


Department of Dermatology, University Hospital of Aarhus, Marselisborg Centret, P.P. Orumsgade 11, DK-8000 Aarhus C, Denmark. E-mail: anneolse@rm.dk
Accepted Jan 8, 2018; Epub ahead of print Jan 9, 2018
In 2011 we reported 2 cases of patients with treatment-resistant, diffuse, deep, localized scleroderma (LoS), who showed significant improvement of both active disease and old fibrotic lesions on treatment with abatacept (1). Since then we have offered abatacept to adult patients with therapy-resistant, moderate-to-severe, active LoS. Abatacept is a fusion protein that acts as a T-cell co-stimulation blocker to inhibits tumour necrosis factor alpha (TNF-α) and prevent T-cell activation. Another group has also reported a good effect of abatacept in 3 patients with LoS (2), and there is an ongoing study of subcutaneous abatacept to treat diffuse cutaneous systemic sclerosis (SSc) (ASSET; https://clinicaltrials.gov/ct2/show/NCT02161406).
The LoS diseases are a group of sclerosing skin diseases of rare occurrence. They mainly affect females and young adults (3, 4). Adjacent tissue (fascia, muscle, bone) may also be affected in LoS, but, in contrast to SSc, there is no involvement of the internal organs (3). In the subtype called “en coup de sabre” involvement of the underlying central nervous system (e.g. seizures, migraine, headache) and abnormal ophthalmological findings (e.g. uveitis) can occur (5). Untreated LoS, especially the linear deep form, may result in joint contractures, muscle atrophy and growth limitations (5, 6). Although causing significant morbidity, plaque-type LoS typically has a benign self-limiting course of 3–5 years duration of disease activity of each lesion. In general, the course of the disease can vary, with improvement and reactivation over some years. Currently, there is no evidence-based causal (antifibrotic) treatment for LoS, and there is a lack of clinical trials with regard to other treatment options (7).
The aim of this study is to further determine whether abatacept may have a positive effect on disease activity in otherwise treatment-resistant LoS.
The scleroderma clinic at the Department of Dermato-Venereology of Aarhus University Hospital manages approximately 650 patients with scleroderma and scleroderma-like diseases. Each week a total of 2–4 new patients are admitted and 25–45 patients attend for regular control of disease and treatments. Through 2009 to 2016 we followed up on all adult treatment-resistant LoS patients who were treated experimentally with abatacept. The patients were treated with either 500 mg (patients weighing < 60 kg) or 750 mg (> 60 kg) abatacept intravenously on days 1, 15, 30, and thereafter every 4–6 weeks. Some patients switched to subcutaneous injection of 125 mg abatacept/week during treatment. Evaluations, including either modified Rodnan Skin Score (MRSS) or Localized Scleroderma Cutaneous Assessment Tool (LoSCAT) (8), were performed by well-trained doctors. Medical records review were conducted to extract data at two time points: At the beginning of abatacept treatment (the day the first abatacept treatment was injected) 1st assessment and either the latest follow up during treatment (the patient is still treated with abatacept) or at the determination (2 nd assessment) of abatacept treatment. Regarding patients with generalized LoS, MRSS and LoSCAT, data were collected at any time, prior to, during, and after abatacept treatment. Primary endpoints were changes in MRSS, LoSCAT, and/or change of size of lesions. Secondary endpoints were changes in CRP, C3c, C4, and/or PIIINP.
A total of 13 adults with treatment-resistant LoS were treated with abatacept (11 women and 2 men). Through-out 2016, 8 patients were still receiving treatment with abatacept (patient numbers 1–5, and 10–12) and 5 patients had stopped treatment (patient numbers 6–9, and 13) (Table SI). Primary endpoints are missing in 2 patients, both with “en coup de sabre” disease. The duration between assessment points ranges from 3 to 32 months, with a mean of 16 months. When measured, CRP, C3c, C4, and PIIINP were within reference ranges and without significant deviations in all patients.
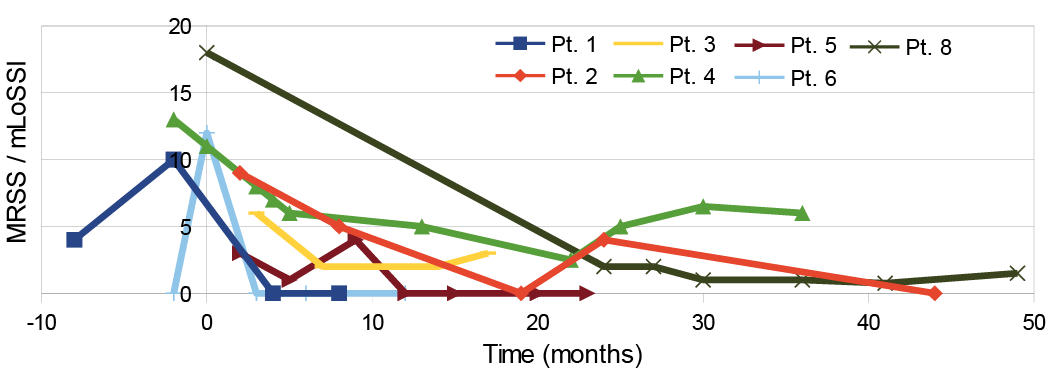
Eight patients had generalized LoS; 2 with a lichen sclerosus et atrophicus (LSA) overlap and 2 with a deep linear LoS overlap, and there was a mean reduction in MRSS (3 patients) of 6.7 (range 0– 6) over a mean treat-ment duration of 24 months. Likewise, LoSCAT was measured in 5 patients with a mean reduction in activity (modified LS Skin Severity Index; mLoSSI) of 4.2 (range (–7)–12) over a mean duration of 12.6 months. One patient with generalized LoS had an increase in mLoSSI over 16 months of treatment. There was a mean increase of 2.4 in LoSCAT damage score (LoSDI). Considering all scores of the same kind (either MRSS or mLoSSI) performed both before and during abatacept treatment, there is clear tendency towards a significant reduction in either score after initiation of treatment (Fig. 1). Scores have been made in 2 patients after cessation of abatacept treatment, with an increase in either MRSS or mLoSSI after approximately one year (data not included in Fig. 1).
Fig. 1. Modified Rodnan Skin Score (MRSS) and modified localized scleroderma skin Severity Index (mLoSSI) assessed in patients with generalized LoS before and after abatacept treatment. Pt.: patient number.
Five patients had linear or deep type LoS. Among these, MRSS have been measured in only one patient and showed a reduction from 5 to 1.5 after 13 months. Likewise, LoSCAT have been measured in 2 patients, with a reduction in activity from 18 to 3 over a period of 9 months in one patient and an activity score of 0 at both assessments in the other patient. Measurement of elements (in cm) has been carried out in 2 patients with LoS “en coup de sabre” (patient numbers 12 and 13). A significant reduction, approximately 50%, of the area (measured in cm2) was observed in both patients. Three patients had a reduction in damage scores (LoSDI) (between 1 and 2), whereas 3 patients had an increase in LoSDI (between 3 and 7).
In general, the patients reported moderate-to-good effect of the treatment with regard to skin symptoms/stiffness and, for 5 patients, improvement was observed with regard to general well-being, muscle aches, and joint pain (Table SI). One patient (patient number 9) initially experienced good effect, but treatment was later stopped due to a sense of progressive tightening in the skin, tingling and aching sensation in the legs, and fatigue. The most common reported side-effect was fatigue for 1–3 days after infusion. Also nausea and diarrhoea (in some cases with fever) has been described after treatment. Treatment was stopped in one patient (patient number 7) due to a diagnosis of ulcerative colitis. The patient had gastrointestinal symptoms prior to treatment with abatacept and a familial predisposition to the disease.
A reduction in activity of LoS was observed in this small group of patients with previously treatment-resistant LoS. The treatment was generally well tolerated, but some patients had transient adverse effects, such as fatigue, nausea and diarrhoea. However, this retrospective descriptive case study has several limitations in design, as well as the well-known difficulty of assessing disease severity in various forms of scleroderma. The clinical course of the disease with a general improvement over time, partially depending on subtype, is not regarded as a significant confounding factor in interpretation of the collected data, since the mean time between assessments of disease severity is 16 months, which is a short time relative to the activity of each lesion and mean duration of disease activity prior to treatment with abatacept. It is worth noticing that this is a highly selected group of treatment-resistant cases with severe disease. The effects in cases with milder disease, or of abatacept as 1st or 2nd line of systemic treatment, cannot be evaluated in a descriptive case series.
Overall, an improvement/reduction in size of lesions or MRSS/mLoSSI score were observed in this series of adult patients with LoS treated with abatacept. Thus, abatacept may be an appropriate treatment option for treatment-resistant LoS disease of different subtypes. However, further studies are needed.
Conflicts of interest. ABO performs studies in corporation with Actelion Roche and Boehringer-Ingelheim with no association to this study. SWF and KBA have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize