


1Department of Dermatology, Tel Aviv Medical Center, 6 Weizman Street, Tel Aviv 6423906, and 2Department of Human Molecular Genetics & Biochemistry, Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel. *E-mail: benofir@gmail.com
Accepted Dec 20, 2017; Epub ahead of print Dec 21, 2017
Oral antifungal medications are considered the gold standard therapy for onychomycosis. Topical antifungal treatments are less efficacious, mainly due to their limited penetration through the nail plate into the nail bed at fungicidal concentrations (1). In the last decade, the use of lasers and photodynamic therapy (PDT) has been used as an alternative treatment for onychomycosis, with varying clinical and microbiological results (1, 2). Pretreatment with ablative fractional lasers (AFR) increases the permeation and absorption of topical drugs and improves efficacy (3–8).
The aim of this study was to assess the efficacy of fractional ablative CO2 laser (FACL)-assisted delivery of 20% aminolaevulinic acid (ALA)-PDT and of 5% amorolfine (as nail lacquer) in achieving clinical and mycological cure of toenail onychomycosis.
This open-label comparative study included 60 patients, age range 18–60 years, with typical clinical finding and positive mycological culture of bilateral toenail onychomycosis. All participants provided written informed consent according to a protocol approved by the Tel Aviv Medical Center institutional review board in accordance with the prin-ciples of the Declaration of Helsinki. Exclusion criteria included: systemic antifungal treatment during the previous 12 months, concomitant nail disease, vascular or microcirculatory disorders, metabolic diseases, including diabetes mellitus, immunodeficiency states, paresis and paralysis caused by injuries to the central or peripheral nervous system, pregnancy, and porphyria, photosensitive dermatoses, and allergy to components of the photosensitizer compound for patients who were assigned to be treated with PDT. Patients who failed to comply with the treatment regimen and those who experienced discomfort and unusual side-effects due to the treatment were subsequently excluded.
All patients received 6 treatment sessions at 3-week intervals. The patients were randomly assigned to 2 study groups (groups A and B). Group A patients had 20%-ALA applied to the toenails and kept under occlusion using an opaque shield for 3 h. At the end of the incubation period, red light (630 nm) illumination was delivered from a non-coherent light source (Aktilite, Galderma) at a dose of 75 J/cm2. Group B patients’ toenails were painted with 5% amorolfine nail lacquer, and the patients were instructed to re-apply the nail lacquer once a week. Prior to undergoing PDT (group A) or the topical application of 5% amorolfine nail lacquer (group B), the toes of the right foot were pretreated with FACL (Lumenis, UltraPulse, Yokneam, Israel, Setting: SCAARFX mode. Energy: 150 mJ, density: 3%, one pass, small spot size). Prior to laser treatment, 5% EMLA cream (AstraZeneca AB, Södertälje, Sweden) was applied under occlusion to the infected nail and periungual skin for 60 min.
Standardized photographs and mycological cultures were obtained at baseline and at 3 months (first follow-up) and 9 months (second follow-up) after the final treatment. All toenails were photographed with a digital camera (Canon EOD 70D) using a 100-mm macro objective and ?ash (Canon Macro 100 mm). The baseline and follow-up photographs were compared by 2 dermatologists using a 0–5 grading scale (8), where: 5 = complete response (fully normal-appearing nail measured from the proximal nail fold to involved nail), 4 = very significant response (> 75% normal-appearing nail, compared with the area of the initially infected nail), 3 = significant response (50–75% normal-appearing nail), 2 = moderate response (25–50% normal-appearing nail), 1 = small improvement (< 25% normal-appearing nail), and 0 = no response to treatment. The dermatologists were blinded to the study groups and to the side of treatment. The first toe was evaluated if it was infected on both sides. If not, the other toes were evaluated.
At each treatment session the patients were asked to evaluate any treatment-related pain using a 10-cm visual analogue scale, from 0 (no pain) to 10 (extremely painful). At the 2 follow-up visits, they indicated their degree of satisfaction using the 5-point Likert scale: 5 = very satisfied, 4 = satisfied, 3 = neither satisfied nor dissatisfied, 2 = dissatisfied, and 1 = very dissatisfied.
