


Department of Dermatology and Venereology, Skåne University Hospital, SE-211 17 Malmö, Sweden. E-mail: gregtheodosiou@yahoo.com, Grigorios.Theodosiou@skane.se
A 17-year-old man presented with an unusual glistening texture of the hair since early childhood. No-one else in his family had a similar condition. His parents were non-consanguineous. The patient had been treated for acute lymphoblastic leukaemia 4 years earlier. His scalp hair had a banded appearance, with alternate dark and light colour (Fig. 1). His axillary and pubic hair was normal. No increased fragility and no other abnormality of the scalp were noted. Trichoscopy with a handheld dermatoscope revealed alternate white and dark bands, giving a zebra-like appearance (Fig. 2).
What is your diagnosis? See next page for answer.
Fig. 1. Scalp hair with a banded appearance.
Fig. 2. Trichoscopy: alternating 1–3-mm light and dark bands.
Acta Derm Venereol
Diagnosis: Pili annulati
Pili annulati (PA) ringed hair or “Morse alphabet” hair is a rare disorder of the hair shaft, which was first described by Landois in 1866 and is characterized by hair shafts with alternate white and dark bands (1). The light bands are the abnormal areas due to air-filled spaces within the cortex. The pathogenesis of PA remains unclear (2).
Inheritance of PA is determined by an autosomal dominant pattern. A locus for PA was mapped to chromosome 12q24.32–24.33, but it remains unknown which gene is responsible for the disease. Sporadic cases have also been reported (3).
PA is usually noted at birth or during infancy. The hair often appears shiny with a peculiar glistening texture, but is otherwise normal. The characteristic alternating light and dark bands are visible to the naked eye, but are best seen under trichoscopy (Fig. 2) and microscopy (Fig. 3). The abnormality is usually limited to scalp hair, but axillary, beard, and pubic hair may also be affected (1–4).
The light bands result from an increased light reflex due to clusters of abnormal, air-filled cavities in the cortex, which appear to result from insufficient production of the interfibrillar matrix (2, 4, 5).
Although, classically, PA is not associated with increased hair fragility, coexistence with trichorrhexis nodosa has been reported. The significance of PA is that the air-filled spaces between the macrofibrillar units of the hair cortex are more susceptible to weathering, particularly in combination with androgenetic alopecia. With the onset of hair thinning due to androgenetic alopecia, progressive reduction in the calibre of the hair shaft may induce increased trichorrhexis-nodosa-like hair fracturing in PA. In such cases, hair shaft fracturing is limited to the androgenetic region and co-localizes with the air-filled spaces of PA (5).
There are several reports of PA associated with alopecia areata. However, most of the authors believe that this is a coincidental concomitant manifestation, as a true pathognomonic association has yet to be proved (4).
Pili pseudoannulati also presents with light and dark bands, but has a different mechanism; it is a condition similar to PA, due to slightly flattened or twisted hair, as viewed under reflected light, and has no clinical significance (6).
In PA, the hair looks shiny and the majority of patients seem to find the changes attractive and accept them. No treatment is available.
The case of PA presented here demonstrates the classic clinical, trichoscopic and microscopic features of this condition (6). It also highlights that the characteristic features of PA can easily be visualized using trichoscopy without the need for plucking hairs for diagnostic purposes (7). Diagnosis of PA requires a high degree of clinical suspicion and careful clinical examination, since it is asymptomatic. It may be clinically relevant in cases of androgenetic alopecia as a cause of secondary trichorrhexis-nodosa-like changes in the air-filled spaces of the cortex (8, 9).
Fig. 3. Light microscopy: periodic dark and light bands in the hair shaft.


 Click to show fullsize
Click to show fullsize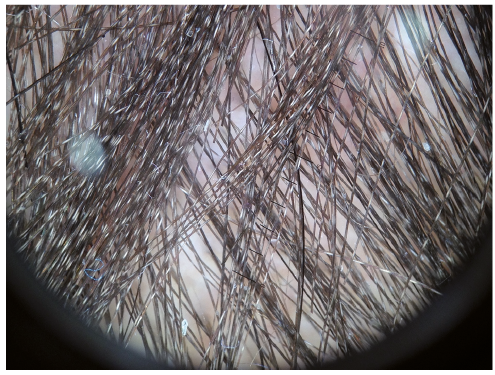 Click to show fullsize
Click to show fullsize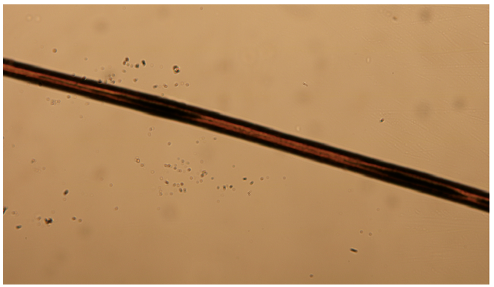 Click to show fullsize
Click to show fullsize