


1Department of Dermatology, Clinica Alemana de Santiago – Universidad del Desarrollo, 2Immunology Disciplinary Program, Universidad de Chile School of Medicine, Universidad de Chile, 3Medical Technology School, and 4Department of Epidemiology, Universidad del Desarrollo – Clinica Alemana School of Medicine, Santiago, Chile
Vitiligo is an acquired depigmenting disorder. To date, there is no predictive model for its response rate to narrowband ultraviolet B (NBUVB) phototherapy. The aim of this study was to investigate the different types of response of patients with non-segmental vitiligo undergoing NBUVB 3 times a week. Many patients who were previously considered non-responders were given the opportunity to continue the treatment. Long-term maintenance of treatment and follow-up of a cohort of 579 patients enabled different subtypes of response (very rapid, rapid, average, slow and “non-responders”) to be described for the first time, and a predictive model of response to be constructed based on repigmentation rate in the first 48 sessions of NBUVB. Among those patients who did not respond during the first 48 sessions, a new subgroup of patients was found, termed “very-slow” responders, who achieved a low, but significant, level of repigmentation after 96 sessions of NBUVB.
Key words: vitiligo; phototherapy; ultraviolet; narrowband UVB; predictive model.
Accepted Jan 23, 2018; Epub ahead of print Jan 24, 2018
Acta Derm Venereol 2018; XX: XX–XX.
Corr: Raul Cabrera, Department of Dermatology, Clinica Alemana de Santiago – Universidad del Desarrollo, Av. Manquehue Norte 1410, Vitacura, Santiago, Chile. E-mail: rcabrera@alemana.cl
Vitiligo is the most frequent cause of acquired leukoderma, and results in significant psychological and social difficulties for patients (1). Its prevalence varies from 0.5% to 2% (2). According to the Vitiligo European Task Force, the condition can be classified on clinical grounds into 3 major forms: non-segmental vitiligo (NSV), segmental vitiligo (SV) and mixed vitiligo (MV) (3). NSV, which is the most common type, is characterized by symmetrical and bilateral white patches or scattered symmetrical macules, with a long period of evolution. SV has a unilateral, band-shape distribution, with an early age of onset and rapid stabilization (4). The term “mixed vitiligo”, initially proposed by Mulekar et al. in 2006 (5), has recently been included in the main classification (3). MV shows initial segmental involvement, but in a second phase bilateral vitiligo patches usually follow (6). There are a few types of vitiligo that do not fall into this classification. Follicular vitiligo, recently described, is a primary vitiligo of the hair, in which hair whitening precedes leukoderma (7). Mucosal vitiligo refers to the exclusive involvement of oral or genital mucosa (8). Trichrome vitiligo, first suggested by Fitzpatrick (9), is the presence of vitiliginous patches with 3 colours; an achromic centre, a hypochromic border and the unaffected skin (10). All forms have in common progressive depigmentation of the skin, hair or mucosa (4).
Narrow-band ultraviolet B (NBUVB) phototherapy for vitiligo was first introduced in 1980, but the first specific publication concerning its use in vitiligo was published in 1997 (11); it is currently the treatment of choice for widespread forms of vitiligo due to its proven superiority to psoralen plus ultraviolet A (PUVA) and broadband UVB in terms of clinical effectiveness (11), safety and side-effect profiles (12–14). NBUVB has also been shown to be effective and well tolerated in children (15–18). Its mechanism of action includes immunomodulatory effects (19) and activation of repigmentation by proliferation, differentiation and migration of melanocyte precursors in hair follicles (20).
There is a full body of evidence supporting the usefulness of NBUVB in treating vitiligo, both in paediatric and adult populations. However, to date, there is no predictive model for the rate of repigmentation. This study of 579 patients constructs a new predictive model for the management of patients with vitiligo undergoing NBUVB treatment.
This retrospective cohort study included consecutive patients with SV and NSV diagnosed by physical examination, including Wood’s light examination, who were treated with NBUVB phototherapy at Clinica Alemana de Santiago, Santiago, Chile from January 2006 until March 2015.
Exclusion criteria were: MV, history of untreated cancer, primary or secondary immunodeficiency, photodermatoses, positive antinuclear antibodies, patients without complete photographic records, and those with failure to follow-up (i.e. patients who completed fewer than 24 sessions of phototherapy) and/or patients who missed more than 4 weeks of phototherapy. The study was approved by the IRB of Clinica Alemana de Santiago – Universidad del Desarrollo.
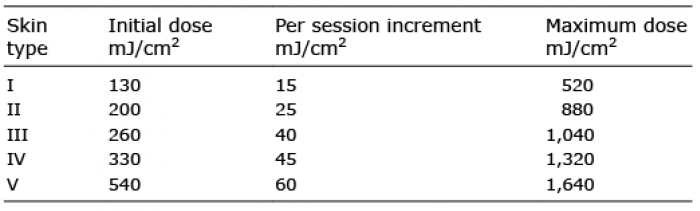
Phototherapy was performed according to Clinica Alemana protocols, based on Morison’s formally proposed scheme (21) with a variable dosage according to skin type (Table I). The Houva 4 Clinical Phototherapy System (National Biological, Ohio, USA), equipped with 48 NBUVB lamps was used, with daily calibrations performed by medical technologists. Patients underwent 3 sessions per week. No topical medications were used.
Table I. Initial, maximal and per-session increment in narrow-band ultraviolet B (NBUVB) dose according to skin type
Clinical information was obtained from patient records. Total body photographs were taken under standardized conditions using a Canon EOS t3i camera (Tokyo, Japan); before phototherapy and at 24, 48, 72, 96 sessions according to clinical individual response.
Each patient received at least 24 phototherapy sessions (1 cycle). More sessions were assigned according to clinical response and sessions were continuous. The number of phototherapy cycles completed by each patient depended on clinical response, medical prescription or treatment abandonment. Image records were stored in a secure database using TakioN Cap 2.3.7.132 software (CAS, Santiago, Chile). The extent and severity of depigmentation was calculated using the Vitiligo Area Scoring Index (VASI) scale (22), as modified by Komen, which includes the head and neck region (23).
To investigate the rate of repigmentation according to body site involvement, the severity of vitiligo in each body segment was studied by determining the area of repigmentation expressed as a percentage, using the palm plus volar surface of digits as 1% of total body surface area (24) and the degree of pigmentation in that area, using the same chart as that used for VASI calculation (22).
VASI scores were obtained at baseline and every 24 sessions up to 96 sessions. The repigmentation rate was also scored every 24 sessions, comparing baseline VASI with VASI at 24, 48, 72 or 96 sessions, respectively, and expressed as a percentage of change, using the following equation:
VASI t0 and VASI tx represent VASI at baseline, and VASI after x sessions, respectively. The rate of repigmentation is expressed in terms of percentage improvement in 1 or more 24-session cycles.
Given current recommendations to assess phototherapy response at 48 sessions (25), a rate of response and percentage of repigmentation in the first 24 and 48 sessions was used to classify patients as very rapid, rapid, average, slow responders, or non-responders (Table II).
Differences in response were examined according to: age, sex, disease duration, body segments involved and type of vitiligo.
Table II. Patient’s classification according to rate of repigmentation
To characterize the study sample, categorical variables are shown as numbers and percentages of cases, and numerical variables are shown as mean ± standard deviation.
Student’s t-test and analysis of variance (ANOVA) for repeated measures were used to compare treatment response according to body segment, type of vitiligo and time from diagnosis. Pearson’s correlation coefficient was used to correlate numerical variables.
A predictive model was developed using simple linear regression models. The slope of time vs. repigmentation gave the speed of response for each patient for periods between 24 or 48 sessions. Cut-off points were defined according to its maximum predictive power. A kappa index was used to evaluate correlation between initial speed of response and final treatment result.
A p-value ≤ 0.05 was considered statistically significant. All analyses were performed using SAS 9.3 (SAS Institute Inc., USA).
The demographic characteristics of the 579 patient cohort are listed in Table III. Global improvement of all patients after treatment was 42.9 ± 26.5%; 67 (11.6%) improved more than 75%, 335 (57.9%) between 25% and 75%, and 177 (30.5%) improved less than 25%. Mean improvement at 24 sessions was 21.5% (579 patients), 33.3% at 48 sessions (402 patients), 45.7% at 72 sessions (270 patients) and 56.1% at 96 sessions (182 patients).
Table III. Demographic characteristics of patients
The mean response according to rate of response and number of sessions is shown in Table IV. A global and a specific rate of response considering the body site of vitiligo is shown in Table V.
Table IV. Mean response according to number of sessions and rate of response
Table V. Type of rate of response and global response according to body segment involvement
Responses according to body site at different numbers of sessions (4 cycles of 24 sessions each) are shown in Fig. 1. Maximum final repigmentation responses were observed in the face (75%), trunk (64.89%) and superior limbs (61.81%). Unfavourable responses were seen in the feet (10.95%) and hands (14.88%). A significantly better response was found in NSV compared with SV (Fig. 2), with a repigmentation percentage of 57% vs. 43% at 96 sessions, respectively (p = 0.0006), these responses were achieved by different rate of response, with NSV being more rapid to respond.
Fig. 1. Repigmentation rate according to body segment. Significant differences are observed in face, hands and feet (p < 0.0001).
Fig. 2. Repigmentation rate according to type of vitiligo. Significant differences are observed at 96 sessions (p = 0.0006) between non-segmental and segmental vitiligo.
Based on the age of patients, significant differences in repigmentation response were found only in the trunk. Patients under 15 years of age had a 79.86% repigmentation, whereas patients aged 15 years or older had a 64.71% repigmentation (p = 0.006). No significant differences were attributable to sex (p = 0.56) or skin type (p = 0.39).
An inverse correlation (r = –0.15) was found between time from diagnosis and repigmentation percentage at 24 sessions (p = 0.0009), meaning that a shorter time from diagnosis was related to higher repigmentation percentage at 24 sessions. This correlation was not significant from 48 sessions onwards. However, when NSV and SV were analysed separately, there was no difference in SV at any cycle (p > 0.23), while NSV shows significant differences at 24, 48, 72 and 96 sessions (p < 0.008). These differences were found between patients whose vitiligo was diagnosed more than one year prior to initiation of treatment compared with those whose treatment was started within one year of diagnosis.
The repigmentation percentage achieved by the different response groups at each cycle was plotted. The slope of the curve is the rate of response (Fig. 3). At 96 sessions very rapid responders achieved 88% repigmentation, rapid responders 74.8%, average responders 58.4%, slow responders 38.8% and non-responders 35.2%. There were significant differences in repigmentation response between these groups during the whole length of treatment (p < 0.0001). When longitudinal behaviour in each of these groups was analysed, no significant differences were found in the rate of repigmentation in the very rapid responders between sessions 72 and 96 (p > 0.05), or in non-responders when comparing rate of repigmentation between 24 and 48 sessions. All other comparisons were significantly different (p < 0.05).
Fig. 3. Different groups are depicted according to rate of repigmentation. In very rapid responders no significant repigmentation difference is seen between 72 and 96 sessions (p > 0.05), while in slow and non-responder groups the ability to repigment is conserved until later periods of treatment.
Fig. 4 shows the predictive model of repigmentation response for up to 96 sessions. The final response can be estimated according to initial repigmentation rate in the first 48 sessions. There was substantial agreement, with a weighted kappa index of 0.7.
Fig. 4. Predictive model to estimate the final repigmentation response to narrow-band ultraviolet B phototherapy treatment according to the response in the first 48 sessions.
This 579 patient-cohort study is the largest single-institution study sample of patients with vitiligo treated with NBUVB to date. The male/female ratio is 1.02:1 and the type of vitiligo is 88.9% NSV and 11.1% SV. The statistical findings are in accordance with those found in existing literature. The global repigmentation response was 44.41% in NSV and 31.64% in SV. Good response was found in the face, neck, trunk and superior limbs, and poor response in the hands and feet (Fig. 1), which is consistent with the results of previous studies (8, 15, 18, 22, 26–30).
Age was an important factor; patients under 15 years old with NSV on the trunk (the most frequent vitiligo location in children) responded significantly better than adults (p = 0.006).
In our phototherapy protocol, each patient received from 24 (1 cycle) to 96 sessions (4 cycles) of NBUVB according to clinical response, recorded using sequential body photographs and VASI score. Only 8.1% of patients were lost to follow-up; a percentage that is considered to be very small, as it has been proven that losses smaller than 20% are irrelevant even if they are “not-random” (31). This study of a large number of patients following a long phototherapy protocol of NBUVB treatment has allowed us to build-up a predictive model of repigmentation response using the variable rate of response of the patients (Fig. 4).
Previous studies have demonstrated the “repigmentation potential” according to body site, treatment duration, type of vitiligo and ultraviolet used (NBUVB/PUVA) (27, 30, 32–34), but the repigmentation rate related to the number of sessions has not been described previously. Herein, we scored the repigmentation response at 24, 48, 72, 96 sessions and the slope of the curve for different subgroups according to rate of response allowed us to build a predictive model of response. According to this model, the long-term response of a single patient can be predicted by tracking his or her response at the 24 and 48 sessions of therapy, using their best position on the predictive model chart (Fig. 4).
At one extreme of the predictive model is the “very rapid responder” group, representing 13.1% of the cohort study and composed primarily of patients with NSV.
The NSV “very rapid responders” have preferential involvement of well responding areas, such as the face, neck and trunk (Table V). This subgroup of patients has an extremely high percentage of repigmentation in the first 48 sessions (77.3%) with 9.3% of improvement between 48–72 sessions and only 1.7% repigmentation between 72 and 96 sessions. Unexpectedly, 4 SV patients behaved as very rapid responders. They had a small area of vitiligo on the face, were under 25 years of age, and less than 9 months from diagnosis.
The “average responders” (the largest group) represents 37.4% of the cohort and is composed of 205 NSV and 11 SV patients. This group shows a progressively lower rate of response, with 31.7% of improvement in the first 48 sessions, 15.9% between 48 and 72 sessions, and 10.8% between 72 and 96 sessions. They differ from very rapid responders because, after 48 sessions, these patients still repigmented significantly (26.7%); thus in order to achieve the good response at 48 sessions shown by the very rapid responders, the average responders needed a longer treatment time.
At the other extreme of the predictive model is the “non-responder” group; 5.5% of the cohort (32 patients), composed of 20 females and 12 males, 14 NSV and 18 SV, and an mean age of 38 years (range 5–60 years). They were recently diagnosed (mean 6.15 months) and had a more localized disease. In this group hand involvement is more frequent (37.5%) than in the general cohort (34.5%). These patients show only 2.7% of repigmentation in the first 48 sessions, but unexpectedly they can still improve very slowly after 48 sessions. This group can still achieve an mean of 35.2% repigmentation at 96 sessions (Fig. 3), which falls under “moderate repigmentation” as proposed by Njoo et al. (35), and could have been considered as non-responders by other authors in previous reports (36, 37) that considered only the first 48 sessions of phototherapy for determining responsiveness to NBUVB phototherapy. One patient in this “non-responder group” had a response after 48 sessions comparable to that of average responders, 2 patients a response comparable to a rapid responder, and 1 patient a response comparable to a very rapid responder.
According to these data, the “non-responder” group cannot be evaluated using only 48 sessions. With our new data, a real “non-responder” has to be moved toward a response of 10% or less of repigmentation after 96 sessions.
Amongst the limitations of this study are that it is based on a single centre and that we did not include an assessment of patient satisfaction. However, we regard the degree of repigmentation as a good proxy of this latter point.
In conclusion, this cohort study found many different rates of response. The term “non-responder”, as described previously, must be redefined based on these new findings. The long follow-up of a large number of patients in this study enabled a predictive model of response to be constructed for the first time. This will be a valuable tool for dermatologists recommending NBUVB phototherapy.
The authors would like to thank Professor Henry W. Lim, Chair Emeritus, Department of Dermatology, Henry Ford Hospital, Detroit, Michigan, USA, for his constructive comments on this article.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize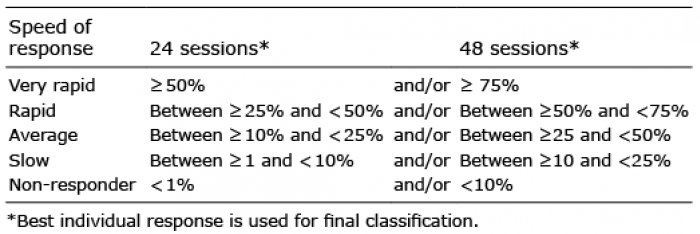 Click to show fullsize
Click to show fullsize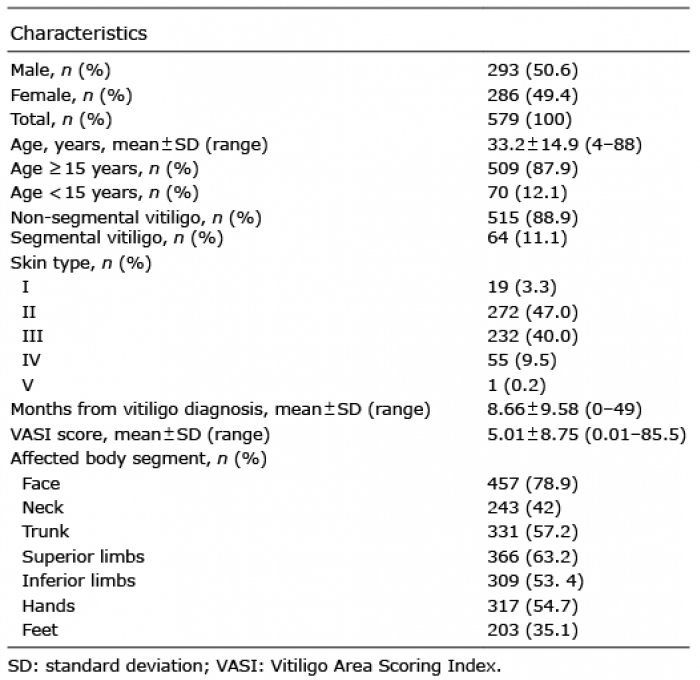 Click to show fullsize
Click to show fullsize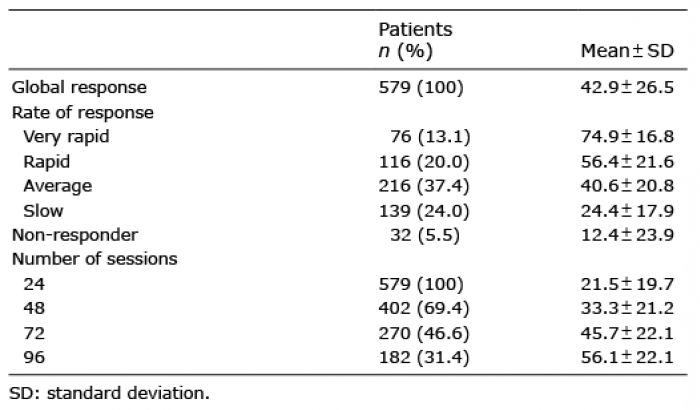 Click to show fullsize
Click to show fullsize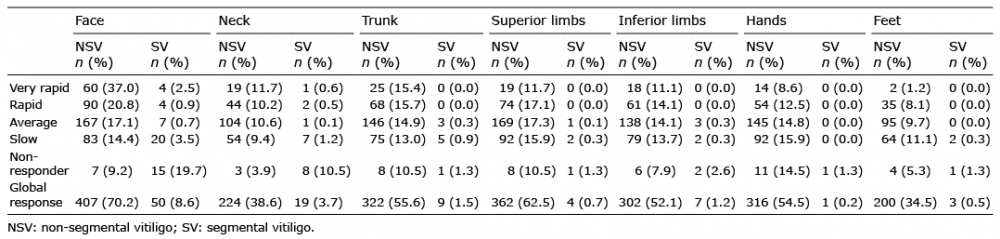 Click to show fullsize
Click to show fullsize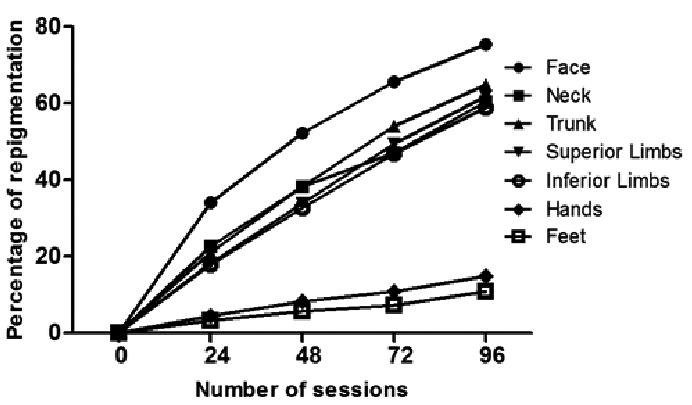 Click to show fullsize
Click to show fullsize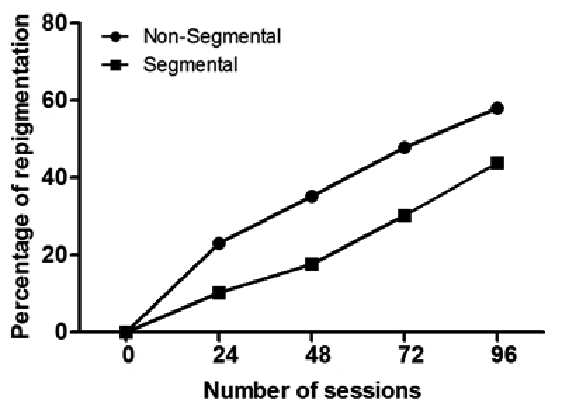 Click to show fullsize
Click to show fullsize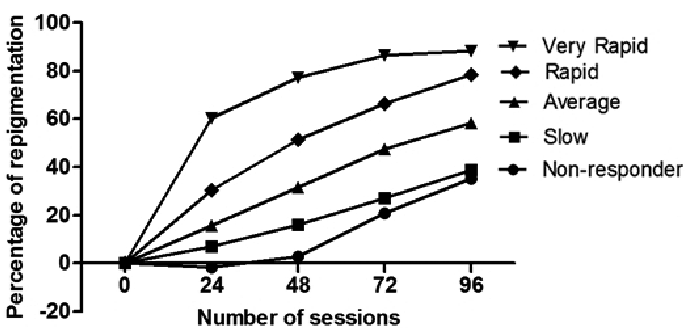 Click to show fullsize
Click to show fullsize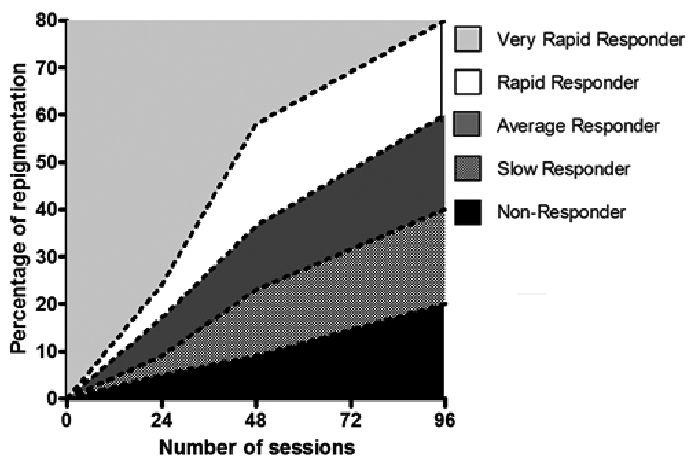 Click to show fullsize
Click to show fullsize