


1Department of Dermatology, Graduate School, Tokyo Medical and Dental University, Tokyo, Japan, and 2Department of Dermatology, National Defense Medical College, 3-2 Namiki, Tokorozawa, 359-8513, Saitama, Japan. E-mail: tasaderm@ndmc.ac.jp
Accepted Jan 29, 2018; Epub ahead of print Jan 30, 2018
Systemic sclerosis (SSc) is a multi-organ fibrotic autoimmune disease (1). Although the aetiologies underlying SSc remain unclear, vasculopathies (both micro- and macro-angiopathies) are thought to play important roles in the pathogenesis (2). Toe gangrene due to lower limb arterial occlusion often occurs in patients with SSc (3). The ankle-brachial pressure index (ABI) is widely used and considered useful for detecting lower limb arterial occlusion, particularly peripheral artery disease (PAD) (4). We report here a series of 7 SSc patients with toe gangrene due to macroangiopathy, in whom ABI values did not reflect the severity of arterial ischaemia.
Seven patients with SSc and toe gangrene were admitted to our department between April 2005 and March 2016. One patient had gangrene of a single toe, and 6 had multiple gangrene sites (Fig. 1a). Detailed profiles of the patients are shown in Table SI. Patients comprised 2 men and 5 women, with a mean age of 67.9 years (range 51–79 years). Five patients had limited cutaneous SSc with positive results for only anti-centromere antibody (ACA), one had diffuse cutaneous SSc with positive results for only anti-topoisomerase I (Topo-I) antibody, and one had diffuse cutaneous SSC with positive results for both ACA and anti-Topo-I antibody. All patients had Raynaud’s phenomenon. With regard to other vascular risk factors (diabetes mellitus, smoking habits, hypertension, and hypercholesterolaemia), one patient had a smoking habit, but no other risk factors, one was a smoker with hypertension, and 5 had none of these risk factors. Antiphospholipid antibodies were detected in only one patient (patient 4). No patients had any other connective tissue diseases, including systemic lupus erythematosus or Sjögren’s syndrome.
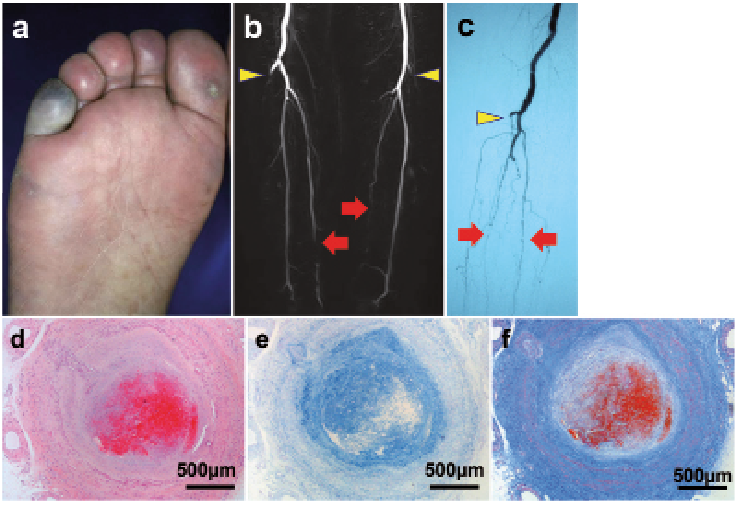
Fig. 1. (a) Toe gangrene and acrocyanosis (patient 6). (b, c) Features of magnetic resonance angiography (b, patient 1) and conventional catheter angiography (c, right limb of patient 4) of the lower limbs. Smooth luminal tapering (arrows) and obliteration (arrowheads) with poor collateral vessel formation are detected for below-the-knee arteries. (d–f) Histopathological features of posterior tibial artery (patient 6). (d) Intimal fibrosis or hyperplasia with luminal narrowing and presence of intraluminal thrombosis (haematoxylin and eosin stain; original magnification, × 40). (e) Acid mucopolysaccharide deposition in the intima (colloidal iron stain, × 40). (f) Adventitial fibrosis (Masson’s trichrome stain, × 40).
