 10 years and 8 were aged 10 years or older. Twelve patients had a family history of AD and the others had no history. None of the patients had a previous history of hospitalization. Eleven of the patients reported that their AD had persisted for more than one year, while the remaining participants had not yet had the disease for a year. Arms were the most commonly affected site, followed by legs, and torso. Alimentary allergy was the most common diagnosis, found in 15 patients (75%). The mean baseline severity of children’s AD was 74.61 ± 12.79, with a possible total score of 0–103. AD severity levels and demographic information on mothers and their children are given in Table III.
Fig. 1. Flow chart showing enrollment and intervention procedure.
Table III. Demographic characteristics of children (n = 20) with atopic dermatitis (AD) and their mothers (n = 20)
Mothers’ mean anxiety scores decreased significantly from 50.3 ± 14.2 points before the AD management programme to 31.7 ± 6.3 points at the end of the programme (t = 5.75, p < 0.001). The mean caregiving efficacy score significantly increased from 18.3 ± 3.5 points before the programme to 29.4 ± 3.2 points at the end of the programme (t = –9.64, p < 0.001). Likewise, the mean caregiving behaviour score increased from 47.7 ± 7.7 points before the programme to 78.8 ± 4.9 points at the end of the programme (t = –14.4, p < 0.001). Changes in anxiety levels, confidence in caregiving abilities, and caregiving behaviours by demographic characteristics are shown in Table IV. No significant difference in mothers’ anxiety levels was found when comparing the mothers’ scores on these variables according to their child’s age (t = –2.966, p = 0.102), sex (t = 2.519, p = 0.130), family history of AD (t = 0.472, p = 0.501), onset of symptoms (t = 0.200, p = 0.660), mother’s age (t = 1.392, p = 0.253), religion (t = 0.202, p = 0.658), mother’s employment status (t = 2.020, p = 0.172), and previous experience in receiving education on AD (t = 1.440, p = 0.246). Likewise, no significant difference in the mothers’ levels of confidence in caregiving abilities was found according to these variables. While changes in the level of caregiving behaviour were greater for mothers who were employed compared with those were not (t = 7.727, p = 0.013), no significant difference was found for other variables.
Table IV. Changes in mothers’ anxiety levels, caregiving efficacy, and caregiving behaviours by demographic characteristics (n = 20) after participating in the hybrid atopic dermatitis education programme
For this study, we developed a hybrid education programme for mothers of children with AD with the intention of reducing the mothers’ anxiety while improving their caregiving confidence and behaviours. The present study demonstrated a significant decrease in mothers’ mean anxiety score after taking part in our educational programme. This result is consistent with Kendall et al.’s (37) study that reported that a group-based parenting programme helped lower parents’ anxiety. Likewise, Pustišek et al. (38) reported a significant decrease in mothers’ anxiety and stress after participation in a parental education programme for parents of children with moderate to severe AD. Given that Ersser et al.’s (17) study revealing that educational interventions provided to individuals and groups by nurses or teams of dermatology specialists in hospitals or community settings, helped parents and children better understand the child’s condition, we may assume that our programme’s question-and-answer sessions, both offline and online, contributed to this significant reduction in anxiety because they allowed the mothers to directly consult dermatologists and nurses regarding their children’s condition.
Consistent with previous studies (15, 17, 19, 36, 39) that recommended an innovative, systematic approach for educating parents about how to properly care for their children’s AD, our intervention programme helped reduce mothers’ feelings of anxiety, while strengthening their caregiving efficacy to carry out actions to provide care for their children with AD. Kendall et al. (37) also indicated that mothers’ efficacy was correlated with their stress level and anxiety level, which was consistent with our findings. In addition, Mitchell & Fraser (40) showed a positive relation between caregiving efficacy for managing AD and self-reported task performance. Likewise, Morawska et al. (41) reported that improvement in parents’ caregiving efficacy regarding childhood chronic illness management was associated with improved child health outcomes, such as competence with treatment, and lower symptom severity (41). It has been reported that educational interventions positively affected mothers’ efficacy (30, 40, 41). Similarly, Son & Lim (42) suggested that a web-based education programme as an advanced intervention might be useful in improving mothers’ caregiving efficacy, knowledge of AD, and adherence to treatment.
In addition to efficacy, the mothers in our study significantly increased their caregiving behaviours after participating in the 8-stage hybrid educational programme. Consistent with our findings, a similar study by Jang et al. (43) also indicated that mother’s AD-management behaviours were significantly influenced after they increased their knowledge of the condition and shared their experiences of AD during an educational programme designed to help them manage their children’s AD. These findings mirror those of Aga et al. (44) and Bes et al. (45), who showed that caregiving behaviour increased after the implementation of health education programmes for mothers.
Thus, our findings indicate that this hybrid educational programme for mothers of children with AD proved effective in reducing their anxiety, improving their caregiving efficacy, and increasing the caregiving behaviours performed by the mothers. This programme can be used by nurses in practice while treating atopic children in the hospital and educating parents about home-based care for their children after discharge. Our flexible, easy-to-implement programme can be efficiently used by nurses who often feel rushed or hurried when providing patient education. This programme can also be used by school nurses responsible for communicating with parents and providing health education.
This study has some limitations. First, the participants were all mothers of atopic children living in urban areas in South Korea, thus the results do not reflect the situation in rural areas or in other countries. Therefore, it is suggested that further studies examine children and mothers nationwide and globally. Secondly, the study identified the effects of the AD education programme on a single group, thus further studies with a control group are warranted. Lastly, while subgroup analyses were conducted in this study, these were not powered, owing to very small groups. Despite these limitations, the hybrid educational programme for the targeted population reduced anxiety, improved caregiving efficacy, and enhanced caregiving behaviour among mothers. It would be worth exploring whether mothers’ results are related to the severity of their child’s AD. A comparison study to assess the specific impact of each online and offline programme component of the hybrid programme may also be beneficial. Based on our results, we expect that similar programmes will be directed towards other populations and illnesses in the future. Healthcare providers and educators should consider examining the long-term effects of the hybrid education programme for this population.


 Click to show fullsize
Click to show fullsize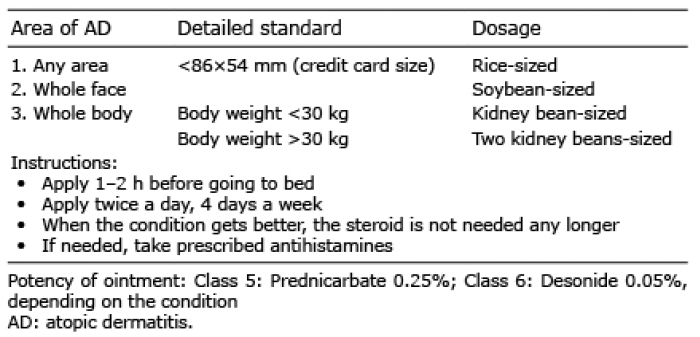 Click to show fullsize
Click to show fullsize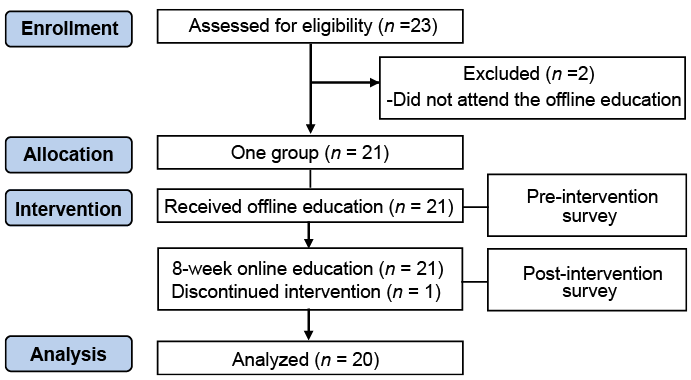 Click to show fullsize
Click to show fullsize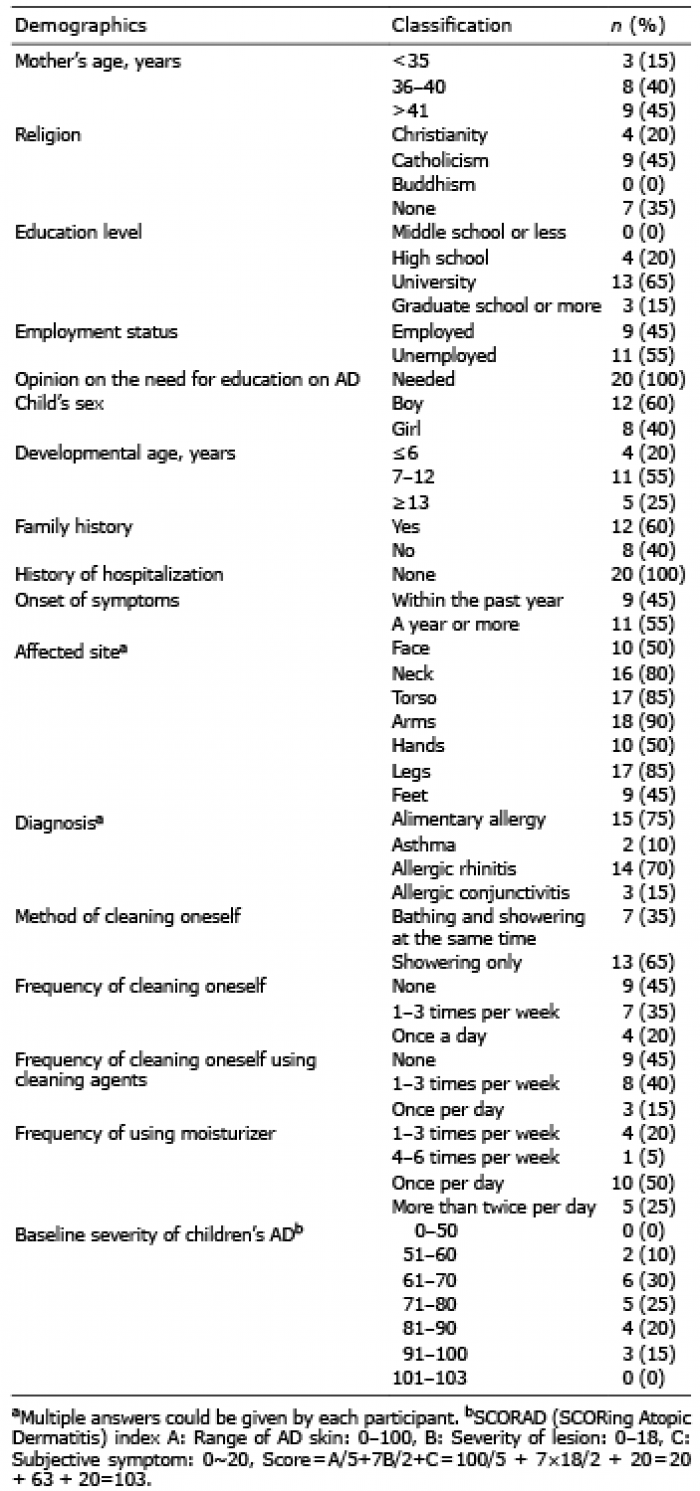 Click to show fullsize
Click to show fullsize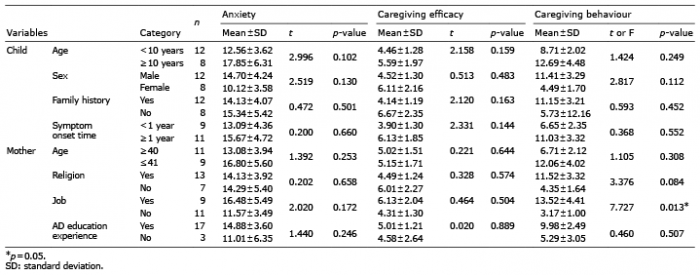 Click to show fullsize
Click to show fullsize