


1Department of Clinical Social Medicine, Environmental and Occupational Dermatology, Ruprecht Karls University Heidelberg, Voßstr. 2, DE-69115 Heidelberg, 2Private Practice for Dermatology, Künzelsau, 3Institute of Pathology, and 4Institute for Diagnostic and Interventional Radiology, Caritas Hospital, Bad Mergentheim, Germany. *E-mail: elke.weisshaar@med.uni-heidelberg.de
Accepted Feb 13, 2018; Epub ahead of print Feb 13, 2018
Malignancies can be accompanied by paraneoplastic symptoms or syndromes, which may be caused by an indirect effect of the malignancy and may be the first sign of a cancer (1–4). The symptom “paraneoplastic itch” (PI) describes itch as a systemic reaction to the presence of a malignancy, “neither induced by the local presence of cancer cells nor by tumour therapy” (3). PI is often associated with haematological malignancies, but has also been reported in patients with solid tumours. Paraneoplastic neurological syndromes (PNS) are a group of rare neurological disorders that usually precede the detection of the underlying cancer (4). PNS can affect any part of the nervous system and many are associated with onconeural antibodies (4–6). We report here a patient with generalized pruritus that preceded a paraneoplastic neurological syndrome associated with onconeural anti-Hu antibodies due to large cell neuroendocrine carcinoma (LCNEC). The aim of this report is to highlight the consequence of misdiagnosed or underdiagnosed chronic itch (CI).
A 68-year-old man developed CI on normal-looking skin (head, arms, shoulder, thighs) in December 2015. Several treatments, e.g. topical corticosteroids and systemic antihistamines had no effect. When he presented to the Itch Clinic at University Hospital Heidelberg for the first time in March 2016 the CI had a burning, stinging and sharp character and was suspected to be of neuropathic origin. The severity of itch, assessed by numerical rating scale (NRS), was 10 (scale 0–10 [0: no itch, 10: maximum imaginable itch]). His quality of life (assessed by question) was severely reduced and the patient reported severe sleeplessness due to CI. His medical history revealed a good response of CI only to a therapy with systemic corticosteroids, prednisolone 20 mg per day for 2 weeks. His medical history included myocardial infarction, pneumonia, heartburn, iron deficiency and active smoking. The patient was advised to get a full body check-up (internal medicine, neurology), but did not do so because he attributed the itch to psychological distress.
Four months later, in July 2016, the patient had lost 10 kg of weight and developed nausea and vomiting. He reported loss of hearing, tinnitus and vertigo, as well as walking impairment, dysaesthesia and numbness of the legs. Neurological examination revealed cerebellar ataxia and a bilateral vestibular pathology. Electroneurography revealed a severe sensomotoric polyneuropathy. To detect a potential underlying malignancy, imaging examinations (e.g. chest X-ray, abdominal ultrasound, pelvis computed tomography (CT) scan) and lumbar puncture were performed. Imaging showed no evidence of a tumour, but lumbar puncture revealed the presence of onconeural anti-Hu antibodies. In the further course of the disease, the patient developed neurological gastrointestinal paresis, as well as micturition disturbance as a part of PNS.
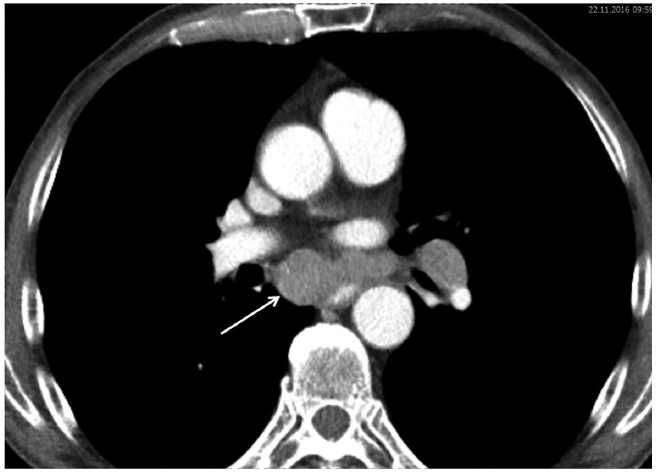
Therefore, a close follow-up scheme was set up to detect the underlying malignancy. During the second half of 2016 itching was still present, but had decreased. Due to the dominance of the other symptoms and their impairment, as well as the patient’s reduced general health status, he did not present to the dermatologist and only incomplete information about itch is available. In November 2016, CT scan showed a suspicious mediastinal lymph node enlargement (Fig. 1) so that a lymph-node-biopsy was taken. The biopsy proved lymph node metastases by a large cell neuroendocrine carcinoma (LCNEC), a rare subgroup of high-grade neuroendocrine tumour, typically of pulmonary origin. This diagnosis requires the presence of a neuroendocrine pattern and positive staining with neuroendocrine markers (chromogranin A, synaptophysin, CD 56) in immunohistochemistry, which was demonstrated in the patient (Fig. 2). However, the primary carcinoma location could not be detected. The patient received 2 cycles of chemotherapy (cisplatin, etoposide) with partial remission and radiotherapy was initiated. CI had disappeared completely after the second cycle of chemotherapy. In April 2017, before the third cycle of chemotherapy could be started, the patient died from a nosocomial pneumonia.
Fig. 1. Computed tomography (CT) scan (November 2016) showing axial slices. The arrow indicates subcarinal lymph node enlargement.
Fig. 2. Histopathology of the patient’s mediastinal lymph node (original magnification 200 x): note the characteristic perinuclear fine granular positivity for the most specific neuroendocrine marker, synaptophysin.
We report here the case of a patient with generalized CI preceding a large cell neuroendocrine carcinoma (LCNEC) associated with anti-Hu positive paraneoplastic neurological syndrome. It is likely that CI was the first paraneoplastic symptom in this patient, triggered by the large cell neuroendocrine tumour. We also suspect that the generalized pruritus was the first sign of a paraneoplastic sensory neuropathy, secondary to the production of onconeural antibodies. The detected anti-Hu antibodies are well characterized and frequently detected onconeural antibodies. They were first described in 1985 in a patient named “Hull” who had a PNS (7). Onconeural antibodies cross-react with antigens expressed on tumour cells and neuronal antigens in healthy cells. The clinical character of the patient’s itch, described as burning, stinging and sharp, indicates a neuropathic origin. A falsely initiated immune reaction could explain the good response of the CI to therapy with systemic glucocorticosteroids.
In more than 90% of all cases anti-Hu antibodies are related to small cell lung cancer (SCLC), but they have also been reported in patients with, for example, non-SCLC, prostate-cancer, lymphoma, and gynaecological tumours (8). In neuroendocrine cancer, onconeural antibody-associated PNS is rare (9, 10). CI in patients with diagnosed paraneoplastic neurological syndromes (PNS) has been reported only in single cases (11, 12).
PNS criteria have been developed that classify a neurological syndrome as definitely or possibly paraneoplastic. If well-characterized onconeural antibodies are present and the patient has a suspected PNS, irrespective of whether a cancer has been detected, the diagnosis of a definite PNS should be made (5). Diagnosis of PNS should prompt the investigation of an underlying malignancy, every 3–6 months (13).
In conclusion, CI should always be taken seriously by dermatologists and other physicians. It should be borne in mind that CI without concomitant skin changes and clinical signs of neuropathic origin, followed by neurological symptoms, can be caused by an undiagnosed PNS. In PNS early diagnosis is crucial for a successful tumour-specific and immunosuppressive therapy (13, 14). Therefore patients with CI should always be asked whether they have other sensations, such as pinching, prickling, burning or pain on the skin, to detect a neuropathic origin of the itch. Particular attention should be paid to additional neurological symptoms and complaints. A precise diagnostic check-up is always necessary and the underlying need should be explained carefully to the patient, who may not understand why all the time-consuming and extensive investigations are necessary.


 Click to show fullsize
Click to show fullsize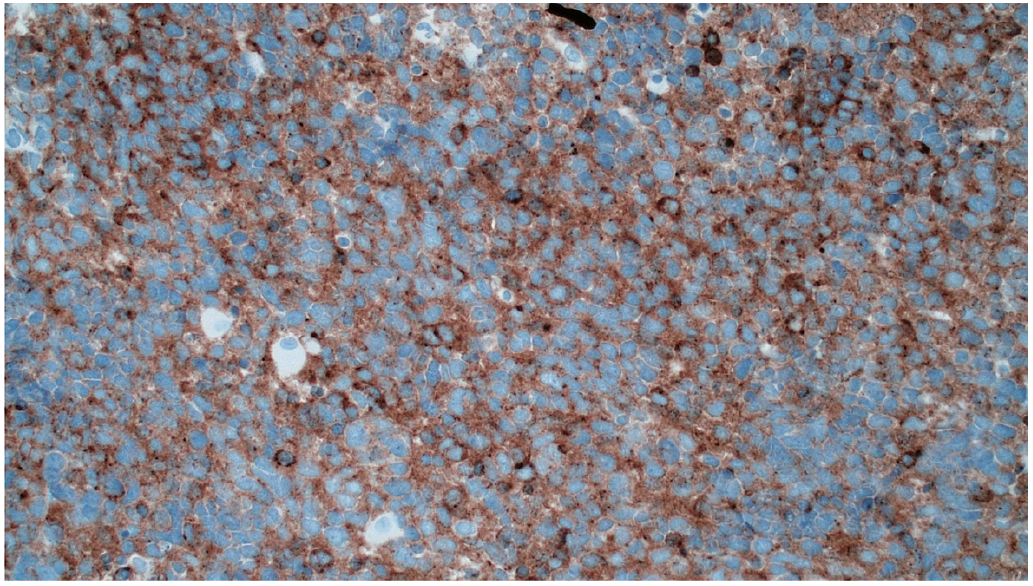 Click to show fullsize
Click to show fullsize