


1Department of Pathology, and 2Department of Dermatology, Venereology and Allergology, Wroclaw Medical University, Wroclaw, Poland
Actinic keratosis (AK) is the most common in situ cancerous skin lesion. Compared with other approved treat-ment modalities photodynamic therapy is preferred by patients due to faster recovery and improved cosmetic outcome. However, pain during irradiation is an important drawback. The aim of this study was to compare the effectiveness and tolerability of topical aminolaevulinic acid-photodynamic therapy in the treat-ment of AK on the head using red and green light. Complete remissions after 3 sessions of photodynamic therapy at 2-week intervals following 9 months of observation were 91.67% for red light and 86.67% for green light (difference not significant). The mean pain value was significantly greater in areas irradiated with red light compared with green light for all 3 sessions. This comparative study demonstrates that aminolaevulinic acid-photodynamic therapy with green light is of similar efficacy as that with red light in the treatment of middle/moderate AK, but causes less pain.
Actinic keratosis is the most common early non-invasive stage of skin cancer. Compared with other approved treatment modalities photodynamic therapy is preferred by patients due to faster recovery and improved cosmetic outcome. However, pain during irradiation is an important drawback. This study shows that 3 sessions of topical aminolaevulinic acid-photodynamic therapy using green light is of similar efficacy as that with red light in the treatment of middle/moderate actinic keratosis, but irradiation with green light caused significantly less pain compared with red light.
Key words: photodynamic therapy; red light; green light, 5-aminolevulinic acid; actinic keratosis; pain.
Accepted Mar 27, 2018; Epub ahead of print Mar 27, 2018
Acta Derm Venereol 2018; XX: XX–XX.
Corr: Jacek C. Szepietowski, Department of Dermatology, Venereology and Allergology, Wroclaw Medical University, ul. Chalubinskiego 1, PL-50-368 Wroclaw, Poland. E-mail: jacek.szepietowski@umed.wroc.pl
Actinic keratosis (AK) is the most common in situ neoplasm of the skin in the white population, particularly in people with skin phototypes I–III. Epidemiological data show a rapid increase in AK morbidity in recent years. Lesions usually present as multiple erythematous or hyperkeratotic yellow, scaly plaques on skin areas damaged by ultraviolet (UV) light (photodamaged skin). Clinical research shows that 1–10% of AKs progress to cutaneous squamous cell carcinoma (SCC).
Common treatments for AKs use various procedures, both ablative (cryosurgery, laser ablation, curettage, and surgery) and topical (5-fluorouracil, diclofenac 3% gel, and imiquimod). Some of these therapies may cause scarring or hyper- or hypo-pigmentation. Because most AKs are found in the sun-exposed skin (face skin, scalp, and hands), therapies offering the best cosmetic results are especially desirable.
Topical photodynamic therapy (PDT) with 5-aminolaevulinic acid (5-ALA) has been approved as an alternative method of treating various precancerous (e.g. AK) and superficial tumours of the skin (1–3). Safety, non-invasiveness, and excellent cosmetic results make PDT competitive with other conventional methods. Clinical studies have shown the effectiveness of ALA-PDT to be comparable to, or even exceed that of, cryotherapy, excisional surgery, or electrodesiccation in the treatment of AK (4–7). Many patients who have previously undergone other FDA-approved treatment modalities for AK prefer PDT because of improved cosmetic outcome and faster recovery compared with cryotherapy and surgical excision. Moreover, PDT is better tolerated than 5-fluorouracil (5-FU) and imiquimod (8).
PDT is based on the interaction between 3 elements: a photosensitizer, an activating light source of the appropriate wavelength and oxygen. 5-ALA is selectively taken up by premalignant or malignant cells. In the target cells it is converted to protoporphyrin IX (PpIX), via the haem synthesis pathway. Exposure to light leads to activation of PpIX, formation of reactive oxygen species (ROS) and cytotoxicity of pathological cells (9). PDT is typically induced by red light because of the optimal depth of light penetration into tissue. However, an important drawback of ALA-PDT is pain, often intense, experienced by patients during irradiation. Several studies have shown that, in the case of patients with AK on the forehead and scalp, PDT causes more pain than in cases of lesions in other areas (10, 11). PDT offers clinical efficacy similar to standard treatments, but pain remains the most common adverse event reported. Therefore, new strategies are being sought in order to minimize discomfort during PDT.
The fact that a variety of wavelengths can initiate photodynamic reactions from ALA via PpIX in cells has led to interest in using green light (which is less penetrating) to treat superficial skin lesions. A number of clinical studies have reported that green light is effective in the treatment of facial AK and Bowen’s disease, while being less painful than red light PDT (12). However, in the only comparative study on the results of treatment of Bowen’s disease using red and green light PDT, green light was found to be less effective (13).
The aim of this study was to compare the effectiveness and tolerability of topical ALA-PDT in the treatment of AK on the head by using red and green light.
This study was approved by the local ethics committee (BW UMW: KB/6-2014) and conducted in accordance with the Declaration of Helsinki. All patients included in the treatment protocol were provided with detailed information about the procedures and aim of the study.
Twenty patients (11 men and 9 women), age range 61–84 years (mean 76 years), with typical clinical (visibly pink-reddish and palpable) AK lesions on the head (face, scalp and forehead) were enrolled in the study. The AKs that qualified for the treatment met the criteria of grade I (mild) or grade II (moderate) according to Olsen et al. (14). Diagnoses of AK were verified histologically. Fifty-four areas of 3×3 cm were chosen, each having at least 2 AKs with a minimum diameter of 0.5 cm. In each patient, 2, 3 or 4 areas were selected according to the above criteria.
The aim of this study was to compare the efficacy of PDT with red and green light using the same procedure, with the same lesion type and location. Patients were randomly assigned to 2 equipotent groups. In group I, half of the areas were irradiated with red light on the left side and the other half with green light on the right side; in group II, the order was reversed. In patients with 3 selected areas, the third area was always irradiated with green light. In total, 30 areas with AK lesions received ALA-PDT using green light and 24 areas using red light.
Each area was treated with 3 sessions of PDT at 14-day intervals regardless of the current clinical stage. For one week before the first PDT irradiation, all patients applied a cream with 30% urea once a night on selected skin areas with AKs. Four hours before exposure to light, lesional areas were treated with 20% ALA (Sigma-Aldrich®, St. Louis, Missouri,US) prepared in an oil-water cream with 2% dimethyl sulphoxide (DMSO) under occlusion. The cream was applied to an 3 × 3 cm2 area. Next, the adhesive patch was removed and the rest of cream was wiped off with a 0.9% natrium saline solution.
The lesions were irradiated with incoherent light from a halogen lamp (Penta Lamps, Teclas, Switzerland) with a proper bandpass filter. Dosimetry was adapted from literature data, where the total dose 62.5 J/cm2 for green light at the wavelength of 540 ± 15 nm corresponds to the total dose of 125 J/cm2 for red light at a wavelength of 630 ± 15 nm (13). The fluence rate for both types of light was 86 mW/cm2. The irradiation was performed in a dark room in a fractionated mode during each session: 3 min of irradiation and 1-min pause (15). No analgesics were given.
The pain experienced by patients treated with green PDT and red PDT was compared during each of the 3 sessions. The intensity of the maximum pain level during the irradiation was evaluated for every area using a numeric rating scale (NRS), graded from 0 (no pain) up to 10 (unbearable pain).
From the next day, the patients were to apply RadioProtect® cream (Aurea Pharma, Nadarzyn, Poland) to all irradiated areas 3 times a day for one week to accelerate the withdrawal of adverse reactions and optimize healing of the epidermis. Moreover, they were to use an SPF 50+ sunblock for the whole period of treatment and follow-up. The use of any topical or systemic analgesics after PDT sessions was not recommended.
