


1Department of Dermatology, Chelsea and Westminster Hospital, SW109NH London, and 2Department of Histopathology, Charing Cross Hospital, London, UK. E-mail: emilyclairerudd@hotmail.com
A 31-year-old woman presented to the dermatology clinic with a two-month history of a pruritic rash on her left flank. The rash erupted as a single erythematous papule and, within days, progressed into multiple papules in a linear distribution. She reported no fever, haematuria or gastrointestinal symptoms. Her past medical history and medication history were unremarkable. On further enquiry she had swum in Lake Malawi two years previously. At that time she did not recollect having a rash or flu-like symptoms. Physical examination revealed firm erythematous papules on the left flank in a linear distribution. A cluster of subcutaneous nodules were palpable adjacent to the rash (Fig. 1). Routine blood tests showed normal full blood count, renal and liver biochemistry and inflammatory markers. A diagnostic skin biopsy was taken (Fig. 2).
What is your diagnosis? See next page for answer.
Fig. 1. Clinical photographs of rash.
Fig. 2. Skin biopsy (amplification x120).
Acta Derm Venereol 2018
Diagnosis: Cutaneous schistosomiasis
The diagnostic skin biopsy shows a cluster of Schistosoma spp. ova in the dermis with surrounding necrobiosis and granulomatous tissue. There is peripheral palisading of lymphocytes and histiocytes in the dermis (Fig. 2). Some of the Schistosoma spp. ova have clearly identifiable terminal spines indicative of S. haematobium (Fig. 3). Ziehl Nielson stain was positive. Gram stain and culture were negative. Schistosomal serology was positive. Four urine and stool samples showed no evidence of ova on microscopy. A CT abdomen-pelvis showed no lymphadenopathy and no bladder or kidney abnormalities.
This is a case of isolated cutaneous schistosomiasis which presented two years after exposure. There was no evidence of visceral involvement. The patient responded well to standard treatment; two doses of praziquantel 20 mg/kg 6 hours apart.
Schistosomiasis is caused by infection with parasitic flatworms of Schistosoma species. The disease is otherwise known as bilharziasis after Theodore Bilharz who identified the parasite in 1852. An estimated 200 million people are infected with schistosomiasis worldwide (1).
There are 3 main species that can cause infection in humans: S. haematobium, S. manosoni and S. japonicum. S. haematobium is found mainly in Africa and the Middle East and causes urinary disease; presenting usually with haematuria and dysuria. S. mansoni is found mainly in Africa, South America and Caribbean. S. japonicum is mainly seen in East Asia. Both S. mansoni and S. japonicum cause intestinal and hepatosplenic schistosomiasis.
Chronic cutaneous manifestations are rare, particularly in the absence of visceral involvement (2). They are most frequently caused by S. haematobium. Most published cases of cutaneous schistosomiasis involve the genital and peri-genital sites (including anus and perineum), presenting as hypertrophic, erosive or vegetative lesions (3).
Ectopic or extragenital lesions are extremely rare, even in endemic areas. The first case of extragenital cutaneous schistosomiasis was described in 1941 by El Mofty (4) in a 17-year-old male who was infected with S. hematobium in his urinary tract. Typically the rash affects the trunk and consists of single or clusters of itchy skin-coloured papules (5). A peri-umbilical or zosteriform distribution are most frequently seen (6). Ectopic cutaneous schistosomiasis is most commonly associated with S. haematobium (5).
The clinical diagnosis of cutaneous schistosomiasis can be difficult, particularly in non-endemic areas. Clinical manifestations can present months to years after exposure to the pathogen. Biopsy findings of schistosomal ova in the dermis are required for diagnosis. The species of schistosome can be identified by the location of the ova spine; S. haematobium has a terminal spine whereas S. mansoni has a lateral spine (7). In older lesions, there is disintegration of the eggs on histology; multiple layers are often required to identify ova among dense connective tissue (8). Positivity of the Ziehl Nielson stain appears to be unreliable in determining the species of schistosome (6).
The mechanism of ova deposition is not well understood. Faust postulated that anastamoses between venous systems allow adult worms or ova to migrate to ectopic sites (9). In relation to the peri-umbilical distribution of the rash, Macdonald & Morrison (6) suggest that the likely route is from the portal circulation via the left portal vein to the paraumbilical veins where there is an anastomosis with the superficial and deep epigastric veins of the caval system.
Cutaneous schistosomiasis presents a clinical diagnostic challenge. This case highlights the cutaneous signs and pathological features of isolated ectopic cutaneous schistosomiasis. Clinicians should be aware of the condition as, if left untreated, S. haematobium can cause significant morbidity, and bladder cancer is a recognised complication of visceral disease.
Fig. 3. Skin biopsy (amplification x480, Ziehl Neelsen stain): Terminal spines indicative of Schistosoma haematobium.


 Click to show fullsize
Click to show fullsize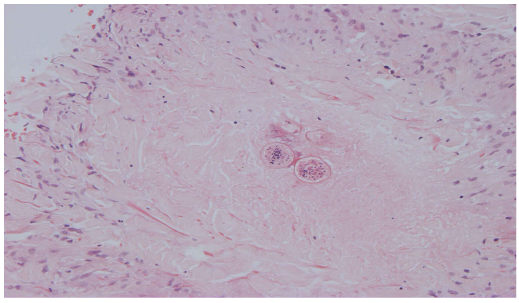 Click to show fullsize
Click to show fullsize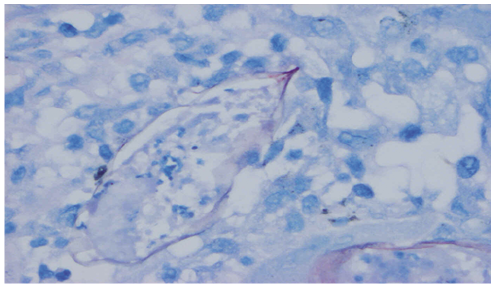 Click to show fullsize
Click to show fullsize