


Department of Dermatology, University Hospital Jena, University Hospital Jena, Jena, Germany
Sarcoidosis is a systemic non-caseating granulomatous disease of unknown aetiology. Cutaneous manifestations are present in approximately 10–30% of the patients with the systemic form. Therapy is indicated in case of disabling symptoms, organ dysfunction or cosmetically distressing manifestation. Despite different therapeutic possibilities, cutaneous sarcoidosis remains exceptionally difficult to treat. Light and laser therapy may be a promising alternative. In this systematic review, we summarised the available treatments according to the literature concerning light and laser therapy for cutaneous sarcoidosis. Publications written in English and German, published between January 1990 and July 2016 in the database PubMed, MEDLINE, Embase, and Scopus were analysed. Light therapy with intense pulsed light, photodynamic therapy, and ultraviolet A light therapy, as well as laser therapy with pulsed dye laser, YAG laser, and Q-switched ruby laser were described. The results are based on individual case reports and small case series. Randomised controlled studies are lacking.
Key words: cutaneous sarcoidosis; treatment; light therapy; laser therapy.
Accepted Dec 15, 2017; Epub ahead of print Dec 15, 2017
Acta Derm Venereol 2018; 98: XX–XX.
Corr: Ana Luiza Lima, Department of Dermatology, University Hospital Jena, Erfurter Straße 35, DE-07743 Jena, Germany. E-mail: Ana.Lima@med.uni-jena.de
Sarcoidosis is an idiopathic, non-caseating granulomatous disorder that may affect various organs (1). Many patients are asymptomatic; however, in a small group of patients the disease can be devastating and fatal.
The lungs are affected in more than 90% of the patients with sarcoidosis, followed by lymph node, cutaneous, and ocular manifestations (2). Skin involvement is present in about 10–30% of patients with sarcoidosis and often occurs at the onset of the disease (2, 3).
Half of all patients with sarcoidosis undergo spontaneous healing within 2 years (2). Treatment is indicated in case of disabling symptoms, organ dysfunction or cosmetically distressing manifestation (4).
Despite different therapeutic possibilities, cutaneous sarcoidosis (CS) remains exceptionally difficult to treat, presenting a variable response to the standard therapies (5). Light and laser therapies have been proposed as a promising alternative for therapy-resistant cases of CS and for refractory lesions. This article systematically reviews the use of physical modalities in the treatment of CS.
This systematic review was conducted in September 2016 based on literature from PubMed, MEDLINE and Embase. The search was restrained to reports published between January 1, 1990 and July 31, 2016 in English and German language. The terms ‘(phototherapy) AND (cutaneous sarcoidosis)’, and ‘(laser) AND (cutaneous sarcoidosis)’ were used for searching in PubMed. The articles were also cross-referenced with the Scopus database. Manual search of the references from retrieved articles was also performed.
In the initial search, a total of 31 articles were found. Reviews, duplicated papers and papers that did not discuss the treatment of CS were excluded, reducing the number of articles to 14. Six additional articles were included through manual search, to give a final total of 20 reports for analysis.
A total of 11 reports (17 patients) on light therapy treatment of CS were found (Table SI).
Six patients underwent treatment with topical gel psoralen 0.005% and UVA (PUVA) (6). Three patients had a complete response and the other 3 showed a 50% improvement of the lesions. The therapy was well tolerated and showed no adverse side-effects.
The two cases treated with UVA1 showed a therapy-resistant sarcoidosis (7, 8). One patient underwent nearly complete healing of all lesions and the other a considerable improvement in the lesions. UVA1 therapy was well tolerated.
A total of 7 patients were treated with photodynamic therapy (9–14). For 5 patients topical aminolevulinic acid (ALA) was used as photosensitizer. Two further patients were photosensitized with topical methyl aminolevulinate. Adverse effects described were: burning and prickling sensation, erythema, oedema, hyperpigmentation; and superficial desquamation.
Two case reports analysed the efficacy of intense pulse light (IPL) in the therapy of CS (15, 16). In one case, the patient experienced marked improvement (15). The second case was extracted from a case series with 10 patients with different dermatological diseases, which were treated unconventionally with IPL. The pain disappeared and a significant reduction of the vascular component and the consistency of the lesions was achieved. The therapy was well tolerated without side-effects.
A total of 11 CS patients were treated with laser therapy (see Table SI).
Five single case reports analysed the efficacy of pulsed dye laser on the therapy of CS (17–21). Two other case reports described the use of YAG laser and Q-switched ruby laser by patients with refractory disease after PDL therapy (22, 23). Most patients archived a dramatic improvement of the lesions. Relapse was described in one case, in which the majority of the erythema and papules returned after 15 months (17). Ekbäck & Molin (22) reported a limited effect of PDL. Similarly, Grema et al. (23) described a failure of PDL therapy.
