


Departments of 1Dermatology, and 2Psychiatry, Ninewells Hospital, NHS Tayside, Dundee, United Kingdom
Perceptions of the clinical management of delusional infestation (DI) were compared with clinical outcomes in this 10-year case series from a single centre in Dundee, UK. An online questionnaire (survey-monkey, a TM brand of online survey available for free for basic use) was sent to Scottish Dermatologists to gauge their opinions and confidence in the management of DI. Also, a retrospective review of medical case notes of patients seen by dermatologists in one institution was undertaken and clinical outcomes were reported by patients’ general practitioners (GP). The survey showed that 61% of responding dermatologists encountered 1–5 cases of DI per year. Twenty-four percent respondees were ‘confident’ in managing patients with DI, 54% were ‘somewhat confident’. Forty-seven patients (62% female, 70% single) were seen over the 10 years; 43% brought a self-collected specimen to clinic, 68% of patients had a psychiatric comorbidity, 23% of patients had primary DI and 11/47 (23%) were seen by a psychiatrist. Clinical outcomes as rated by patients’ GPs were reasonable or good in 2/3 patients. A poor outcome was seen in 12 patients and associated with chronic pain in 50% (p < 0.01) and psychiatric comorbidity in 100% (p < 0.01). We conclude that good outcomes can be achieved in some patients with DI without psychiatric input and without psychoactive treatment.
Key words: delusional; infestation; parasitosis; psychodermatology.
Accepted Dec 20, 2017; Epub ahead of print Dec 21, 2017
Acta Derm Venereol 2018; 98: xx–xx.
Corr: Yee Ling Wong, Department of Dermatology, Ninewells Hospital, NHS Tayside, DD2 1UU Dundee, United Kingdom. E-mail: yeelingwong@nhs.net
Delusional infestation (DI) is a condition characterised by false, firmly held beliefs of infestation, involving either living or inanimate pathogens, despite objective evidence suggesting otherwise (1). The preferred term DI is often used interchangeably with delusions of parasitosis (which is too restrictive and suggests a specific aetiology), Ekbom’s syndrome, and Morgellons disease (2). Primary DI develops without any underlying physical or psychiatric cause whereas secondary DI occurs in the context of an underlying disorder including substance misuse, psychiatric illness, medication side effects and physical or structural brain abnormalities (3). Presenting clinical features include stinging, biting and crawling sensations, which may be associated with psychological distress and anxiety (4). Affected individuals often employ various methods of eradication and may inflict considerable damage to the skin in their efforts to remove the perceived infesting agent. (4). A proportion of patients (up to 75%) bring samples of the presumed pathogen to the clinic in an attempt to convince their doctor of the infestation. This is known as the ‘matchbox sign or ‘specimen sign’ (5). The ‘matchbox sign’ is a somewhat archaic term still used by many practitioners. Recent expert commentary has suggested that the “specimen sign” is a more suitable term as it is important whether the patient brings the specimen for examination regardless of which carrier the specimen is in (6). DI is a rare disorder, with an estimated incidence of 1.9 in 100,000 person years although it may be increasing (3). The prevalence is unknown due to the lack of population-based epidemiological research (5). Many patients are often reluctant to see a psychiatrist and lack insight. The challenges presented to the dermatologist and suggestions for clinical management are described elsewhere (3).
In this 10-year retrospective study we aim to compare and contrast the demographic detail and co-morbidities with previously reported case series of DI, highlighting the clinical outcomes in relation to patient factors and different management strategies.
There were two parts of this study:
1) In this first part of the study, the aim was to reveal how many dermatologists were happy to treat DI and how many considered the outcome of DI to be poor.
An online questionnaire was sent to all members of the Scottish Dermatology Society (SDS) to gauge their opinions and confidence in the management of DI. A total of 55 dermatologists responded in May 2017 (24% response rate). The questions asked and the answers are summarised in Table SI.
2) The second part of the study was designed to assess outcomes of the disorder.
