


Department of Dermatology, Saitama Medical Center, Saitama Medical University, 1981 Kamoda, Kawagoe, Saitama 350-8550, Japan. E-mail: teraki@saitama-med.ac.jp
Accepted Dec 20, 2017; Epub ahead of print Dec 20, 2017
The interleukin (IL)-17A inhibitors, secukinumab and ixekizumab, are successfully used for the treatment of psoriasis and psoriatic arthritis (1–3). Both secukinumab and ixekizumab have favorable safety profiles, although various adverse events have been reported in patients treated with IL-17A inhibitors (4–6). Common adverse events after using IL-17A inhibitors include nasopharyngitis, headache, upper respiratory infection, pruritus, and injection site reactions. Mucocutaneous candidiasis and neutropenia are more common in patients treated with IL-17A inhibitors than in those treated with tumor necrosis factor-α and IL-12/23 inhibitors. However, little is known about eyelid dermatitis following therapy with IL-17 inhibitors (4–6). Here, we report 3 cases of eyelid dermatitis following therapy with IL-17A inhibitors for patients with psoriasis.
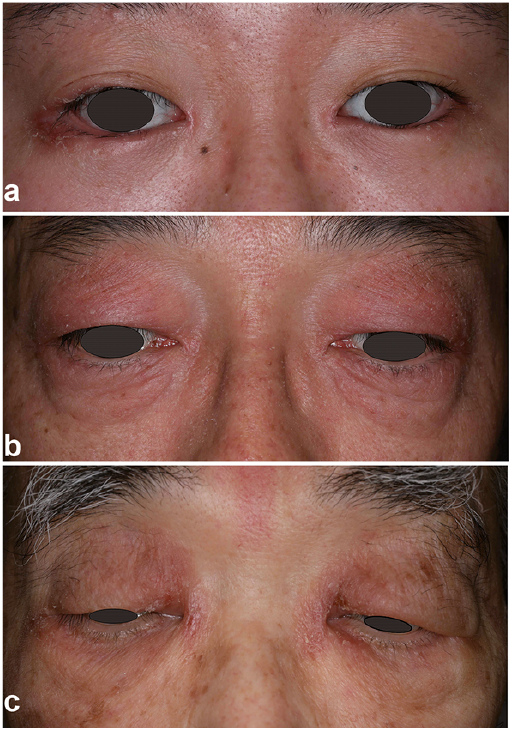
Case 1. A 33-year-old woman was referred to our dermatology clinic with a psoriatic arthritis. The patient had a 20-year history of plaque psoriasis on the scalp and extremities and developed arthralgia on the right ring finger and right 4th toe 2 months earlier. The psoriasis area and severity index (PASI) was 3.0 and disease activity score 28-C-reactive protein value was 3.2. The patient had been treated with 300 mg secukinumab at weeks 0, 1, 2, 3, and 4, followed by 300 mg every 4 weeks. Treatment with secukinumab resulted in rapid remission of both psoriatic lesions and arthritis. The patient developed eyelid dermatitis 3 months after the initiation of secukinumab therapy. The patient did not use any eye drops and eyelid cosmetics. A physical examination revealed erythematous lesions with flaking scales on the eyelid margins and scaling on the eyelashes (Fig. 1a). Neither itching nor conjunctivitis was observed. Potassium hydroxide examination of the scales did not reveal any fungal elements. Treatment with topical corticosteroids did not improve eyelid lesions. Finally, the eyelid dermatitis resolved after discontinuation of secukinumab.
Fig. 1. Clinical features. a) Case 1. Erythematous lesions with flaking scales on the eyelid margins and scaling on the eyelashes, which developed 3 months after the initiation of secukinumab for treating psoriatic arthritis. b) Case 2. Erythematous lesions with scaling and mild lichenification on the eyelids, which developed 4 months after the initiation of secukinumab for treating plaque psoriasis. c) Case 3. Scaly erythematous lesions with slight lichenification on the eyelids, which developed 4 months after the initiation of ixekizumab for treating pustular psoriasis.
Case 2. A 52-year-old man was referred to our dermatology clinic with a 15-year history of plaque psoriasis. A physical examination revealed psoriatic plaques on the trunk and extremities, with a PASI of 16.4. The patient had been treated with 300 mg secukinumab at weeks 0, 1, 2, 3, and 4, followed by 300 mg every 4 weeks. Treat-ment with secukinumab completely cured the psoriatic lesions within 3 months. At that time, the patient involved mild oral candidiasis, which was promptly improved by treatment with oral itraconazole. He developed eyelid dermatitis 4 months after the initiation of secukinumab therapy. An examination revealed erythematous lesions with scaling and mild lichenification on the eyelids (Fig. 1b). The patient had little itching. No relapse of psoriasis was found on the skin. Treatment with topical cortico-steroids improved eyelid lesions; therefore, secukinumab therapy was continued.
Case 3. An 89-year-old man was referred to our dermatology clinic with a 2-year history of psoriasis involving the trunk, extremities, and scalp. A physical examination revealed scaly diffuse erythema with pustules on the entire body. The PASI was 20.6. Skin biopsy revealed Kogoj’s spongiform pustules in the epidermis. The patient had been treated with 160 mg ixekizumab at week 0, and 80 mg at weeks 2, 4, 6, 8, 10, and 12, followed by 80 mg every 4 weeks. Treatment with ixekizumab promptly cleared all skin lesions except those on his legs, resulting in PASI 90 improvement within 2 months. The patient developed erythematous eruptions on the eyelids 4 months after the initiation of ixekizumab therapy. An examination revealed scaly erythematous lesions with slight lichenification on the eyelids (Fig. 1c). Treatment with topical corticosteroids improved skin lesions; therefore, ixekizumab therapy was continued. However, eyelid dermatitis frequently recurs after the cessation of topical corticosteroids.
The 3 present patients provided written informed consent for publishing the information.
In the 3 present cases, we demonstrated eyelid dermatitis in patients treated with the IL-17A inhibitors, secukinumab or ixekizumab, for psoriasis and psoriatic arthritis. In the 3 patients, eyelid dermatitis occurred 3–4 months after the initiation of secukinumab or ixekizumab treatment. Clinical features of eyelid lesions included ery-thematous eruptions with scaling on the eyelids or eyelid margins. No obvious conjunctivitis was observed in any patients. Eyelid dermatitis was improved by topical corticosteroids in 2 of the 3 patients; however, it frequently recurred in one patient. In one patient in whom dermatitis was localized on the eyelid margins, the lesions resolved after the discontinuation of IL-17A inhibitors.
Most cases of eyelid dermatitis are manifestations of endogenous diseases such as atopic dermatitis and psoriasis or the result of external exposure to the eyelids (7). However, the 3 patients did not have any history of atopic dermatitis and showed no relapse of psoriatic lesions on the skin when eyelid dermatitis occurred. They did not use any eye drops and eyelid cosmetics and did not complain of itching due to the eyelid lesions; therefore, allergic contact dermatitis can be excluded. Although the 3 patients did not have any history of seborrheic dermatitis on the face during the treatment period, seborrheic dermatitis of the eyelids or seborrheic blepharitis may be an important differential diagnosis.
The pathophysiology underlying eyelid dermatitis due to IL-17A inhibitors is unclear. The present cases suggest that eyelid dermatitis may be a class effect of anti-IL-17A rather than a drug-specific adverse event. IL-17 cytokines are critical for antimicrobial peptide production at the skin surface (8, 9). Therefore, IL-17A inhibitors reduce antimicrobial peptides, thereby leading to the overgrowth of microorganisms, such as Malassezia, which might contribute to the development of eyelid dermatitis. Little is known about eyelid dermatitis as a side effect of IL-17A inhibitors (4–6). In our department, IL-17A inhibitors have been used as treatment for 25 patients with psoriasis and 3 (12%) of the 25 patients developed eyelid dermatitis. Thus, eyelid dermatitis is a unique, not entirely rare, adverse event resulting from the use of IL-17A inhibitors. Physicians should pay attention to eyelid dermatitis as a side effect of IL-17A inhibitors.


 Click to show fullsize
Click to show fullsize