Continuous measurements were summarized using means ± standard deviations (SD), and categorical measurements were summarized using counts and percentages. Comparisons of continuous measurements between the 2 study groups were carried out using the independent t-test. Comparisons of categorical measurements were performed using the Fisher’s exact test. The McNemar’s test was used for paired analysis between sides within the study groups. Significance was defined as p = 0.05. The analyses were carried out using SPSS 24.01.
A total of 60 patients were enrolled in the study, of whom 56 (30 in group A and 26 in group B), whose mean age was 49 years (range 26–66 years), completed the study. Four patients dropped out due to lack of compliance. The mean disease duration was 11.7 years. Most of the patients (73%) had severe onychomycosis. The mean onychomycosis severity index (OSI) score (9) was 23.6. Fungal cultures revealed Trichophyton rubrum in the majority (94.6%) of patients.
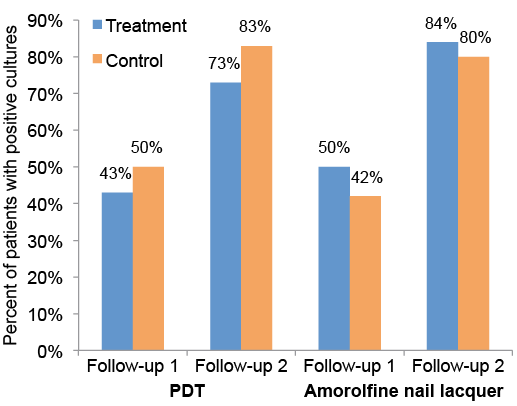
A comparison of the percentages of positive fungal cultures at the 2 follow-up visits revealed no significant differences between the treatment and the control sides of both treatment groups (Fig. 1). While the percentage of positive cultures was less than 50% in both treatment groups at 3 months following the last treatment, it grew considerably at the second follow-up visit (9 months follow-ing the last treatment) for both treatment groups and for both treatment sides. The lack of satisfactory mycological cure was reflected by the dermatologists’ low clinical assessment scores for both the treatment and control sides, with no significant difference between the 2 sides in both treatment groups (mean scores of ≤1.33). Age, sex and OSI score had no significant impact on the mycological or clinical results. Patient mean ± SD satisfaction was higher at the first follow-up visit (group A 3.27 ± 0.52; group B 3.27 ± 0.34) compared with the second visit (group A –2.97 ± 0.52; group B 2.88 ± 0.34). The mean ± SD pain evaluation score was slightly higher among the subjects in group A (5.3 ± 3.2) compared with group B (4 ± 2.6), but the differences were not significant (p = 0.102).
Fig. 1. The percentages of positive mycological cultures at 3 and 9 months following each treatment. PDT: photodynamic therapy.
To date, 6 publications have demonstrated the efficacy of AFR in combination with topical antifungal treatment or with PDT for the treatment of onychomycosis (3–8). Despite the methodological differences in most parameters (number of patients, number of treatment sessions, intervals between sessions, follow-up duration and presence or absence of a control group), they all showed good clinical responses with high percentages of mycological cure.
The 6 studies described above included small patient populations, had short follow-up periods or lacked a control group. In comparison, our current study design included a relatively large number of patients, a control side and a long follow-up period. Both treatment groups in our study had unsatisfactory clinical and mycological results. The control side of both groups, amorolfine lacquer and PDT alone, also failed to show good clinical efficacy. Finally, an interesting finding was the discrepancy between the failure of clinical and mycological cure and the relatively high unexplained levels of patient satisfaction.
Amorolfine is a synthetic antifungal drug that exhibits broad-spectrum fungistatic and fungicidal activity and is considered an effective topical treatment for onychomycosis (10, 11). The nails treated with amorolfine alone (group B, left toenails) demonstrated a 20% mycological cure. These findings are consistent with the relatively low mycological cure rates of the treatment of onychomycosis involving the matrix (10, 11).
In conclusion, this study calls into question the efficacy of laser-assisted PDT or laser-assisted amorolfine lacquer delivery for the treatment of toenail onychomycosis, and emphasizes the need for randomized controlled blinded trials with larger sample sizes to determine the actual efficacy of these treatment combinations.
The authors thank Ms Dvora Cohen and Ms Shoshi Zilber for their assistance in patients’ recruitment and Ms Esther Eshkol for editorial assistance.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize