


1Department of Dermatology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Dongcheng District, Beijing 100730, China, and 2Department of Dermatology, University of Colorado Anschutz Medical Campus, Aurora, CO, USA. *E-mail: zengyueping0917@126.com
Accepted Dec 14, 2017, E-pub ahead of print Dec 15, 2017
Indeterminate cell histiocytosis (ICH) is a rare disease characterized by the proliferation of histiocytic cells derived from indeterminate dermal cells. The clinical features of ICH include solitary or multiple, asymptomatic, papules and nodules on the trunk and extremities. In some cases, ICH presents as a generalized eruption. We report here the case of a patient with ICH who presented with “leonine facies”.
A 31-year-old Chinese man presented with a 4-year history of progressive, asymptomatic, scattered, skin-coloured and erythematous papules and nodules. The skin lesions initially appeared on the left cheek, spreading to his right cheek, trunk, and extremities. He did not report any preceding illness or associated constitutional symptoms, such as weight gain/loss, fevers, chills, night sweat, coughs, or chest pain. He had no personal or family history of skin rashes. The skin lesions regressed spontaneously over the subsequent 42 months without any treatment, leaving atrophic scars. Two months prior to his initial visit to our clinic, he experienced a recurrence of his skin lesions.
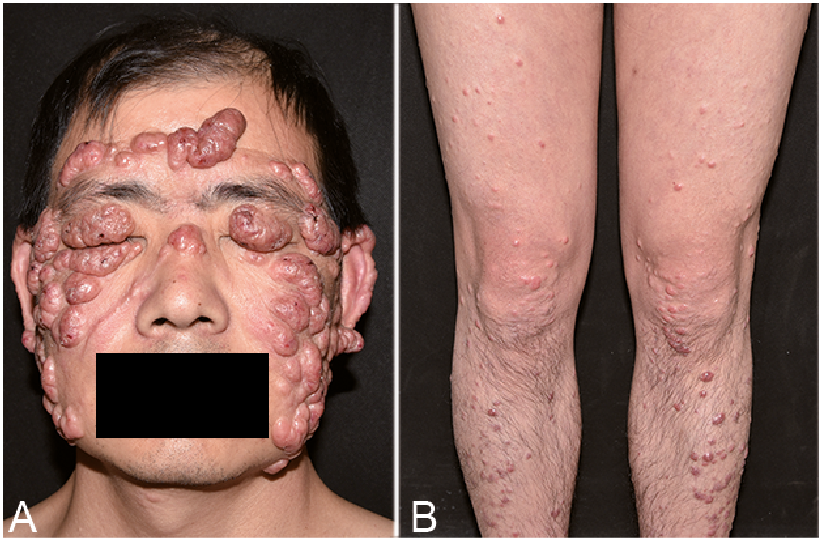
Dermatological examination revealed skin-coloured and ery-thematous, soft papules and nodules on his face and both auricles resembling “leonine facies” (Fig. 1A). The lesions ranged from 5 to 40 mm in diameter. There were similar lesions on the patient’s lower and upper extremities (Fig. 1B), but his back was relatively spared. A peripheral blood count, urinalysis, serum electrolytes, antinuclear antigen, rheumatoid factor, and tumour markers including carcinoembryonic antigen, and squamous cell carcinoma were within normal limits. The patient had a modestly elevated aspartate transaminase, lactate dehydrogenase, triglycerides, and an erythrocyte sedimentation rate. Abdominal sonography revealed a fatty liver. A chest X-ray was normal.
Fig. 1. Clinical features. (A) The patient gradually developed asymptomatic papules and nodules on both cheek and auricles, as “leonine facies”. (B) Clinical photograph of erythematous papules on the lower limbs. Written permission from the patient is given to publish these photos.
A punch biopsy revealed a well-defined Grenz zone with no evidence of histiocytic epidermotropism. A dense dermal infiltrate of histiocytes admixed with lymphocytes was present without eosinophilic infiltration. The histiocytes had abundant eosinophilic cytoplasm with vesicular nuclei. The nuclei of some histiocytes appeared coffee-bean or kidney shaped (Fig. 2A). The histiocytic cells were immunohistochemically reactive for CD1a (Fig. 2B), CD163, and CD68, and partly positive for S-100 protein; cells were negative for langerin. Acid-fast and Periodic Acid-Schiff staining were negative.
Fig. 2. (A) Punch biopsy revealed a well-defined Grenz zone, and a dense dermal infiltration of histiocytes and lymphocytes; (A, insert) nuclei of some histiocytes were coffee-bean shaped (yellow arrow) or kidney shaped (white arrow) (haematoxylin and eosin (H&E) stain, bar = 20 μm). (B) Immunohistochemical studies demonstrated that the histiocytes were strongly positive for CD1a (streptavidin peroxidase (SP) staining, bar = 400 μm).
The constellation of skin morphology, histology, and immunophenotypic findings were compatible with ICH. Methotrexate (MTX), 15 mg weekly, was recommended. No improvement was seen at his follow-up visit. Given the lack of response to MTX, daily isotretinoin 30 mg and thalidomide 75 mg were recommended. The patient noted improvement in his skin, and remains under close observation in our clinic.
Wood et al. (1) first drew attention to ICH in 1985. Classically, skin lesions are found on the trunk and extremities, or are in a generalized distribution. Extracutaneous and systemic involvement in ICH are exceedingly uncommon. Pathological features include positivity for S-100 and CD1a antigens, and negativity for intracytoplasmic Birbeck granules.
The current case is of particular interest because of its unique morphology and cutaneous presentation. Leonine facies are rare (2), and are more frequent in association with lepromatous leprosy (3), cutaneous T-cell lymphomas (4, 5), lichen myxoedematosus (LM) (6), and pachydermoperiostosis (7) (Table I). Clinical and histopathological features can help to differentiate these conditions from ICH (8–11).
Table I. Differential diagnoses of disorders presenting with leonine facies
Other mimickers of ICH include granulomatous diseases, such as Langerhans cell histiocytosis (LCH), xanthoma disseminatum, Rosai-Dorfman disease (RDD), and sarcoidosis. ICH shares morphological and immune-phenotypic features with both LCH and non-LCH. LCH is characterized by granulomatous lesions composed of clonal pathological histiocytes, with the most common affected sites being pulmonary, osseous, central nervous system, and skin (12). The cutaneous presentation is highly variable and includes dry scaly involvement, erythematous rashes, or diffuse red-to-purple papules on the limbs, chest, and back. In contrast, ICH is typically associated with papules on the extremities. Birbeck granules are seen in LCH, but not in ICH. Immunohistochemical positivity for S-100 and CD1a are seen in ICH, but usually not in non-LCH, such as xanthoma disseminatum. RDD does not express CD1a or langerin, but the S100-positive histiocytes are often multinucleated with obvious emperipolesis (13). Sarcoidosis, finally, is a multi-systemic disease of unknown cause characterized by the formation of non-caseating granulomas in involved organs (14).
In summary, ICH is a rare histiocytic disorder with a variable clinical course, although it is generally considered benign. The current case highlights the unusual presentation of ICH as “leonine facies” and the utility of using immunohistochemical markers to help establish a definitive diagnosis.
This study was supported by the National Natural Science Foundation of China (81602765), the Beijing Natural Science Foundation (7174340), and the Young scientific research fund of Peking Union Medical College Hospital (pumch-2016-2.12).


 Click to show fullsize
Click to show fullsize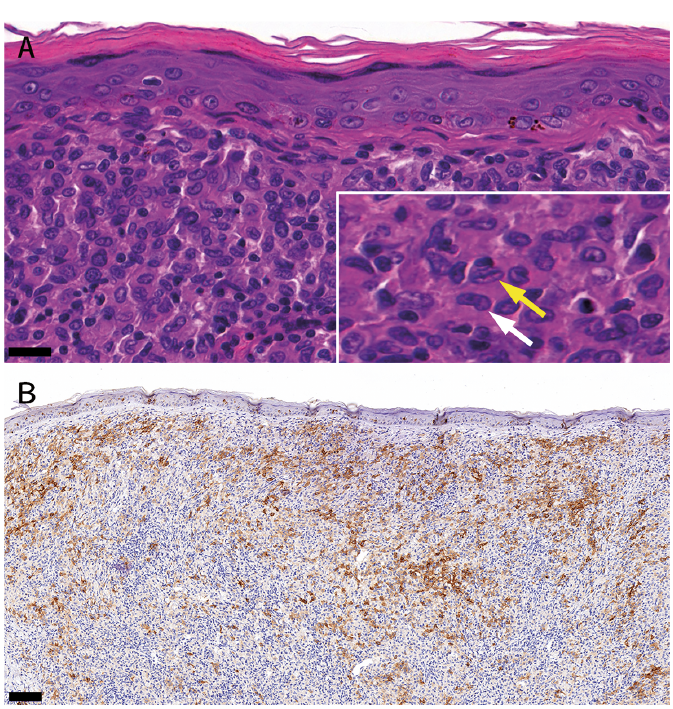 Click to show fullsize
Click to show fullsize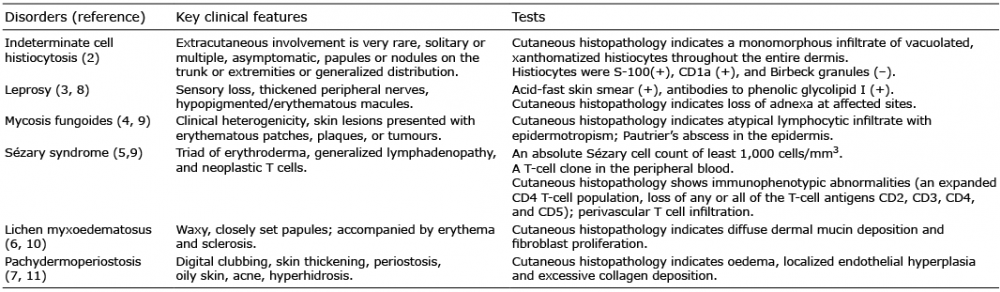 Click to show fullsize
Click to show fullsize