A total of 4 patients were treated with CO2 laser (24, 25). Stack et al. (24) described the complete improvement of lesions in a patient with refractory disease after CO2 laser therapy. The most recent report described 3 cases with lupus pernio treated with CO2 laser (25). One case experienced a partial recurrence after reduction of oral corticosteroid (25). Subtle hypopigmentation was described as adverse effect in one case (25).
As described above, YAG laser and Q-switched ruby laser were used in patients with refractory disease after PDL therapy (22, 23). The sessions of Q-switched ruby laser were well tolerated and the lesions healed without recurrence (22). The patient treated with YAG laser showed complete clearance of the lesions. Slight erythema and swelling of the treated skin were described as adverse side-effects (23).
In a summary of Table SI, UVA phototherapy in the form of topical PUVA (6 cases) or UVA1 radiation (2 cases) improved the CS lesions. PUVA-treated patients underwent a complete remission in 3 patients and a 50% improvement of the lesions in the other 3 patients (6). UVA1 was used in localised and disseminated disease, resulting in improvement in the lesions in both cases (7, 8). The therapy was well tolerated and may be a good alternative in cases of disseminated CS.
Seven patients were treated with photodynamic therapy (9–14). ALA was the most commonly used photosensitizer (9, 12–14). All reports showed significant improvement in the lesions and just one case recurred after 3 months (12). Photodynamic therapy has a considerable effect; however, various side-effects, such as hyperpigmentation, desquamation, headache, burning and prickling sensation, erythema, and oedema were described (9, 3).
Two case reports analysed the efficacy of IPL in CS (15, 16). Solely localised CS lesions were treated. The patients experienced considerable improvement.
PDL was the most commonly used laser therapy (17–21). Most patients achieved a remission of their cutaneous lesions. However, PDL showed limited effect in 2 cases as well as no response in one case (17, 22, 23). YAG laser and Q-switched ruby laser were used in patients with refractory disease, resulting in complete remission of the lesions.
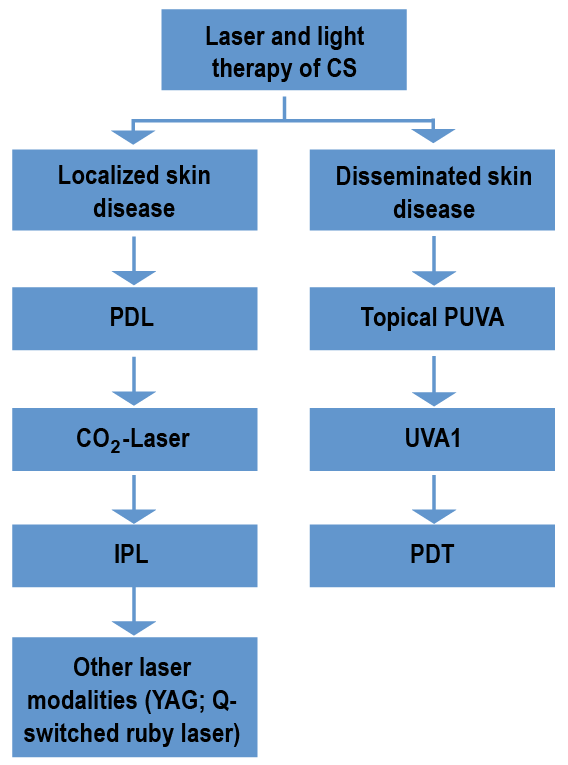
Two reports analysed the CO2 laser as therapy option for CS (24, 25). All patients treated showed an improvement in the lesions, and one patient showed a partial recurrence after reduction in the systemic corticosteroid. Hypopigmentation was described as an adverse side-effect (25). These results are based on individual case reports and small case series, thus lacking study-based evidence. Based on the current review, we suggest an algorithmic approach (Fig. 1) to CS therapy.
Systematic clinical studies on the treatment of CS are needed, but they are difficult to perform due to the rarity of the condition. In the meantime, case reports and case series on successful (and unsuccessful) treatment approaches in patients with CS should be published to broaden the available medical database.
The authors have no conflicts of interest to declare.
Fig. 1. Suggested algorithm for sarcoidosis light and laser therapy based on the number of patients treated, therapy success, relapse, and adverse side-effects. This approach is based on individual case reports and small case series, having limits in terms of lack of evidence. CS: cutaneous sarcoidosis; PDL: pulsed dye laser; IPL: intense pulsed light; YAG: yttrium aluminium garnet laser; topical PUVA: topical gel psoralen 0.005% and ultraviolet A; PDT: photodynamic therapy.


 Click to show fullsize
Click to show fullsize