


Department of Dermatology, University Hospital Jena, Erfurter Straße 35, DE-07743 Jena, Germany. E-mail: tittelbach@derma-jena.de
Accepted Dec 20, 2017; Epub ahead of print Dec 21, 2017
Permanent makeup is a type of cosmetic tattoo in which micropigments are frequently used. The procedure is advertised as “harmless and safe” and the cosmeticians who perform it do not need any formal approval. None-theless, there is a broad spectrum of possible side-effects associated with permanent makeup, the most frequent being infections, and pigmentation of the surrounding area by lymphatic drainage of pigments or local inflammation (1, 2). Histological patterns of inflammatory reactions are non-specific. They may resemble acute contact dermatitis, chronic eczema, lichenoid dermatitis, lupus-like patterns or granulomatous, including foreign body and sarcoidal, reactions (3). A granulomatous reaction following tattooing may also indicate sarcoidosis (4, 5).
Treatment of inflammatory side-effects of permanent makeup can be challenging, due to deep deposition of the pigments. Patients must be informed about possible severe risks prior tattooing.
On initial presentation in our outpatient clinic, a 41-year-old woman reported having had permanent makeup 10 years previously, which had been refreshed after 5 years. She had noticed itchy red papules developing in the tattooed area, starting on one side, 18 months previously. Dermatological treatment with silicone scar gel, followed by mometasone cream, did not result in sufficient improvement. Therefore, a biopsy had been taken, which revealed a “granulomatous foreign body reaction”. The patient received laser treatment, which resulted in a temporary improvement, but was followed by new, now partially ulcerating, lesions. She then tried self-treatment with aloe-vera-containing gel and panthenol cream.
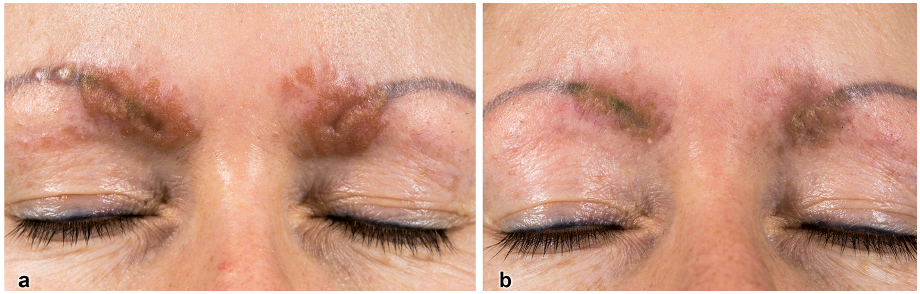
Dermatological examination revealed yellowish-erythematous indurated papules with mild scaling accentuated on the medial eyebrows (Fig. 1a).
Fig. 1. Clinical photographs before and after therapy. (a) Yellowish-brown-red papules and plaques, that showed an apple-jelly-coloured infiltrate under diascopy. (b) Improvement after 5 injections of triamcinolone; 24 weeks after first injection.
Angiotensin-converting enzyme, soluble interleukin-2-receptor, calcium level, blood sedimentation rate, and blood count were within normal ranges. Mycological testing of skin scales from the eyebrows (native, culture, and PCR) was negative for dermatophytes. Antinuclear antibodies were negative. Chest X-ray was without patho-logical findings.
Patch-tests according to recommendations by the German Contact-Allergy-Group (DKG) including standard, preservatives, ointment bases, hairdresser’s series-substances (6), as well as the patient’s own substances (aloe-vera gel, panthenol ointment, PUREBEAU HiCon Permanent Eyebrow-colour (PUREBEAU New Cosmetics GmbH, Berlin, Germany)) showed positive test results at 72 h only to nickel (II) sulphate (+++) and methylisothiazolinone (++), which were not present in the tattoo material.
A skin biopsy showed granulomatous accumulation of epithelioid cells in the whole dermis, surrounded by a sparse lymphocytic infiltrate and some multinucleated histiocytes on dermatopathological investigation. There was no evidence of foreign bodies under polarized light (Fig. 2) and special stains (Fite Faraco and Ziehl-Neelsen) did not reveal the presence of mycobacteria as reported by other authors (7, 8).
Fig. 2. Histological examination of a punch biopsy taken before therapy. (a) Multiple granulomas of epithelioid histiocytes throughout the whole dermis (haematoxylin and eosin (H&E), original magnification ×50). (b) Granulomas surrounded by sparse lymphocytic infiltrate. Few multinuclear histiocytes. (H&E ×200).
After the establishment of a diagnosis of a granulomatous foreign body reaction of sarcoidal type to tattoo-ink in the permanent makeup, we initially started topical treat-ment with clobetasol propionate cream. Due to lack of effectiveness, intralesional injections with triamcinolone were added. In total, the patient received 5 injections with 3–4 weeks interval, with a very satisfactory result (Fig. 1b).
We report here a case of a cosmetically disturbing and difficult-to-treat side-effect of permanent makeup. Manufacturers of micropigments usually connote the harmlessness of their products by claiming that the pigments will be deposited only “in the upper skin layers” instead of the deeper dermis, which is, however, not controlled. No standardized information of possible side-effects is provided to the customer. However, unintended deep dermal deposition of the pigments may cause inflammation and granulomata, and the treatment of side-effects of permanent makeup may be challenging, as the effectiveness of topical therapies is very limited in these cases. In some cases, laser therapy was reported to be successful (1). In the case described here, only dermal injection of triamcinolone led to a regression of the inflammation. Skin atrophy may be caused by this treatment, especially when the injection is subcutaneous. In addition, a relapse may occur. Interestingly, the current patient did not develop any granulomatous skin reactions in other tattooed areas. A possible explanation may be that specific pigments were the causative agent.
In general, for tattoo-reactions a histological examination should be performed in addition to allergy tests. Patch-testing may give negative results (9). In case a sarcoidal reaction is diagnosed, sarcoidosis should be ruled out. It should be mandatory to obtain informed consent from customers regarding the potential side-effects of permanent makeup. In the European Union, no consistent legal regulation on tattoos and permanent makeup has been implemented. A harmonization of regulations on patient education, patient consent, materials used, and rules for application is recommended in the interest of consumer health (10).
In conclusion, the potential adverse effects of cosmetic tattooing should not be underestimated. As for any other decorative tattoo, permanent makeup may cause disturbing and persistent side-effects.


 Click to show fullsize
Click to show fullsize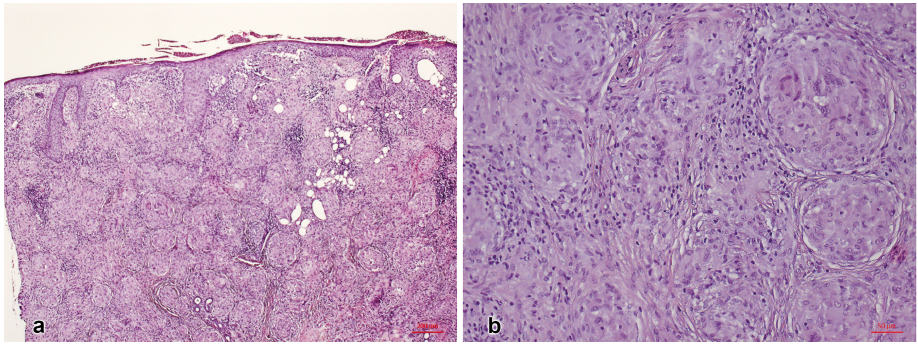 Click to show fullsize
Click to show fullsize