


1Department of Emergency and Organ Transplantation, School of Allergology and Clinical Immunology, University of Bari Aldo Moro, Bari, 2Scientific Directorate, IRCCS Burlo Garofolo, Trieste, 3Pneumology Department, Sacro Cuore Hospital, Gallipoli (Lecce), and 4Section of Allergy and Clinical Immunology, Unit of Internal Medicine, “F. Miulli” Hospital, Acquaviva delle Fonti, Bari, Italy. *E-mail: elisabettadileo71@libero.it
Accepted Jan 23, 2018; Epub ahead of print Jan 24, 2018
Chronic spontaneous urticaria (CSU) is a common skin disease defined as spontaneous recurrent wheals and angioedema or both lasting for at least 6 weeks (1). CSU usually has a duration of 1–5 years, but in 14% of patients it lasts longer (2). Omalizumab, an anti-IgE humanized monoclonal antibody, has proven effective for the treat-ment of CSU and is currently recommended as the third-line treatment option for management of CSU (1, 3).
A prospective observational study was carried out on 24 patients with moderate, H1 antihistamine-refractory CSU, managed at our referral centre since 2015, who received omalizumab re-treatment after a successful first course of treatment (i.e. ≥ 90% improvement in symptoms) (4) with this drug. In all patients, re-treatment was necessary because they experienced relapse of the disease with an intensity of symptoms (urticaria activity score [UAS7] ±15%) similar to the pre-treatment period. The option of taking non-sedating second-generation H1 antihistamines (nsAH) only as needed for symptomatic relief was investigated, rather than maintaining a stable daily dosage of nsAHs while on omalizumab treatment.
The study comprised a 4-week pre-treatment period, a 24-week first treatment period, an 8–16-week follow-up period, and a 24-week second treatment course. Patients were recruited who had moderate, refractory CSU, defined as having a history of spontaneous urticaria for more than 6 weeks, who had not responded to treatment with the approved dosage of nsAH for at least 4 weeks and who had a clinically diagnosed daily urticaria activity score (UAS) of 4 or more and a 7-day urticaria activity score (UAS7) be-tween 16 and 27 in the 7 days preceding the first treatment. UAS7 is a widely used patient-reported measure of CSU (1). Autologous serum skin test (ASST) (5) and measurement of dosage of total serum IgE were performed in all patients at baseline.
Omalizumab was administered subcutaneously every 4 weeks at doses of 300 mg for 24 weeks (1st treatment course) and again (2nd treatment course) at least 8 weeks after the end of the first course (6). Also, in the second treatment course all the patients received omalizumab 300 mg subcutaneously every 4 weeks for 24 weeks.
In the first cycle and between the first and the second cycles, patients continued to receive stable doses of their pre-treatment H1 antihistamine drugs. During the second treatment period the nsAHs were used continuously only in the first 10 days; thereafter they were administered at 1 dose per day only as needed in the case of mild exacerbations. Patients were allowed to take hydroxyzine 25 mg on demand for relief of symptoms throughout the entire study period, for a maximum of 3 doses per 24 h. Any side-effects of omalizumab were recorded.
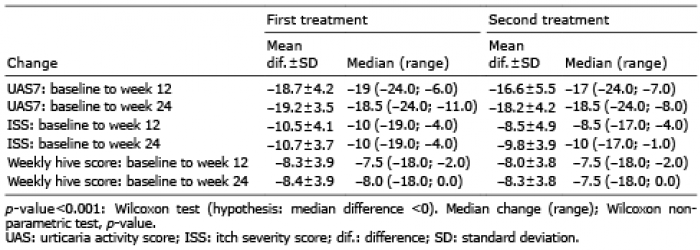
The median, range, mean and standard deviation (SD) at defined time intervals (baseline, 12 months, 24 months) were calculated for all 3 clinical scores (UAS7, hive and itch severity score (ISS)). Comparisons of median scores at 12 and 24 weeks of the latter 3 clinical outcomes with their corresponding baseline values were made using the Wilcoxon non-parametric test. The mean difference between the 3 clinical scores at 12 and 24 weeks and their respective baseline values was calculated using the t-test. Comparisons of proportions were made using the χ2 test. The level of significance was set at < 0.05. Statistical analysis was performed with Stata 14 package (Stata Corporation, College Station, TX, USA).
The local ethics committee approved the study and written informed consent was obtained from all patients (registration number: #5202).
For the 24 patients (58.3% (n = 14) women and 41.7% (n = 10) men) enrolled in the present study, the mean ± standard deviation (SD) age was 48.0 ± 13.7 years. The mean time since diagnosis of CSU was 15.2 ± 11.1 months. ASST was positive in 37.5% of subjects. The mean IgE level for patients was 161.2 ± 111.0 kU/L. The mean in-clinic UAS was 4.6 ± 0.7 and mean ± SD UAS7 19.8 ± 0.5. The nsAHs administered to the 24 patients were bilastine (n = 7; 29.2%), cetirizine (n = 4; 16.7%), fexofenadine (n = 3; 12.5%), levocetirizine (n = 2; 8.3%), rupatadine (n = 2; 8.3%) and ebastine (n = 6; 25.0%).
Following the first course of treatment, all patients experienced relapse of the disease, with a UAS 7 score similar to the value at pretreatment, within 9–19 weeks of the final injection of omalizumab (mean time to relapse 14.6 weeks). The mean ± SD UAS7 before starting the second treatment was 21.3 ± 2.7.
Table I compares the scores of all 3 clinical outcomes (UAS7, ISS, hive sore) at 12 and 24 weeks since the start of treatment with their respective baseline values (outcome at 12 weeks vs. baseline; outcome at 24 weeks vs. baseline) for both therapeutic regimes. Both treatments showed strong efficacy, with almost overlapping health outcomes at 12 and 24 weeks compared with their baseline values in terms of ISS (p < 0.001), hive score (p < 0.001) and UAS7 score p < 0.001).
Table I. Comparison of clinical end-points in the 2 treatment groups
Comparison of clinical scores between the 2 treatment courses (2nd vs. 1st) shows that there was only weak evidence of a difference between the 2 treatments for ISS score at 12 weeks (Wilcoxon test p-value = 0.03) and slightly higher values for the 2nd course. This discrepancy, however, waned at 24 weeks. Improvements in weekly UAS7 over time were similar in the 2 treatment groups (Fig. 1).
Fig. 1. Mean change in weekly urticaria activity score (UAS7) from baseline by study week for the first and second treatments.
There was some evidence of a difference between the 2 treatment courses in the proportion of patients with a UAS7 = 0 (p = 0.02) and itch-free days (p = 0.01) at 12 weeks, with slightly better health outcomes observed for the first treatment regimen. However, the latter differences disappeared at 24 weeks. No significant difference was detected between the 2 treatment courses regarding the proportions of patients with angioedema-free days in weeks 5–24. No significant differences were found between the 2 treatment courses in terms of number of hydroxyzine tablets taken by patients. In contrast, there was strong evidence (Wilcoxon p < 0.001) of a difference in the number of nsAH tablets taken by patients in the first treatment regimen compared with the second.
The 2 omalizumab treatments were very well tolerated.
There is currently no consensus regarding modality of CSU treatment with omalizumab and there is a lack of clinical trial data on concomitant H1 antihistamine therapy
during omalizumab treatment in this patient group.
In some randomized clinical trials (RCTs) patients continued to receive stable licensed doses of their pre-randomization H1-antihistamine throughout the treatment period with omalizumab (7, 8), or received high doses (2–4 times the approved dose) of H1 antihistamines (9), or maintained stable doses of their pre-randomization combination therapy with H1 antihistamine treatment plus H2 antihistamines, leukotriene receptor antagonists, or both (10). In other RCTs, patients were given H1-antihistamines on an as-needed basis throughout the treatment period (11, 12).
To our knowledge, this is the first study showing that nsAH as needed for symptom relief during omalizumab treatment is as effective as maintaining stable doses of the same drug in patients with moderate refractory CSU.
Despite a relatively small sample size, this study was still capable of detecting significant differences with relevant effect sizes. Although larger confirmatory studies are needed, our findings suggest that it might be preferable for patients with moderate CSU to combine a 24-week omalizumab treatment with nsAH as needed, rather than undertaking a daily H1 antihistamine therapy course at the approved dosage.
Thus, it is possible that concomitant use of nsAH is not necessary if omalizumab works. Or perhaps omalizumab would not necessarily be added to nsAH when nsAH does not work. Such a treatment regimen would be more advantageous, since it may have a positive impact on quality of life and the motivation of patients, thus potentially increasing their compliance with therapy. Moreover, the latter treatment approach would reduce the pharmaceutical costs, not only to the health service, but also to patients themselves. Lastly, although being more tolerated than first-generation counterparts, nsAH may still cause side-effects, particularly in sensitive individuals and in case of interaction with other medications taken by patients (13).
Furthermore, as previously reported (4, 14) in our study omalizumab provided rapid and effective symptomatic relief in both treatment courses, with almost overlapping health outcomes at 12 and 24 weeks.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize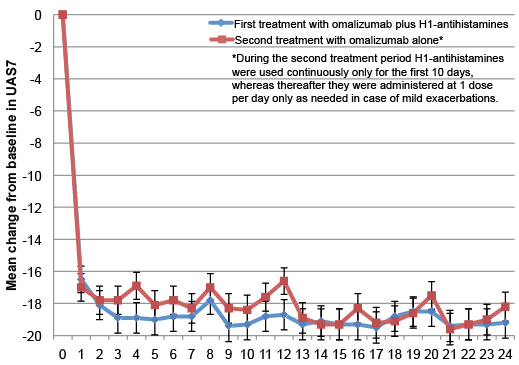 Click to show fullsize
Click to show fullsize