To determine whether macroangiopathy was present, we initially assessed the traditional ABI. Generally, an ABI < 0.4 suggests severe arterial occlusion, often in association with ulcers and/or gangrene, and is defined as representing critical limb ischaemia (CLI) (4). Unexpectedly, 5 patients showed almost normal ABI (≥ 0.8) and 2 patients showed ABIs of 0.62 and 0.61 (Table SI).
The “alternative” ABI has recently been reported to improve the prediction of mortality risk compared with traditional ABI (6). In our patients, however, only 2 patients showed values < 0.4 and 5 displayed values between 0.4 and 1.0 (Table SI). These results led to the assumption that macroangiopathy was not present in these patients.
Next, we conducted angiographic examinations to evaluate the involvement of medium-sized arteries in the lower extremities. No evidence of atherosclerosis was seen, such as involvement of multiple vascular beds, varied lesion lengths, calcifications, or irregular plaque in any of the patients. Instead, smooth luminal tapering and/or obliteration with poor collateral vessel formation was found for below-the-knee arteries (anterior tibial, posterior tibial, and/or peroneal arteries, but not all the arteries), but not for iliac or femoral arteries (Fig. 1b, c). These features are characteristic of vascular changes in SSc (3, 7).
Histopathological features of below-the-knee arteries from 2 patients (patients 4 and 6) who underwent lower extremity amputation are shown in Fig. 1d–f. The intima showed fibrosis and/or hyperplasia with luminal narrowing and intraluminal thrombosis. Deposition of acid mucopolysaccharides was accompanied by adventitial fibrosis. These findings were consistent with prior reports regarding digital arteries (8) and lower limb arteries (9) in patients with SSc. Based on these observations, structural changes characteristics of SSc might result in rigidity and incompressibility of arteries, leading to falsely elevated ankle pressures and deceptive ABIs.
Macroangiopathy in below-the-knee arteries was apparent in our patients. We initially expected that ABIs in our patients would be < 0.4. However, the results revealed that ABI failed to indicate the existence of macroangiopathy.
ABI is a commonly used parameter for detecting macroangiopathy, particularly arteriosclerosis obliterans. While high degrees of specificity (83.3–99.0%) and accuracy (72.1–89.2%) have been reported for ABI ≤0.90 in detecting ≥50% stenosis in the literature, different levels of sensitivity (15–79%) have been described (10).
Affected sites of arteries differ between atherosclerosis obliterans and SSc. In patients with SSc, 1 or 2, but not all, below-the-knee arteries tend to be affected. In addition, the iliac or femoral arteries are rarely involved in SSc, unlike atherosclerosis obliterans (3, 7). Discrepancies in results from ABI and angiography could thus be attributable to the fact that ABIs were calculated from higher-pressure values from some patent artery/arteries, leading to deceptive ABIs. The “alternative” ABI has been considered to indicate macroangiopathy with greater accuracy than the conventional method, as the alternative ABI is calculated using the lower of the dorsalis pedis or posterior tibial artery pressures (7). However, even the alternative ABI did not necessarily reflect the severity of ischaemia in our patients.
Another explanation for deceptive ABI values could be histopathological arterial changes characteristic of SSc (Fig. 1d–f). Unreliability of ABIs due to vessel rigidity and incompressibility has also been described in specific conditions, such as Mönckeberg-type arteriosclerosis and atherosclerosis associated with long-term haemodialysis and/or diabetes mellitus. Under such conditions, arteries show hard incompressibility due to severe calcification, particularly in the tunica media, and ABI indices are thus often falsely elevated and provide poor sensitivity for detecting angiopathy (11).
Previous research suggests that toe-brachial index and skin perfusion pressure would be more useful than ABI for evaluating angiopathy in patients with incompressible arteries, such as SSc (12, 13). Laser Doppler flowmetry and/or plethysmography should also be useful (14). However, these measurements do not specifically detect macroangio-pathy, as the values could also be influenced by impaired microcirculation of the toes due to thickening of the walls of cutaneous arterioles and tissue sclerosis. Thus, angio-graphic evaluations may be essential in patients with SSc when toe ischaemia is detected by these measurements.
A key limitation of this study was that it evaluated only 7 patients with SSc. Nevertheless, measuring ABI in SSc may carry a real risk of overlooking ischaemic changes in medium-sized arteries.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize