


1Department of Dermatology, Gunma University Graduate School of Medicine, 3-39-22 Showa-machi, Maebashi, Gunma 371-8511, and 2Department of Dermatology, Japan Red Cross Maebashi Hospital, Maebashi, Japan. *E-mail: shimizuakira@gunma-u.ac.jp
Accepted Mar 27, 2018; Epub ahead of print Mar 27, 2018
Calcinosis cutis is a rare complication of the subcutaneous injection of calcium-containing heparin, which mostly occurs in patients with advanced renal failure (1–3). We report here a case of calcinosis cutis at the injection sites of calcium-containing heparin in a patient with systemic lupus erythematosus (SLE) without renal failure.
A 74-year-old man was admitted to our hospital for management of heart failure and bacterial pneumonia. The abnormal laboratory findings were as follows: haemoglobin 6.6 g/dl (normal range 13.2–17.3 g/dl); red blood cell count 240 × 104/μl (420–570 × 104/μl); white blood cell count 3,500/μl (4,000–9,600/μl); brain naturietic protein (BNP) 128.5 pg/ml (0–18.4 pg/ml); C-reactive protein (CRP) 0.9 mg/dl (< 0.1 mg/dl); Na 136 mEq/l (137–145 mEq/l); K 4.1 mEq/l (3.5–4.8 mEq/l); Cl 107 mEq/l (100–107 mEq/l); P 2.5 mg/dl (2.5–4.1 mg/dl); Ca 7.9 mg/dl (8.9–10.5 mg/dl); CH50 < 14.0 U/ml (30.0–46.0 U/ml); C3 22.0 mg/dl (65–135 mg/dl); and C4 2.0 mg/dl (13–35 mg/dl). The patient’s blood urea nitrogen (BUN) and creatinine levels were within normal limits. Laboratory analysis revealed that the patient was positive for anti-nuclear antibodies (anti-nuclear antibody titre 1:1,280; homo-speckled pattern), anti-Sm antibodies (133.5 U/ml (< 7 U/ml)), and anti-RNP antibodies (147.6 U/ml (< 5 U/ml)). The patient was negative for anti-ds DNA antibodies, lupus anticoagulant, anti-cardiolipin β2 glycoprotein I antibodies, and anti-cardiolipin IgG/M antibodies. A cardiac catheter test revealed a mean pulmonary arterial pressure of 28 mmHg (< 20 mmHg). No ultrasound or X-ray was performed to visualize the extent of the calcifications. Based on the findings, the patient was diagnosed with SLE, autoimmune haemolytic anaemia and pulmonary arterial hypertension (PAH).
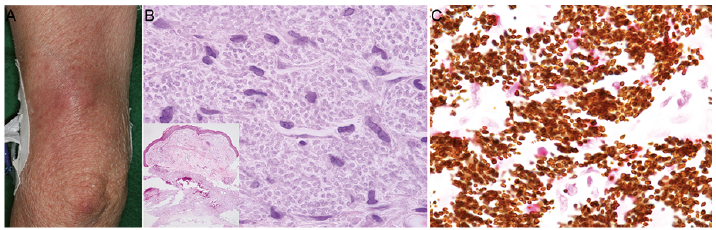
The patient was treated with oral prednisolone (50 mg/day) and one week later, corticosteroid pulse therapy (methylprednisolone sodium succinate (500 mg) for 3 days). At that time, he also received a calcium-containing heparin injection at the extensor surface of the upper arm for 9 days to prevent thrombotic events. Two months later, he noticed several firm, slightly erythematous, painful subcutaneous nodules at the injection sites (Fig. 1A). We suspected lupus erythematosus profundus or granuloma-forming inflammation due to the injection. A skin biopsy from the subcutaneous nodules showed calcium deposits scattered between the dermal collagen bundles of deep dermis. High-power magnification revealed numerous basophilic granules admixed with mononuclear cells (Fig. 1B). Von Kossa staining demonstrated numerous dark-brown granules that were relatively similar in size (Fig. 1C). Transmission electron microscopy revealed needle-like structures and dense amorphous structures, compatible with calcium apatite crystals (Fig. 2). A diagnosis of calcinosis cutis was established based on these histological findings. The patient declined any treatment, and the nodules have shown no significant changes during follow-up.
Fig. 1. Clinical features and histopathology. (A) Indurated erythema at the site of calcium-containing heparin injection. (B) Histopathological examination revealed calcium deposits in the deep dermis (haematoxylin and eosin staining, ×8). High-power magnification revealed numerous basophilic substances (haematoxylin and eosin staining, ×400). (C) Numerous dark brown substances (Von Kossa staining, ×400).
Fig. 2. Transmission electron microscopy revealed multiple structures with a high electron density, admixed with mononuclear cells and fibroblasts (×2,000). High-power magnification revealed needle-like structures and dense amorphous structures, compatible with calcium apatite crystals (×40,000).
Calcinosis cutis is an uncommon condition characterized by the deposition of calcium salts in the subcutaneous tissues. There are 4 types of calcinosis cutis: dystrophic, metastatic, iatrogenic and idiopathic (4, 5). Our case was classified as iatrogenic calcinosis cutis due to the injection of calcium-containing heparin. Calcinosis cutis sometimes occurs in patients with SLE during the disease course (6); this dystrophic type of calcinosis cutis is associated with tissue damage (5). Although the precise pathogenesis in our patient was unknown, both the elevated local concentration of calcium and tissue damage caused by the injection of calcium-containing solutions may trigger the formation of calcium apatite crystals, as reported previously (1, 3). In addition, endothelial damage due to SLE might have also resulted in the deficient absorption of calcium-containing heparin. The time interval between injections and occurrence of symptoms/calcifications of the previous cases ranged from 3 days to several weeks (1–3). In the current case, the lesion developed 2 months after the injection, which took a long time compared with previous cases. It is possible that the difference depends on the disease; most previous cases had severe renal dysfunction, while our case did not. It should be borne in mind that iatrogenic calcinosis cutis can occur following the injection of calcium-containing heparin.


 Click to show fullsize
Click to show fullsize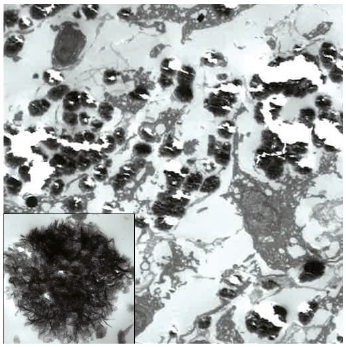 Click to show fullsize
Click to show fullsize