


Departments of 1Dermatology and 3Pathology, Hospital Clínico San Borja Arriarán, Santa Rosa 1234, Santiago, and 2Faculty of Medicine, University of Chile, Santiago, Chile. E-mail: javier_al20@hotmail.com
We report here a case of a 60-year-old woman with a history of adequately controlled type 2 diabetes, hypertension and hypothyroidism, on daily treatment with metformin, hydrochlorothiazide and levothyroxine. She presented at the dermatology clinic with a 10-year history of a slowly growing and occasionally painful plaque on her left breast.
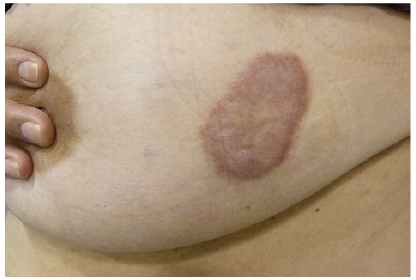
Physical examination revealed that the patient was an obese, but otherwise healthy, Hispanic woman with a brownish-coloured plaque that measured up to 6 cm in diameter, on her left breast (Fig. 1). Histopathology, punch biopsy and subsequent complete excision of the plaque demonstrated a spindle-cell proliferation, with myofibroblasts with no atypia (Fig. 2).
What is your diagnosis? See next page for answer.
Fig. 1. A brownish plaque on the left breast.
Fig. 2. (a) Haematoxylin and eosin (H&E) 25×. Band-like, ill-defined spindle-cell proliferation in the reticular dermis. (b) H&E 100×. Dermal myofibroblastic proliferation in fascicles running parallel to the epidermal surface. (c) H&E 400×. Uniform-spindled myofibroblasts with no nuclear atypia or mitoses.
Acta Derm Venereol 2018; XX: XX–XX.
Diagnosis: Dermatomyofibroma
Dermatomyofibroma (DMF) is a rare benign cutaneous mesenchymal neoplasm of myofibroblasts and fibroblasts that was first described in 1992 (1). It is often misdiagnosed because it is poorly known. The usual presentation of DMF is an asymptomatic, solitary, slowly growing red-brown discoloured plaque or nodule, located predominantly on the shoulder and adjacent regions, including the upper arm, axilla, neck and upper trunk (2, 3). In most cases lesions measure from 10 to 20 mm, with reports of lesions up to 150 mm, with the current case being one of the largest reported in recent years (4). DMF has been diagnosed predominantly in young female patients (3) and some cases have been reported in children (2). There is a hypothesis that, in female patients, DMF continue to grow after childhood, due to the effects of female hormones, whereas in male children lesions tend to regress spontaneously (5).
The histological findings include a benign dermal fibroblastic and myofibroblastic proliferation, consisting of uniform spindled cells with ill-defined outlines, pale cytoplasm and spindled bland nuclei, in intersecting fascicles, arranged parallel to the epidermal surface and perpendicular to the hypodermis. Between cells, fine collagen fibres and fragmented and often increased elastic fibres can be identified. Mononuclear inflammatory infiltrates and haemorrhage are rarely seen. The proliferation typically sits in the mid-reticular dermis, sparing the papillary dermis, hypodermis and adnexal structures. Mitoses are rare, and the proliferation rate is low (Ki-67 <5%). The epidermis may show hyperplasia. Tumour cells are positive for smooth muscle actin and vimentin, and negative for CD34, S100, factor XIIIa, desmin and beta-catenin. Indeed, immunostaining with actin was positive in smooth muscle and CD34 was negative in the spindled cells (Fig. 3).
Histological differential diagnoses include dermatofibroma, dermatofibrosarcoma protuberans, piloleiomyoma, fibromatosis and fibrous scar (3–5).
The treatment of choice is simple excision, with a favourable outcome; neither recurrence or metastases have been reported (3, 4).
This Chilean case illustrates the importance of an accurate diagnosis of DMF because it represents a relevant differential diagnosis from malignant lesions.


 Click to show fullsize
Click to show fullsize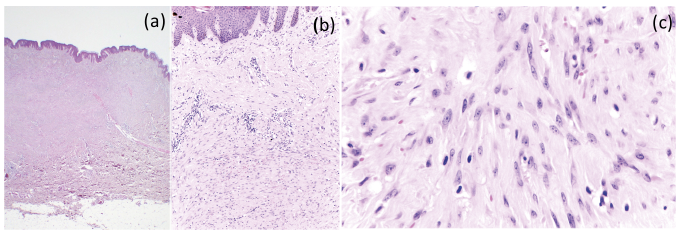 Click to show fullsize
Click to show fullsize