


1Department of Dermatology, and 2Division of Immunology and Rheumatology, Department of Internal Medicine 3, Hamamatsu University School of Medicine, 1-20-1 Handayama, Higashi-ku, Hamamatsu 431-3192, Japan. E-mail: t-shima@hama-med.ac.jp
Accepted Feb 5, 2018; Epub ahead of print Feb 6, 2018
Agents that modulate immune checkpoint proteins, such as programmed death receptor-1 (PD-1) and cytotoxic T-lymphocyte antigen-4 (CTLA-4), have become a main strategy in cancer treatment. Advanced melanoma is one of the major targets of immune checkpoint inhibitors (1). Their clinical benefit can be accompanied by immune-related adverse events (irAEs), which affect the skin, gastrointestinal tract, liver, and endocrine system. The endocrine organs of irAEs include pituitary, thyroid, and adrenal glands, as well as other downstream target organs (2). The endocrine irAEs are typically grade 1 or 2 in severity and often present with non-specific symptoms. In particular, isolated adrenocorticotrophic hormone (ACTH) deficiency is characterized by general fatigue, appetite loss, weight loss, hypoglycaemia, hypotension, and hyponatremia. Thus, these adverse effects might be underdiagnosed.
We report here 2 patients with advanced melanoma, who developed isolated ACTH deficiency induced by nivolumab (Nivo). This rare type of irAE should be considered in patients receiving long-term administration of immune checkpoint inhibitors, such as those with advanced melanoma.
Patient 1. A 53-year-old Japanese man with a primary nodular melanoma on the left thigh with lymph node metastasis was referred to us and diagnosed as American Joint Committee on Cancer (AJCC) stage IIID (pT4bN3bM0; Breslow tumour thickness, 8 mm; Clark’s level V, with ulceration; and Ki-67 index, approximately 50%). The patient received an extended resection of the primary tumour area with a 2-cm margin and inguinal and pelvic lymph node dissection, followed by administration of weekly PEG-interferon-α, 7 courses, as post-operative adjuvant therapy. Four months after the operation, however, he developed multiple skin metastatic lesions on the left thigh. Molecular testing revealed a BRAF V600E mutation. Thus, he was treated with a combination of BRAF inhibitor (dabrafenib) and MEK inhibitor (trametinib) with a therapeutic effect. Because of their cardiac adverse effect, the drugs were discontinued, and Nivo, 3 mg/kg, was begun at a 2-week interval. At 14 weeks after initiation of Nivo, the patient had muscle pain, general fatigue and vomiting, but no fever. The patient’s creatinine phosphokinase (CK) increased gradually to 648 U/l at 36 weeks with eosinophilia. His serum sodium level did not decrease.
Endocrinologically, ACTH, 6.5 pg/ml (normal 7–56 pg/ml), cortisol, 0.4 μg/l (normal 7.1–19.6 μg/l), urinary free cortisol, < 9.0 μg/g of creatinine (normal 11–80 μg/g), were decreased, indicating failure of the hypothalamo-pituitary-adrenal axis. Although thyroid stimulating hormone (TSH) was slightly increased, free T3 (FT3) and FT4 were normal, and anti-thyroidglobulin (Tg), thyroid peroxidase (TPO) and thyrotropin receptor (TR) antibodies were negative, indicating normal pituitary-thyroid function. Anti-diuretic hormone (ADH), growth hormone (GH), insulin-like growth factor-1 (IGF-1), luteinizing hormone (LH), and follicle stimulating hormone (FSH) were all within normal ranges. Magnetic resonance imaging (MRI) of the patient’s pituitary gland exhibited no abnormality in size or tumour lesion.
A detailed assessment of anterior pituitary functions with hypo-thalamic hormone challenges was performed. The results showed a disturbance in the secretion of ACTH in the corticotrophin-releasing hormone (CRH) test (Fig. S1). On the other hand, prolactin secretion was intact in the thyrotropin-releasing hormone (TRH) test, and the secretion of GH and LH/FSH was also normal in the GH-releasing peptide-2 (GHRP-2) and LH-releasing hormone (LH-RH) tests, respectively (Fig. S1).
His condition was diagnosed as isolated ACTH deficiency. At 36 weeks, he was treated with hydrocortisone, 15 mg daily, which improved muscle pain and general fatigue despite continuing Nivo treatment. At 16 months after initiation of Nivo, neither recurrence nor new metastatic lesion was found.
Patient 2. A 72-year-old man was diagnosed with AJCC stage IV melanoma (pTxNxM1b(0)), because of metastatic lesions of the left inguinal lymph nodes and the upper field of the right lung. He received surgical removal of the inguinal lymph nodes and lung lesion. Molecular testing for a BRAFV600E mutation was not performed, and he was treated with Nivo, 3 mg/kg, at 2-week intervals. At 28 weeks, he had general fatigue without fever, followed by appetite loss and vomiting. CK and blood eosinophil count fluctuated after initiation of Nivo, and at 44 weeks, his serum sodium level was dramatically decreased to 126 mEq/l. He had weight loss of 13 kg for 3 months.
Endocrinologically, ACTH and urinary free cortisol were within normal limits; however, cortisol (6.3 μg/l) was decreased. TSH, FT3 and FT4 showed normal levels, and anti-Tg, TPO and TR antibodies were negative. ADH, GH, IGF-1, LH, FSH were all within normal ranges. MRI of his pituitary gland exhibited no abnormality. Hypothalamic hormone challenges showed a disturbance in the secretion of ACTH in stimulation with CRH (Fig. S1). Prolactin secretion was intact in the TRH test, and GH secretion and LH/ FSH was also normal in the GHRP-2 and LH-RH tests, respectively (Fig. S1).
We thus diagnosed his condition as isolated ACTH deficiency. He was treated with hydrocortisone, 10 mg daily, with continuing Nivo. His fatigability and appetite loss improved. After recurrence of appetite loss, the dose of hydrocortisone was increased to 15 mg daily. At 15 months after initiation of Nivo, the patient died of multiple metastasis of melanoma, including liver, bone, and lymph nodes.
A recent cohort study demonstrated that the incidence of endocrine irAE was 12.9% in patients receiving ipilimumab (CTLA-4 inhibitor), Nivo, and/or pembrolizumab (PD-1 inhibitor), and the most common was thyroid dysfunction (11.1%), with a lower incidence of pituitary dysfunction (1.8%) (3). Other groups also reported that hypopituitarism is more frequently induced by ipilimumab than by Nivo (17.0% vs 1.97%), and they share male preponderance and lack of pituitary MRI abnormality (4, 5). The incidence rate of hypophysitis by pembrolizumab is also as low as 0.9% (6). Furthermore, in the CheckMate-069 trial, it was noted that the incidence of grade 1–2 hypophysitis ranged from 11% in patients treated with combination of Nivo and ipilimumab to 2% in patients treated with ipilimumab alone (7). Thus, an awareness of the symptoms and management of endocrine irAEs may aid in the safe and appropriate use of immune checkpoint inhibitors in clinical practice.
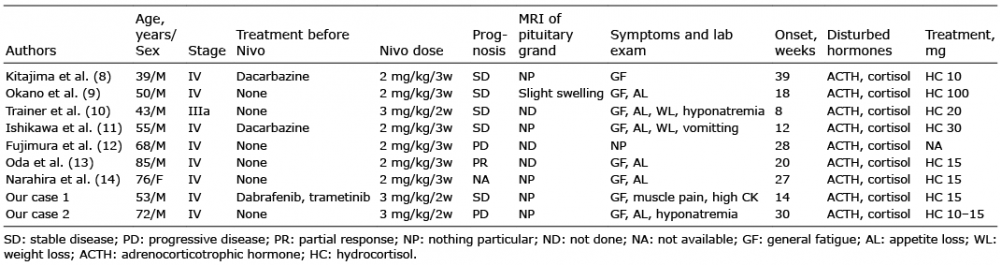
Table I summarizes the reported cases of hypopituitarism induced by Nivo in patients with advanced melanoma (8–14). Eight out of 9 patients, including our 2 cases, are men. The reason for this male preponderance is unknown. In all cases, hypopituitarism was diagnosed as isolated ACTH deficiency and the onset of isolated ACTH deficiency was 8–40 weeks after initiation of Nivo. Hypopituitarism has been reported in melanoma patients, but rarely in patients with lung cancer (15) despite the higher number of Nivo-treated lung cancer patients. Considering that melanoma patients are usually treated with Nivo for a longer period, the length of treatment might contribute to the development of this irAE.
Table I. Reported cases of hypopituitarism in advanced melanoma patients treated with nivolumab (Nivo)
The hypopituitarism of ipilimumab ranges from isolated deficiency to multiple hormone deficiency (4, 5), but our study suggests that Nivo shows only isolated ACTH deficiency. Given that ipilimumab can promote sensitization of CTLs, it is reasonable that this anti-CTLA-4 antibody yield CTLs specific to various pituitary antigenic determinants. On the other hand, Nivo may enhance only the CTL that have already been sensitized in melanoma patients, and antibody-dependent cellular cytotoxicity (ADCC) might operate with specific antibodies. In this context, the presence of autoimmune hypophysitis, also known as primary lymphocytic hypophysitis, provides an explanation. Nivo might render this disorder overt by activating CTLs, possibly with ADCC activity.
Clinically, isolated ACTH deficiency should be borne in mind when melanoma patients treated with immune checkpoint inhibitors develop non-specific, general malaise. Elucidation of its mechanism also may contribute to prediction of this deficiency.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize