


1Department of Dermatology, Seoul St. Mary’s Hospital, and 2Department of Biostatistics, College of Medicine, The Catholic University of Korea, Seoul, Republic of Korea
This study investigated the prevalence of psoriasis and trends in prescription of medications for patients with psoriasis using the Korean National Health Insurance Claims Database from 2006 to 2015. The prevalence of psoriasis and psoriatic arthritis per 10,000 people increased from 47.4 to 61.5 and from 0.04 to 0.23 respectively. The prescription of topical agents was a mean of 73.3%. For systemic agents, prescription of acitretin decreased from 74.8 to 44.5%, methotrexate showed a fluctuation, with a mean of 14.9% and cyclosporine increased from 9.0 to 41.2%. The prescription of biological agents increased sharply from 18 to 1,127 patients. Use of ustekinumab increased from 4.1 to 82.4%; use of infliximab decreased from 20.7 to 6.7% and etanercept decreased from 100 to 6.1%. This study showed an increasing trend in the prevalence of psoriasis. We also reported a rapid increase in the use of biologics in recent years.
Key words: epidemiology; psoriasis; psoriatic arthritis; prevalence; medication.
Accepted Dec 20, 2017; Epub ahead of print Dec 21, 2017
Acta Derm Venereol 2018; 98:
Corr: Ji Hyun Lee, Department of Dermatology, College of Medicine, The Catholic University of Korea, Seoul 137-040, Korea. E-mail: yiji1@hanmail.net
Psoriasis is a T-helper-1 and -17 cell-mediated, chronic, inflammatory skin disease affecting approximately 1–3% of the general population (1, 2). The public health burden of psoriasis increases with rising prevalence. Psoriasis can involve skin, nails, and joints and be associated with a variety of systemic comorbidities such as cardiovascular disorders, stroke, hypertension, dyslipidemia, diabetes, metabolic syndromes and obesity (1, 3). The estimated prevalence of psoriatic arthritis (PsA) in psoriasis patients was 13.8% in the UK when using the ClASsification criteria for Psoriatic ARthritis (CASPAR) (4). Patients with psoriasis are increasingly burdened with comorbidities. In a systematic review, in 2013, the cost of psoriasis was estimated to be more than $121 billion (5).
Topical agents are generally the fist-line treatment for psoriasis, especially for mild disease, followed by phototherapy and DMARDs (disease-modifying antirheumatic drugs). In widespread disease, topical agents in combination with phototherapy or DMARDs could be considered. For patients who do not respond to these therapies, or certain patients who have PsA or nail involvement, biologic agent are recommended (6–8).
This study used the National Health Insurance System (NHIS) Claims Database of Korea in a nationwide study. In 1989, universal health coverage was achieved by the government that provides coverage for nearly 100% of the Korean population (9). This study examined the prevalence of psoriasis and the use of antipsoriatic medications in patients with psoriasis from 2006 to 2015. This study has a limitation that the prevalence of psoriasis might be underestimated.
This was a nationwide, population-based study. Data were from the NHIS claims database, which contains all billing claims provided by the NHIS program and the medical aid system from January 2006 through December 2015. The NHIS system is a mandatory universal health insurance program that contains comprehensive health-related information on the Korean population that is composed of all claims data such as drug prescriptions, International Classification of Disease (ICD) codes, and details about treatment (10). The Korean NHIS database represents the entire population and covers nearly 100% of the Korean population (from 48,341,311 individuals in 2006 to 51,574,044 in 2015) (11). In this study, age, sex and diagnostic codes for psoriasis and PsA based on the International Classification of Diseases, 10th revision (ICD-10) were retrieved with detailed information about prescriptions. This study was approved by the Ethics Committee of Seoul St. Mary’s Hospital, the Catholic University of Korea (KC16EISE0922) and was conducted according to the principles of the Declaration of Helsinki.
The study population consisted of patients who visited clinics or hospitals with an ICD-10 code of psoriasis (ICD-10 L40) and PsA (ICD-10 M073) more than once in a given year from January 2006 through December 2015. Prevalence was analyzed by classifying patients into 10 age groups: 0–9 years, 10–19 years, 20–29 years, 30–39 years, 40–49 years, 50–59 years, 60–69 years, 70–79 years, 80–89 years and > 90 years. The patients were classified into moderate to severe psoriasis who had received any systemic agent and mild psoriasis who had not received any systemic agents.
We analyzed prevalence of psoriasis by age, categorized into 10-year age groups. Prevalence of psoriasis from 2006 to 2015 was reported by level of disease severity. Prevalence in 2015 was reported by accounting for the age-specific and gender-specific distribution of the Korean population. Data were analyzed using SAS version 9.4 (SAS Institute, Cary, NC, USA). A p-value < 0.05 was considered statistically significant.
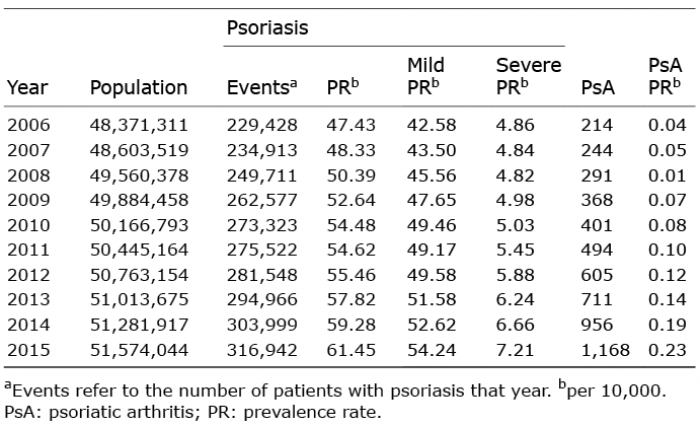
The annual prevalence of psoriasis and PsA from 2006 to 2015, as extracted from the NHIS Database, is summarized in Table I. From 2006 to 2015, the number of patients with psoriasis gradually increased from 229,428 to 316,942 and the number of patients with PsA also increased from 214 to 1,168. The prevalence of psoriasis increased from 47.43 to 61.45 per 10,000 people. In addition, the prevalence of PsA increased from 0.04 to 0.23 per 10,000 people. The prevalence of mild psoriasis increased from 42.58 to 54.24 per 10,000 people and the prevalence of severe psoriasis increased from 4.86 to 7.21 per 10,000 people.
Table I. Prevalence of psoriasis and psoriatic arthritis from 2006 to 2015
Age and sex distribution of psoriasis prevalence is in Fig. 1. Of psoriasis patients included in 2015, 56% were male and 44% were female. According to our study, prevalence gradually increased until the age of 50, and decreased after the age of 60. The prevalence of psoriasis in 2015 was 2.00% for people under 10 years of age, 2.90% for people in their teens, 4.79% in their 20s, 5.97% in their 30s, 6.46% in their 40s, 7.92% in their 50s, 9.59% in their 60s, 10.29% in their 70s, 8.63% in their 80s, and 5.33% in their 90s. In our study, annual prevalence of psoriasis gradually increased in patients younger than 70 years. This increase showed two peaks, for people in their 20s and 50s. Prevalence did not vary by sex in people who were younger than 30; however, in people older than 30, men had a higher prevalence than women and in patients aged from 30 to 60, prevalence increased more rapidly in men than women. In patients older than 70 years, prevalence decreased in both sexes. We additionally included age and sex distribution of psoriasis prevalence from 2006 to 2015 (Fig. S1).
Fig. 1. Age distribution of psoriasis prevalence in 2015.
The changing pattern of prescriptions for psoriasis through 2006 to 2015 is in Fig. 2a. Use of medications in psoriasis in 2006 was topical therapy in 88.47%, systemic therapy in 10.23%, and biologics in 0.01% of patients. In 2015, topical therapy accounted for 86.92%, systemic therapy, 11.64% and biologics, 0.35%. According to our results, the proportion of prescribed topical agents showed a mild fluctuating tendency and a mean use of 73.25% of all psoriasis patients. The proportion of systemic agents also fluctuated from 2006 to 2015, while biologics increased. In 2006, only 18 patients received biologics; in 2015, 1,114 patients received them. The proportion of patients prescribed biologics was about 0.01% in 2006 and increased to 0.35% in 2015. However, 15.30% (35,099 patients) in 2006 and 20.25% (n = 64,185) in 2015 were not treated.
Fig. 2. Patterns of psoriasis management from 2006 to 2015. (a) Total medication pattern. (b) Systemic treatment pattern. (c) Biologic treatment pattern.
We identified utilization rates for each component of systemics and biologics, described in Fig. 2b and c. Among all systemic agents, the proportion of acitretin and methotrexate decreased over time, from 74.76 (n = 18,733) to 44.49% (n = 17,764) for acitretin and 16.25 (n = 4,071) to 14.27% (n = 5,699) for methotrexate. More prompt decrement was estimated on acitretin. In contrast, the use of cyclosporine increased from 9.00% (n = 2,255) in 2006 to 41.24% (n = 16,466) in 2015. For biologics, in 2006, only etanercept was available. Its use declined over time and in 2015, etanercept was prescribed in 6.19% (n = 69) of patients. Similarly, infliximab was prescribed in about 20.69% (n = 6) in 2007 but decreased with a tendency to fluctuate and 6.73% (n = 75) was prescribed in 2015. The proportion of adalimumab prescriptions increased until 2008 from 6.9% (n = 2) in 2007 to 37.21% (n = 16) in 2008, then decreased. In 2015, the use of adalimumab was 15.08% (n = 168). Ustekinumab showed an increase in use after it was introduced in 2011. The proportion of prescribed ustekinumab was 41.16% (n = 128) in 2012 and increased to 74.60% (n = 831) in 2015.
Until now, the prevalence of psoriasis and PsA has not been evaluated in the entire Korean population. Using a nationwide population-based database, we evaluated the mean annual prevalence of psoriasis as 0.54% (54.28 per 10,000 people) during the 10 years between 2006 and 2015. Psoriasis is estimated to affect about 2–4% of the population in the US and Europe (12–14). The estimated prevalence of psoriasis is 2.2–3.2% in the US and 11.43% in Norway (12, 14–17). The prevalence of psoriasis is lower in East Asians than in caucasians (2, 3, 18–21). The prevalence of psoriasis is estimated to be 0.47% in China, 0.34% in Japan, and 0.24% in Taiwan (20–23). According to a previous report using population-based cohort from the Korean National Health Insurance, the prevalence gap between races might be suggested by genetic and/or environmental factors. In particular, genetic factors related to discrepancies in human antigen haplotypes between ethnic groups might lead to differences in prevalence (24). Environmental factors such as infection, stress, medication, humidity, cold weather, smoking, diet, and obesity might explain differences in psoriasis prevalence (25). In addition, we confirmed that the prevalence of psoriasis increased between 2006 and 2015. Wang et al. and Danielsen et al. also reported that psoriasis prevalence is increasing in Taiwan and North Norway respectively, consistent with our results (17, 18). Although the increase in awareness of psoriasis and the increase in use of health services cannot be completely ruled out altogether, changes in lifestyle and environmental factors such as diet, smoking and being overweight may have also contributed to the observed increase in prevalence of psoriasis (17). We estimated that psoriasis prevalence rapidly increased after age 20 and patients in their 50s were the largest group among psoriasis patients.
Our results showed a rapid increase in the prevalence of PsA from 0.0004% in 2006 to 0.0023% in 2015. However, this prevalence was lower than in other previous studies. In previous reports, PsA prevalence was estimated to be 0.02–0.42% in Europe (26, 27), 0.10–0.25% in the United States (13, 28), and 0.01–0.1% in China (29). The prevalence of inflammatory arthritis in psoriasis patients varied from 6–42% (30). In a population-based sample from England, Ibrahim et al. (4) reported that PsA prevalence in patients with psoriasis using the CASPAR criteria is 13.8%. Gelfand et al. (31) reported that the frequency of PsA in psoriasis patients is 11% in the US.
The goal of psoriasis treatment is to improve lesions without causing serious side effects and to prevent long-term recurrence. Treatment options for psoriasis are determined by considering the psoriasis severity and activity, the psoriatic type of lesion, lesion site, patient age, accessibility to treatment, comorbidities, and compliance. In this study, mild psoriasis was 7–9 times more common than severe psoriasis. In this study, on mean, the prescription of topical medication accounted for 73.3%, with mild fluctuation. Topical treatments are generally considered to be safe and were the most commonly used in this study (32).
Conventional systemic treatments have been used for a long time for cases of severe psoriasis. In 2015, the use in Korea was 11.64% of all treatments, with acitretin prescribed 48.15% of the time, methotrexate 15.45% and cyclosporin 44.63% (these include patients who have experienced more than one drug in 2015). In a US and Danish study, methotrexate was the most commonly used systemic drug (33, 34). For short-term (12–16 weeks) treatment, PASI75 was reached for 27% of acitretin, 46% of cyclosporine and 40–49% of methotrexate (35). However, long-term use of systemic treatment is often related to organ-specific adverse effects (36). Compared with other systemic agents such as methotrexate and acitretin, the increased use of cyclosporine may be due to the fact that it is relatively easy to use for female patients and that the side effects are easy to detect and control (37–39). Biologics account for the lowest percentage of psoriasis treatments, but 68% of the $3.5 billion global psoriasis market is biological therapy. Despite the economic burden, biological agents have advantages over conventional systemic treatments because they have favorable effects without serious side effects (36). Biologic prescriptions increased approximately 10-fold between 2006 and 2015 in Korea. Etanercept was the only approved TNF-alpha inhibitor (TNF-α inhibitor) biologic used in Korea in 2006. However, since 2006, the use of etanercept has decreased with the introduction of other TNF-α inhibitors, infliximab and adalimumab. After 2011, when ustekinumab, a monoclonal antibody of interleukin-12 and 23, was introduced, the prescription of all TNF-α inhibitors decreased rapidly. In 2015, ustekinumab accounted for about 75 % of biological agent prescriptions, but infliximab, etanercept and adalimumab were prescribed at about 7%, 6% and 15% each in Korea. In the US, initially, etanercept was the most preferred medication, but adalimumab use increased gradually in 2011 (12.4%) following approval of adalimumab for psoriatic arthritis in 2005 and for psoriasis in 2008 (34). PASI75 was 35–68% for adalimumab, 12–66% for etanercept, 38–53% for infliximab and 63–80% for ustekinumab for short-term (12–16 weeks) treatment (35). For long-term treatment (1- and 2-year data), PASI75 was 49–92.3% for etanercept, 44–89% for adalimumab and 65.5% for ustekinumab (35). Hwang et al. reported that ustekinumab is an efficient treatment choice for moderate-to-severe psoriasis and PsA and has the advantage of reducing the patient burden of visiting hospitals for long-term dosing intervals (2). In a study by the Psoriasis Longitudinal Assessment and Registry (PSOLAR), ustekinumab showed fewer major adverse effects than other biologics and nonbiologics such as malignancy, serious infection and cardiovascular events (40). Until now, ustekinumab has been dominant in the biologics market, but antibody agents that block specific cytokines produced by TH17 cells have fewer side effects and better efficacy and are likely to compete in established markets (41). Treatment guidelines in Korea are not much different from those in other countries such as the United States. However, recent impressive increase in ustekinumab is thought to be caused by the superior efficacy and low adverse effect of ustekinumab and the possibility of receiving ustekinumab treatment at an affordable price by expanding national health insurance coverage in Korea.
This study has some limitations. First, we did not include data on the amount and duration of medical treatment. Second, we did not measure severity based on PASI. Finally, therapeutic methods such as phototherapy were not included.
Despite these limitations, this study provides up-to-date prevalence information from nationwide data on more than 50 million people covering nearly 100% of Korean patients with psoriasis (42). In addition, we showed the latest treatment patterns for psoriasis, including topical and systemic treatments as well as biologics.
This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIP) (No. NRF-2015R1C1A2A01054767).
This study was approved by the ethics committee of the Catholic Medical Center Office of Human Research Protection Program (KC16EISE0922).
The authors have no conflict of interest to declare.


 Click to show fullsize
Click to show fullsize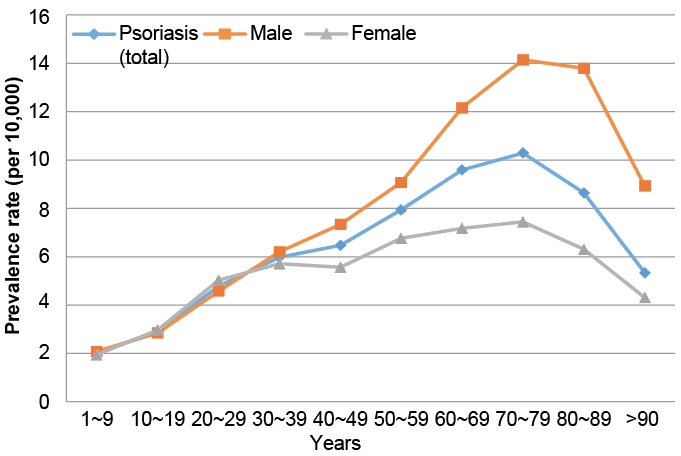 Click to show fullsize
Click to show fullsize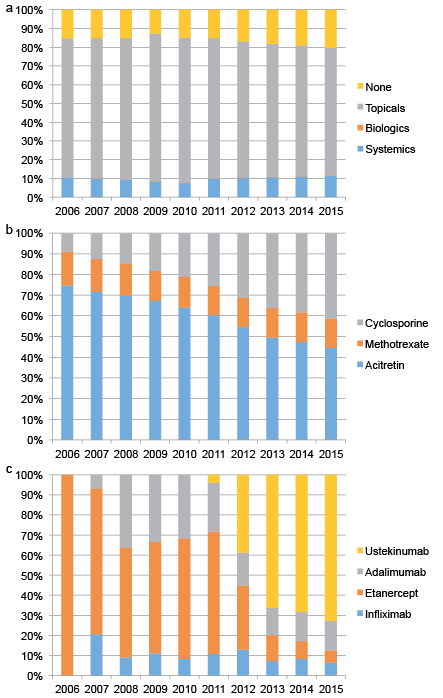 Click to show fullsize
Click to show fullsize