Following Caldicott Guardian approval to ensure minimal use of patient identifiable data and transfer of information, a retrospective review of medical case notes of patients seen by dermatologists in Ninewells Hospital & Medical School, Scotland over the 10-year period (2007–2016) was undertaken. Fifty-eight patient records were retrieved from an electronic clinical database using the search terms ‘delusional”, “infestation’, ‘morgellons’, ‘ekbom’ and ‘delusions of parasitosis’. Inclusion criteria included patients who met the criteria for DI as outlined in Freudenmann and Lepping’s 2009 review. Other psychodermatological conditions derived from the search terms including acne excoriee and body dysmorphic disorder were excluded, leaving 47 patients in this case series. Data obtained included demographic information, symptom duration, referral source, presence of specimen sign, specimen types (examined and analysed microscopically by several specialties including pathology, microbiology, parasitology and plant science) and co–morbid medical and psychiatric conditions. Finally, to assess outcomes, written questionnaires with stamped return envelopes were sent to the patients’ general practitioner (GP) to gather follow-up data on emotional state, psychotropic medication and whether there had been any relapse of DI symptomatology.
A chi-square method was utilised to confirm the statistical significance of differences between groups. p < 0.01 was considered statistically significant.
Of the 229 online questionnaires sent, 55 responses were obtained (see Table SI). During their career to date, 98% dermatologists who responded to the survey had encountered patients with DI. 61% had encountered 1–5 cases of DI per year. 24% respondees were ‘confident’ in managing patients with DI, 54% were ‘somewhat confident’ and 22% were ‘not confident at all’. Out of 55 dermatologists, 49% felt confident to prescribe psychotropic medications to patients with DI without liaising with psychiatry. Some of the major challenges volunteered included engagement in treatment, strains in the doctor–patient relationship, time pressures in a general dermatology clinic, and reluctance to accept diagnosis. Among this group, 38/55 (69%) dermatologists had more than 10 years of experience. Of the 38 responses, 19 (50%) thought outcome was poor, followed by 12 (32%) who were unsure of the likely clinical course, and 7 (18%) who considered outcome to be potentially good.
Of the 47 patients, 62% were women (female-to-male ratio of 1.6 to 1), with a mean age of 55 years. The mean duration of symptoms prior to first presentation at a dermatology clinic was 12 months. GPs referred the majority of these patients. Only 3/47 patients were referred by another specialty (infectious disease, sexual health clinic and psychiatry) (Table SII). Following referral, 27 (57%) were managed by a dermatologist with special interest in psychodermatology, 9 (19%) by various general dermatologists, 6 patients (13%) were referred to psychiatry, 4 (9%) were seen in a joint psychodermatology clinic (established in 2014) and 1 patient (2%) was admitted for in-patient psychiatric treatment.
With regard to comorbidities (Table SIII), 81% of the patients were found to have no dermatological history. 68% had psychiatric comorbidities that included depression, anxiety, obsessive-compulsive disorder, psychosis, bipolar affective disorder, hypomania and encopresis, 32% had no psychiatric comorbidity; 23% had chronic pain. Medications used included anti-parasitic drugs (36%) and topical steroids (Table SIV). In terms of substance use, 5 (11%) were taking stimulants (amphetamine/cocaine); 5 (11%) used opiates (morphine/codeine); 7 (15%) were heavy smokers; 3 (6%) were alcohol dependent; and 2 (4%) concomitantly used alcohol and tobacco. Twenty-five (53%) denied any history of substance use (including alcohol and tobacco).
On physical examination excoriations dominated (n = 21; 44%); followed by dermatitis (n = 10; 21%) and pruritus (n = 10; 21%), ulceration (n = 6; 13%), lichen simplex (n = 5; 11%) and papules (n = 4; 9%). Normal skin was present in 8 patients (17%) patients. (Note that the percentage adds up over 100% due to multiple, coexisting dermatological findings).
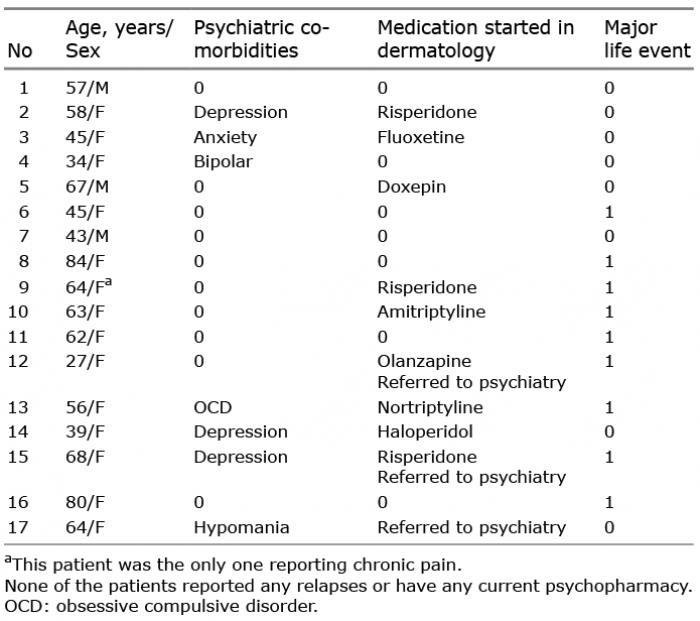
At the time of the study, 10 patients were deceased and therefore excluded from outcome measures. The cause of death for these 10 patients was: 3 cancer, 1 probable suicide, 2 old age, 1 hip fracture, 1 community-acquired pneumonia, 1 stroke and 1 exacerbation of chronic obstructive pulmonary disease. Of the 37 questionnaires sent to GPs enquiring about outcomes specific to their patient, 36 were completed and returned in June 2017 (response rate 97%). In terms of emotional well-being, 17 (47%) of GPs considered their patient to have ‘good’ well-being, 7 (19%) reported ‘average’ well-being and 12 (33%) reported ‘poor’ well-being; 26 (72%) of the patients had not had a further relapse following clinic attendance. Fifteen patients (42%) continued on psychotropic medication for DI and/or associated psychiatric disorder, including anti-depressant and anti-psychotic medications. We further compared the profiles of patients who had ’good’ (Table I) to those with ‘poor’ outcome (Table II) and statistically analysed the difference between the two groups in relation to pertinent psychiatric features, pain and major life events (Table III).
Table I. Detailed profile of 17 patients with ‘good’ outcome
Table II. Detailed profile of 12 patients with ‘poor’ outcome
Table III. Chi-square analysis of prevalence figures for some relevant features depending on outcome
In this retrospective case series, the demographic profile resembles other studies including a study from the European multicentre study (n = 148) (6), the Mayo Clinic in Rochester, USA (n = 147) (7), and an Australian multicentre study (n = 23) (2). These studies demonstrated that the majority of patients were women with a mean age of 56 years. In our study, 29/47 (62%) were female with a mean age of 55 years. Seventy percent of the patients were single (34%), divorced (15%), or widowed (21%). Seventy-nine percent of patients were unemployed; 21 (45%) were unable to work due to illness and 16 (34%) were retired. Contrasting our results, an American study reported that the majority of the patients from their cohort were married and not socially isolated (7). However, our results are consistent with the demographic data of most other reported studies in that single, older women who are socially isolated are most commonly affected by DI (8, 9).
The European multicentre study by Freudenmann et al. reported that no patients presenting with DI had a genuine infestation and that the specimen sign was present in 48% of all cases (6). Our case series revealed similar results, the specimen sign being present in 21 (45%) of cases.
Szepietowski et al. (10) in a survey of Polish dermatologists reported on the management of DI. The results showed that 85% of dermatologists had seen at least one patient with DI in their practice, compared to 98% in our study. The study also showed that 40.7% of the respondents ‘always ask’ and 28.8% ‘often ask’ for a psychiatric opinion. Interestingly, only 15.3% of dermatologists from the study would use their own pharmacological treatment such as sedatives and anxiety-relieving medications, prompting the authors to suggest an urgent need for psychodermatological training among dermatologists (10). This is much lower than the 49% of Scottish dermatologists who reported a willingness to prescribe a psychoactive medication in our study.
There are few reports detailing the specimen types and analysis in patients with DI. Nonetheless, this can be an important part of management and shows that the clinician is taking the patient’s concerns seriously. A study conducted by Hylwa et al. (11) was the first to address patient-provided specimens presenting with DI, although only 20 out of 80 samples were sent for microscopic evaluation.
Our study provided a complete set of data on analysed specimens presented to our centre. Of the 21 patients who brought specimens, 5 (24%) were skin squames, 5 (24%) were organic debris, 4 (19%) were actual insects, 3 (14%) were inorganic debris, and the remaining were hair 1 (5%), eyebrow 1 (5%) and 2 (10%) stool samples.
According to Lepping et al. (3), approximately half of all presentations in large case studies are primary delusional disorder. Our case series revealed that only 11/47 (23%) patients had primary DI ie. no neuropathology (stroke/ motor neurone disease/meningitis), history of substance use or psychiatric co-morbidities. This is very similar to the findings of Foster et al. (7) who identified psychiatric co-morbidities or substance abuse in 81% of patients (19% primary DI).
For the treatment of primary DI, limited evidence from case series previously suggested pimozide as first-line treatment. However, in recent years, other second-generation anti-psychotics with a better safety profile are usually preferred (3, 12). We are not aware of any randomised studies comparing outcomes of 2 antipsychotics. Pharmacological treatment should only be given after establishing a good relationship with the patient, as suggested by Patel & Koo (12).
We acknowledge that in individual cases it may be difficult to determine whether the delusional disorder has emerged in the context of a co-morbid psychiatric illness or the other way around, i.e. anxiety and depression could be triggered by difficulties coping with the DI symptomatology.
As training, teaching and published research on psychodermatological disorders has increased over the last 10–15 years, clinicians have become more familiar with treatment options. Our survey has shown that a significant proportion of dermatologists are now reasonably confident in managing this rare and challenging condition. (3, 5, 12). Close liaison with psychiatry is clearly desirable in individual cases and a joint psychodermatological clinic has obvious benefits as reported previously and is now established at our institution (4). However, we have found positive outcomes in our case series with 72% patients having no relapses since last contact with the clinic and 66% reporting average or good well being. Only 11/47 (23%) of patients were seen by a psychiatrist. Eleven patients had a coexisting chronic pain syndrome which could be considered somatoform in nature and we agree with Reichenberg et al. (13) that such patients may have a broader somatoform disorder which includes overvalued beliefs of infestation. We also agree that patients labelled with DI are a heterogeneous group whose beliefs exist on a spectrum ranging from overvalued ideas to frank delusions and may include tactile hallucinations (12). Indeed, we suggest it may be more appropriate for a dermatologist to use the descriptive term “medically unexplained formication with overvalued beliefs of infestation” rather than “delusional” which carries the risk of inaccuracy when strict diagnostic criteria are applied (14). Indeed distinguishing an overvalued idea from a delusion can be a challenging task, albeit both are clearly defined:
An overvalued idea is “an acceptable, comprehensible idea pursued by the patient beyond the bounds of reason” while a delusion can be considered “a false, unshakable belief, generated by internal morbid processes, which the patient believes with conviction to be true” (15) (Table SV).
To our knowledge, this is the first study that has addressed the outcomes of all patients with DI, and identified red flags associated with poorer outcome. The only other study that considered outcome was performed in 2011 by Wong & Bewley, but only addressed the outcomes of patients with DI who received pharmacotherapy (16). In our study, 9/12 (75%) patients who had a poor outcome had depressive disorder compared to 3/17 (18%) who had a good outcome (p = 0.0026). 12/12 (100%) patients with a poor outcome had an associated psychiatric diagnosis compared to 7/17 (41%) of the good outcome group (p = 0.0012). 6/12 (50%) patients who had a poor outcome had chronic pain compared with 1/17 (6%) who had a good outcome (p = 0.0074). Major life events, being female and single were common in both poor and good outcome groups and so not discriminatory regarding outcome. Seven of 17 patients (41%) with a good outcome were not treated with psychopharmacy compared to 2/12 (17%) who had poor outcome. Only 3/17 (18%) patients in the good outcome group were seen by psychiatry compared to 7/12 (58%) in the poor outcome group.
With a critical chi-square of 121.8 in contrast to a chi square level of 11.4 gives a p-value of p < 0.01. We can conclude that there is a significant difference between the good and poor outcome groups.
The rate of spontaneous remissions is debatable. According to Table I, 7 patients with good outcome improved without pharmacological treatment. Comparing to the whole data set, 7/47 (15%) of spontaneous remission was observed. Twenty-two of 47 patients were started with medications including those who died. Our data suggested that 9/17 (53%) patients in the good outcomes group were started with psychotropic medications in dermatology and none of them are currently on psychotropic medications from the GP questionnaire. From the average outcomes group, 2/7 (29%) patients were started with psychotropic medications in dermatology and 4/7 (57%) are currently on psychotropic medications. In the poor outcomes group, 7/12 (58%) were started on psychotropic medications and 10/12 (83%) are currently on psychotropic medications. An article published in 1946 suggested that the rate of spontaneous recovery without psychopharmacotherapy after only dermatological treatment was observed in 10% of the cases, partial remission in 8% of the cases and no effect in 82% of the cases (17). However, with increased knowledge and publications in the management of DI in the 71 years since this study, we suggest that good outcomes may be influenced by the holistic ability of the psychologically-minded dermatologist in talking and listening approaches rather than only providing dermatological treatment.
We accept that our study has some limitations. In the first part, we received a low response rate from the Scottish Dermatology Society. This is a limitation, as the other 76% of the dermatologists could have given answers that would dramatically change the results. Due to the retrospective nature of case notes review in the second part of the study, some findings may be limited by incomplete data and are therefore subjected to misinterpretation. Outcomes, were assessed indirectly, through a written questionnaire completed by general practitioners, and not through direct examination of patients during follow-up. This is subjective, and is a potential source of systemic error.
In conclusion, from our study red flags that suggest a poorer outcome include chronic pain and psychiatric co-morbidity, especially depression. The presence of such findings should alert dermatologists to seek further assessment from psychiatry, ideally, in our view, at a joint psychodermatology clinic. A proportion of patients have a good outcome without psychotropic drug treatment. However, our findings cannot be over-stated and generalised. Larger multicentre studies looking at treatment of DI may be helpful in the future, by e.g. comparing outcomes between single-handed dermatologists versus combined dermatology/psychiatry clinics. Treatment of any underlying cause of DI is desirable and in all cases a trial of an antipsychotic is usually indicated and often helps reduce the troublesome symptoms.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize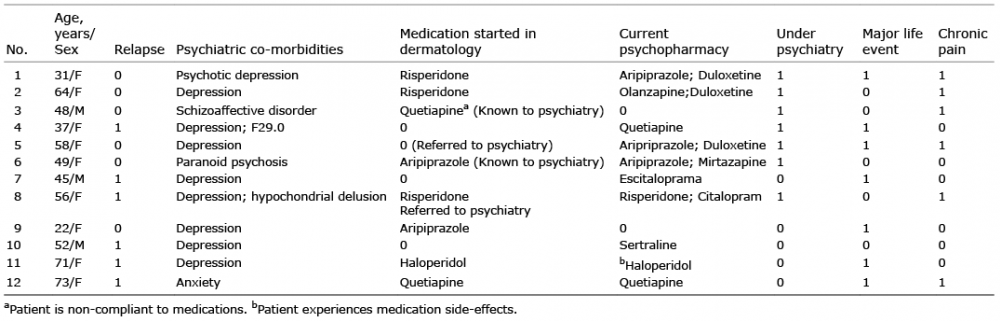 Click to show fullsize
Click to show fullsize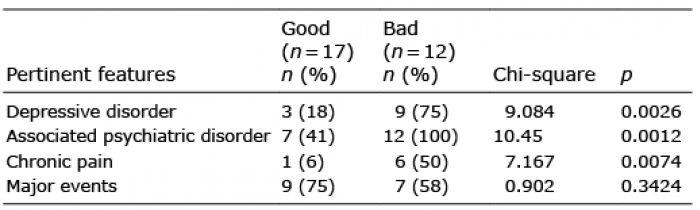 Click to show fullsize
Click to show fullsize