


1Department of Dermatology, Faculty of Medicine and Graduate School of Medicine, Hokkaido University, North 15 West 7, Kita-ku, Sapporo 060-8638, Departments of 2Dermatology and 3Respiratory Medicine and Allergology, Kushiro City General Hospital, Kushiro and 4Department of Cancer Chemotherapy, Hokkaido University Hospital Cancer Center, Sapporo, Japan. *E-mail: nishie@med.hokudai.ac.jp
Accepted Dec 20, 2017; Epub ahead of print Dec 20, 2017
Ramucirumab is a fully human IgG1 monoclonal antibody that selectively binds to the extracellular domain of vascular endothelial growth factor receptor 2 (VEGFR-2). Ramucirumab is mainly used as a second-line treatment for advanced cancers, such as gastric, colorectal and non-small-cell lung cancers (1–4). Various adverse events due to ramucirumab have been reported, including hypertension, deep vein thrombosis, headaches, anorexia, vomiting and dyspnoea (5). Tanibirumab and alacizumab, which are reagents targeting VEGFR-2, are known to induce haemangiomas as a paradoxical reaction (6, 7); however, only 2 cases of multiple haemangiomas associated with ramucirumab have been reported in a phase I study (CP12-0401), and these had no detailed clinical or histopathological descriptions (8). Moreover, tanibirumab and alacizumab are not commercially available. Therefore, we clinicians have limited opportunity to observe this phenomenon. We report here 2 cases of ramucirumab-induced multiple haemangiomas of the skin.
Case 1. A 61-year-old woman presented to our department with multiple reddish macules over the body. She was on FOLFIRI (5-fluorouracil, leucovorin, irinotecan) and ramucirumab treatment as a second-line chemotherapy for refractory metastatic caecal adenocarcinoma. Eighteen months earlier, caecal adenocarcinoma with multiple liver metastases had been found and she had received mFOLFOX6 (oxaliplatin, 5-fluorouracil (5-FU), folic acid) plus bevacizumab therapy. After 5 cycles of the regimen, she had undergone a right hepatic and caudal lobectomy. New liver metastases were found 5 months after the operation, and mFOLFOX6 plus bevacizumab treatment was re-started. Unfortunately, the metastatic lesion of the liver enlarged and the treatment was changed to FOLFIRI plus ramucirumab. Two months after the treatment, reddish papules developed.
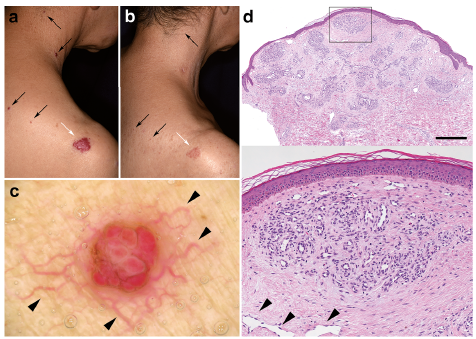
Physical examination revealed numerous reddish papules approximately 2–3 mm in diameter on the scalp, neck, trunk and limbs (Fig. 1a, b). There was a slightly elevated red macule of 30×20 mm on the right shoulder (Fig. 1a). Dermoscopy revealed red homogenous globules surrounded by telangiectasia (Fig. 1c). Histopathological findings of the skin specimen obtained from a red papule on the neck revealed local proliferation of vascular endothelial cells in the superficial dermis (Fig. 1d). Enlarged capillary vessels and fibrosis surrounding the endothelial cells were also observed (Fig. 1d). We made a diagnosis of capillary haemangioma, and the other lesions were not removed. The FOLFIRI plus ramucirumab therapy was switched to panitumumab because of severe neutropaenia. Approximately 3 months after discontinuing the treatment, the haemangiomas disappeared gradually (Fig. 1b).
Fig. 1. Clinical and histopathological characteristics of case 1. (a) Sporadic reddish papules approximately 2–3 mm in diameter are seen on the neck and right shoulder (black arrows). There is also a slightly elevated red macule measuring 30×20 mm on the right shoulder (white arrow). (b) Three months after the cessation of FOLFIRI (5-fluorouracil, leucovorin, irinotecan) and ramucirumab. Note the haemangioma has spontaneously regressed. (The lesion of the right neck has been excised.) (c) Dermoscopy shows red homogenous globules surrounded by telangiectasia (arrowheads). (d) The skin specimen of the red papule on the neck shows local proliferation of vascular endothelial cells in the superficial dermis. Enlarged capillary vessels (arrowheads) and fibrosis surrounding the endothelial cells are also seen. Scale bar: 200 μm.
Case 2. A 65-year-old woman presented to our department with slowly growing nodules on the limbs and the face. She had been receiving docetaxel and ramucirumab as a second-line therapy for refractory metastatic lung adenocarcinoma for 2 months. Three years earlier, she had been diagnosed with lung adenocarcinoma with bone metastasis of the right sixth rib and thoracic vertebrae. The patient had received radiation (total dose: 30 Gy) to the right rib, and thoracic vertebrae and afatinib was started. One month later, the afatinib was changed to gefitinib due to drug-related ileus. One year later, carboplatin and pemetrexed were started because of metastasis to the skull. Unfortunately, cerebellar metastasis was found after 3 cycles of the regimen, which was discontinued; radiation to the cerebellum was started. Thereafter, she was treated with docetaxel and ramucirumab. Two months after the start of treatment, she noticed painful, slowly growing papules and nodules on the left groin and face.
Physical examination revealed easily bleeding, painful reddish papules and nodules of 3–10 mm on the right lateral canthus and the left inguinal area (Fig. S1a, b). Multiple reddish papules approximately 1 mm in diameter were also observed on the face, trunk and limbs (Fig. S1c). Histopathological analysis of the lesions showed the nodular proliferation of vascular endothelial cells with marginal fibrosis (Fig. S1d, e). The nodular lesions macroscopically and microscopically resembled pyogenic granuloma, except for the presence of enlarged capillary vessels in the upper dermis beneath the lesion (Fig. S1d, e). We made a diagnosis of pyogenic granuloma-like haemangioma. The patient is currently still under docetaxel and ramucirumab therapy, and similar reddish papules are increasing in size and numbers. Some of the painful lesions have been surgically removed.
We report here 2 cases of ramucirumab-induced multiple haemangiomas of the skin that were probably induced by a paradoxical reaction. The patients had no history of drug treatments that have been reported to induce multiple haemangiomas as adverse events, except for ramucirumab. Although the aetiology remains uncertain, previous studies have revealed that vascular tumours may arise under therapies targeting VEGFR-2. Ton et al. reported 7 cases of haemangiomas in a phase I evaluation of the VEGFR-2 inhibitor alacizumab (CDP791) (6). The lesions were roundly elevated reddish papules of 5–10 mm in diameter, which histologically showed proliferated vascular endothelial cells with proliferation of the vessels in the superficial dermis. Neither patient developed skin toxicity that would have required discontinuation of the alacizumab, and the haemangiomas resolved upon cessation of alacizumab therapy. Similar haemangiomas were also observed in a phase I study of the new VEGFR-2 inhibitor tanibirumab (7). Surprisingly, more than half of the patients (16 out of 26: 61.5%) who received tanibirumab treatment developed haemangiomas in that study. As in the cases of alacizumab (6), the haemangiomas disappeared after discontinuation of the tanibirumab (7). Notably, the haemangiomas of the first case in the present report also disappeared after the cessation of ramucirumab therapy.
The aetiology of paradoxical reactions to anti-VEGFR-2 therapies remains unknown. Regarding the aberrant roles of VEGFR-2 signalling due to the reagents, it has been reported that the haemangiomas showed little internalization of VEGFR-2 in the phase I study of alacizumab, suggesting that the angiogenesis may be independent of VEGFR-2 signalling (8). It is known that somatic gene mutations in VEGFR-2 can be associated with the development of angiosarcomas (9) and juvenile haemangiomas (10). Consistent with this, a case with somatic gene mutation in VEGFR-2 in a ramucirumab-induced haemangioma has been reported (11). However, it is uncertain whether somatic mutations in VEGFR-2 were involved in the current cases.
In addition to the proliferation of endothelial cells, the present cases were characterized by telangiectasia observed by dermoscopy in addition to the histopathological findings. Telangiectasia is uncommon in other haemangiomas; therefore, this finding may be distinct in ramucirumab-induced skin haemangiomas, which involves increased angiogenesis.
In conclusion, ramucirumab can cause multiple haemangiomas of the skin. Clinicians should be aware of this angiogenesis under anti-VEGFR-2 therapies.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize