


1Department of Dermatology, and 2Department of Pathology, University Medical Center Ruprecht-Karls-University Heidelberg, Im Neuenheimer Feld 440, DE-69120 Heidelberg, Germany. E-mail: ferdinand.toberer@med.uni-heidelberg.de
Accepted Mar 1, 2018; Epub ahead of print Mar 2, 2018
Primary cutaneous diffuse large B-cell lymphoma, leg type (PCDLBCL-LT) is a malignant lymphoma of intermediate behaviour representing approximately 20% of cutaneous B-cell lymphomas (1). PCDLBCL-LT typically affects the leg(s) of elderly patients (mean age 76 years, women:men ratio 1.6) (2). We report here a very rare case that underwent spontaneous regression (SR), which has been reported in only 3 other cases (1–3; Table I).
Table I. Cases of spontaneous regression in primary cutaneous diffuse large B-cell lymphoma of leg type
A 66-year-old man presented with a 6-week history of a purple tumour on his left lower leg (Fig. 1a). The patient’s medical history included diabetes mellitus type II, arterial hypertension and chronic venous insufficiency. Fever, night sweats, and weight loss were absent. Histopathology revealed a dense, diffuse infiltrate of immunoblasts and centroblasts admixed with small reactive lymphocytes within the entire dermis. Neoplastic cells showed positivity for CD20, CD79a, PAX5, Bcl-2, Bcl-6, MUM-1 and stained negative for CD3, CD4, CD5, CD8, CD10, CD21, CD30, CD68, cyclin D1, TdT and EBER-1 (Fig. S1). The Ki-67 proliferation index was approximately 90%. Monoclonal rearrangement of immunoglobulin heavy (IgH) chains was found and mutational analysis of exon 5 (p.L265P) of the MYD88 gene showed the point mutation c.794T>C. Whole-body computed tomography ruled out lymph node or visceral involvement and peripheral blood immunophenotyping was inconspicuous. Radiotherapy of the affected skin was recommended. Unexpectedly, 2 months after the diagnostic biopsy the tumour had almost completely and spontaneously regressed (Fig. 1b). Despite almost complete clinical remission a second biopsy was taken. Histopathology revealed dermal fibrosis and a less pronounced atypical lymphoid infiltrate showing an identical immunophenotype in comparison with the initial biopsy. In addition, a predominantly CD8+ T-cell infiltrate was evident (Fig. 2). Therefore, radiotherapy was initiated to achieve full clinical and histopathological remission.
Fig. 1. Clinical course of spontaneous regression in a patient with diffuse large B-cell lymphoma, leg type. (a) Left lower leg before diagnostic biopsy showing a heavily infiltrated, purple coloured, nodular plaque covered by a few scales. (b) Spontaneous clinical regression 2 months after diagnostic biopsy.
Fig. 2. Histopathological examination of a punch biopsy after spontaneous regression. (a) Section showing dermal fibrosis, telangiectatic vessels and numerous melanophages (haematoxylin & eosin, original magnification ×50). (b) CD79a staining shows remnants of neoplastic cells (original magnification ×100). (c) CD8 staining reveals numerous CD8+ T-cells (original magnification ×50).
In all reported cases of spontaneously regressed PCDLBCL-LT histopathology revealed at least scant foci of remnant CD20+ atypical cells, arguing against complete remission and justifying the initiation of a specific therapy (case 1, 3) (1–3). Interestingly, all biopsies performed after SR revealed a T-cell infiltrate. In case 1 the T cells were predominantly CD8+, in case 2 CD4+ and CD8+ T-cells were found, and in case 3 the CD3+ mature T-cells were not specified further (1–3). The current case also revealed a predominantly CD8+ T-cell infiltrate. Therefore CD8+ T cells appear to play a crucial role in SR of PCDLBCL-LT.
Different causative mechanisms, e.g. apoptosis, reactions of the host’s immune system to infections and particular conditions of the tumour microenvironment, such as the presence of inhibitors of metalloproteinases and angiogenesis, may contribute to SR of malignant tumours (1, 4). Modulation of the host immune system to infections (viral, bacterial) and/or traumatic effects including biopsy might play a crucial role regarding SR in non-Hodgkin’s lymphoma (5, 6). Abe et al. summarized the extremely rare cases of SR in aggressive non-Hodgkin’s lymphoma and speculated that biopsy alone may trigger size reduction of the neoplastic lymph nodes (5). Rarely, infections by Epstein-Barr virus (EBV) or measles virus were documented that may have provoked regression of neoplastic lymph node infiltrates (5, 7). These findings underline the hypothesis that the patient’s anti-tumour immunity could be activated by viral infections. EBV infection may improve the prognosis of sporadic Burkitt lymphoma with granulomatous reaction (5, 8). Nevertheless, in none of the PCDLBCL-LT cases showing SR were EBV or other viral infections described.
We report here, for the first time, a point mutation (c.794T>C) in exon 5 of the MYD88 gene in PCDLBCL-LT with SR. Mutations in this gene, a universal adaptor protein involved in activation of the NF-κB and other signal pathways, are frequent in PCDLBCL-LT (9). Pham-Ledard et al. (9) found this mutation in 69% of cases of PCDLBCL-LT. In this cohort clinical features of patients with or without the mutation did not significantly differ (9). Nevertheless, another study of Pham-Ledard et al. (10) including 58 patients showed that MYD88 mutation in PCDLBCL-LT was associated with shorter survival.
In conclusion, the mechanisms and aetiological factors contributing to SR in PCDLBCL-LT have not yet been elucidated, in particular due to the small number of reported cases. The case described here did not reveal any of the potential factors that might contribute to SR of PCDLBCL-LT. It is important to perform careful histopathological investigation in cases of PCDLBCL-LT with SR in order to not miss residual lymphoma in what may clinically appear to be an almost complete remission.


 Click to show fullsize
Click to show fullsize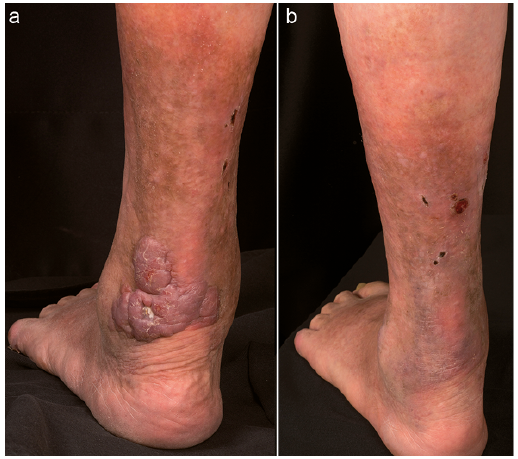 Click to show fullsize
Click to show fullsize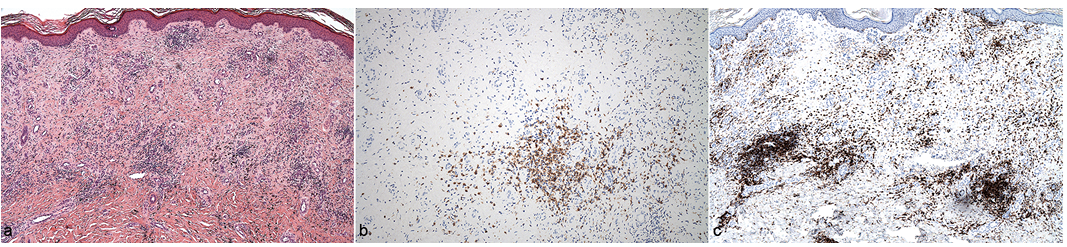 Click to show fullsize
Click to show fullsize