Patients returned for follow-up visits at months 3, 6 and 9 after the final ALA-PDT. The areas where the lesions had subsided were all classified as complete remissions. The areas where the surfaces of lesions were reduced, or at least one lesion recurred, were classified as partial remissions.
The Shapiro–Wilk test was applied to analyse population distribution. The Mann–Whitney U test was used to examine differences in pain experience between the groups treated with red and green light. Differences in pain experience of the groups between the successive irradiation sessions were analysed with the Wilcoxon signed-rank test. The Pearson’s χ2 test with Yates’s correction was used for differences in the treatment results between the 2 groups at the follow-ups after 6 and 9 months.
None of the participants discontinued the study because of the adverse effects of PDT. Two patients were not enrolled into the analysis because they did not attend the third PDT session at the appropriate time.
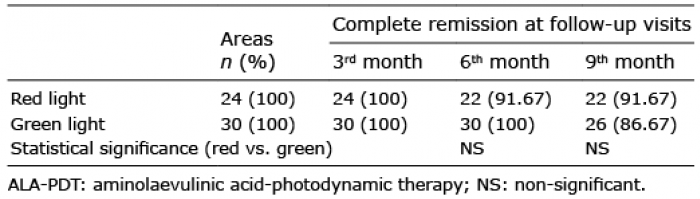
At the first follow-up visit after 3 months, we observed complete remission in all treated areas in both groups (red 100% vs. green 100%). At the second follow-up after 6 months, we observed a recurrence of AK lesions in 2 areas treated with red light (partial response of 91.67%) and no recurrence in areas treated with green light (complete remission of 100%). At the last follow-up after 9 months, 4 new AKs were observed in areas treated with green light. Finally, total response to AK treatment by ALA-PDT following 9 months of observation was 91.67% for red light and 86.67% for green light. No statistically significant differences were found between the groups (Table I).
Table I. Comparison of response to the ALA-PDT treatment at follow-up visits between aktinic keratosis groups treated with red vs. green light
The mean ± SD pain value was greater in areas irradiated with red light compared with green light for all 3 sessions and the differences were significant (p < 0.001, mean visual analogue scale (VAS) score 5.3 ± 1.61 vs. 1.87 ± 1.30 points; 4.58 ± 1.64 vs. 0.70 ± 1.09 points; and 1.92 ± 1.28 vs. 0.13 ± 0.43 points, respectively). We also observed a significant decrease in pain experience in successive PDT sessions in both groups: with red and green light (Table II).
Table II. Comparison of pain experience evaluated with the numeric rating scale (NRS) between actinic keratosis (AK) groups treated with red vs. green light and between the successive irradiation sessions
We did not evaluate the immediate and long-term side-effects. However, anamneses showed erythema and oedema persisting for several days in areas irradiated with red light, especially in patients with greater pain. In the case of green light, no erythema was observed and the slight feeling of skin tension subsided over a period of 24 h. At 3-month follow-up, hyperpigmentation was observed in red light fields in 3 subjects not having regular UV protection. There was no hyperpigmentation in green light fields or any of the patients undergoing follow-ups at 6 and 9 months after treatment.
The main finding of this study is that topical PDT with the use of green light, similarly to red light, is highly effective in the treatment of middle and moderate AKs on the face and scalp. At 9 months, after 3 treatment sessions, the complete response rates were obtained in 91.67% with red light and 86.67% with green light. Similar results showing comparable efficacy of red and green light in the treatment of AKs have been presented in only one paper (12). It has been well proven in the literature that topical application of 5-ALA and its derivative methyl aminolevulinate (MAL), followed by activation with visible light, results in a significant reduction in abnormal lesions (16). Due to the depth of penetration, red light is commonly used in PDT. The overall efficacy rates of AK clearance with PDT range from 75% to 92%. Buinauskaite et al. (17) irradiated patients with AKs in the face/scalp region twice with a 2-week interval, obtaining complete response at 6-month follow-up in 92.1% of lesions for 70 J/cm2 and in 84.2% of lesions for 100 J/cm2. By contrast, Radakovic-Fijan et al. (18) showed that 3 months after one red light PDT session the rate of complete remission varied between 69% and 81% depending on light doses. In the study using topical MAL-PDT, after 2 treatments with a 1-week interval, complete clearance was obtained in 91% of AKs (19).
Data on recurrence rates of AK after PDT are controversial. Some authors report recurrence rates of 28% (between 6 and 12 months) or 30% after a median follow-up period of 13 months (20–23). The high recurrence rates may be explained by use of a single PDT treatment. Some authors believe that a single exposure, which gives approximately 70% clearance rate in clinical examination at 3 months after PDT, is sufficient. Repeat treatments are typically restricted to the lesions that have shown a partial response. In our opinion, all treatments should be repeated. Therefore, we were the first to apply 3 mandatory irradiations of lesions at 2-week intervals.
AKs contain cells with different spectra of molecular and genetic perturbations. If some abnormal keratinocytes are located in deeper layers of the lesions, they may not have received lethal doses of light at the time of first irradiation. Since the migration of keratinocytes from the basal layer to the cornified layer takes approximately one month, our repeated use of PDT at 2-week intervals allows us to destroy atypical cells in accordance with the natural cycle of keratinocyte migration through the entire epidermis. Therefore, repeated light exposure should increase the efficacy of ALA-PDT (24, 25). This should allow us to obtain a high clearance rate with green and red light at 9-month follow-up.
PDT is a process based on free-radical reactions. The oxidative damage within the abnormal cells can induce mechanisms of cytotoxicity, including induction necrosis, apoptosis, and autophagy, which under specific circumstances may also be protective for dysplastic cells (26). The 125 J/cm2 dose used in our study in red light PDT was relatively higher than the doses commonly used in AK treatments, but this may be the reason why we obtained such a good therapeutic effect at 9-month follow-up. The applied dose was taken from a study that treated deeper foci of Bowen’s disease (13). Studies by Kennedy & Pottier (27) confirm a clearance rate of 90–100% for AK/Bowen’s disease when using 150–300 mW/cm2. Other studies have also shown that ALA-PDT for the treatment of dysplastic lesions in the head and neck with the use of higher doses (fluence rate of 100 mW/cm2 and fluence of 100 J/cm2) result in a higher clearance rate (28, 29). Yu et al., in treatment with a standard laser source or light-emitting diode (LED) light, obtained complete remission rates in 96% and 85%, respectively, with a mean follow-up of 32 months (16–72 months) (28).
Red light is usually employed in PDT due to the depth of tissue penetration (30). 5-ALA-induced photosensitivity has a porphyrin-like spectrum with maximum excitation at 410 nm and 4 smaller peaks at 510, 540, 580 and 630 nm (30). The use of green light to treat superficial skin lesions seems particularly attractive. A wavelength of approximately 540 nm penetrates mainly the epidermis, so, in theory, it may be less painful while maintaining full photodynamic effect on the cells. Our previous studies confirm the efficacy and excellent tolerance of green light in the treatment of lichen sclerosus (15). This directed our attention to the possibility of using green light PDT in the treatment of AKs. Apart from 2 studies cited below, the literature lacks comparative studies on the use of red/green light in dermatological clinical practice. In 1997, Fritsch et al. (12) conducted a half-side comparison study on the face and scalp of a small group of 6 patients with AK. After one or, if required, two ALA-PDT treatment sessions, both red and green light were found to be 100% effective. However, green light caused much less pain during the irradiation than red light, thus green light ALA-PDT is superior to standard ALA-PDT. Morton et al. (13) performed a similar research study of Bowen’s disease on a larger group (32 lesions treated with red light vs. 29 lesions treated with green light). The clearance rate at 12-month follow-up after ALA-PDT was 88% for lesions treated with red light and 44% for lesions treated with green light. The authors attribute greater efficiency of green light in AK than in Bowen’s disease to the differences in lesion depth. Although they noted a trend towards red light being more painful than green light, there were no significant differences between the 2 groups in the frequency and severity of the pain experienced.
Pain is the main adverse event in topical ALA-PDT and its pathogenesis is unclear (31, 32). Buinauskaite et al. (33) show that the sex, age of the patient and skin phototype have little or no effect on the intensity of pain during PDT irradiation. However, many factors influence the amount of pain experienced by a patient, especially when he or she is affected by larger AK lesions (10, 33). Induction of inflammation following PDT, the type of photosensitizer, location and type of lesions, intensity of photodynamic processes depending on concentration of PpIX in the affected cells, and also dosimetry and wavelength of the used light may all play a role. Severe lesions, with a high degree of dysplasia, have probably absorbed more ALA, which is why they produce initially high levels of PpIX. Our study has shown that pain intensity during the first irradiation is usually greater than during the following 2 sessions of PDT. A decrease in painfulness, as well as reduction in adverse reactions (reported by patients) may be caused by a gradual decrease in the number of abnormal cells in AK foci, destroyed during successive irradiations, and thus a smaller accumulation of PpIX and weaker photodynamic reactions. Several studies have reported that the first few minutes of irradiation are the most painful. Ericson et al. found that the rate of photobleaching is high at the beginning of a session; therefore, the experience of pain seems to be associated with photodynamic activity (34). Our findings are supported by a study conducted by Sandberg et al. (35), who showed that patients with intense redness (dependent on degree of inflammation) experienced more pain, but that their AK lesions had a higher cure rate. Red light, commonly used in clinical practice, causes pain usually referred to as a burning sensation. Approximately 20% of ALA-PDT patients exposed to a high-output broadband red light source experienced severe pain rated at 7 or above (VAS score) (10, 35). Similar results were obtained by Clark et al. (36), who treated the patients with AK, BD and BCC lesions by using a high-output broadband light source (80–150 mW/cm2 with doses of 50–130 J/cm2). Severe pain experience was reported in 16–21%, but only in 2% of patients irradiated with a low-output broadband light source (20–25 mW/cm2). The energy of red light, which penetrates deeper into the skin, affect the elements present in the corium, including unmyelinated type C nerve fibres. In the case of green light, the effect is superficial (not more than 2 mm into the skin) and covers the epidermis without directly affecting the nerve fibres. This may explain why green light was less painful than red light in the treatment of AK lesions.
Clinical practice relies on various strategies to reduce the level of pain (cooling fan, water spraying, and local analgesia). Our experience demonstrated high efficiency of intermittent irradiation, thanks to which the procedure is relatively well tolerated by the patient. An additional benefit of intermittent irradiation is greater photodynamic activity, associated with partially reversed hypoxia created by ALA-PDT, which should improve the effectiveness of the treatment (37).
In our study, patients experienced pain in varying degrees, depending on the light used. During the first red light PDT session, the maximum VAS pain score was 5.3 ± 1.61 points. On the other hand, the use of green light at a dose corresponding to the effect of red light did not cause any serious pain experience. Patients experienced mild pain scored by VAS as 1.87 ± 1.30 points. Moreover, they described the experience as burning, tingling, or paraesthesia rather than pain. The difference between red and green light was highly significant (p < 0.001).
At 9-month follow-up after PDT light irradiation, AK recurred in 4 patients treated with green light compared with 2 cases treated with red light, suggesting greater efficacy of red light, although the difference was not statistically significant. On the other hand, a recurrence in the red-light fields was observed after 6 months, compared with 9 months for green light. This suggests the opposite: a higher efficacy of green light in the treatment of superficial dysplastic skin lesions. It is interesting that, in our study, the same patients with partial response in AK areas treated with red light also had partial response in areas treated with green light. This may suggest a personal predisposition to poor response to PDT due to low accumulation of PtIX (low enzyme activity of the protoporphyrin IX biosynthesis pathway). A similar observation was made in a study by Fritsch et al. (12), where in the same 2 out of 6 patients there was no therapeutic effect after the first ALA-PDT session with either red or green light.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize