


Department of Dermatology, Faculty of Medicine, University of Tsukuba, 1-1-1 Tennodai, Tsukuba, Ibaraki, 305-8575, Japan. *E-mail: naoko.okiyama@md.tsukuba.ac.jp
Accepted Mar 27, 2018; Epub ahead of print Mar 27, 2018
Subcutaneous panniculitis-like T-cell lymphoma (SPTCL) is a rare type of cutaneous lymphoma accounting for less than 1% of all cutaneous lymphomas. SPTCL is characterized by the infiltration of neoplastic cytotoxic T cells into subcutaneous tissues, which makes it resemble lobular panniculitis. Haemophagocytic syndrome (HPS)/haemophagocytic lymphohistiocytosis (HLH) is sometimes associated with SPTCLs, occurring in approximately 17% of cases (1). On the other hand, visceral involvement is rarely observed in patients with SPTCL (1). We report here a case of a patient with SPTCL who developed bone marrow and lung involvement.
An 82-year-old Japanese man presented with a 6-month history of intermittent fever, non-productive cough, weight loss of 8 kg, and recurrent, multiple and painless subcutaneous nodules and plaques. Because plaques and high-grade fever were intractable despite oral prednisolone, 20–30 mg/day, the patient was referred to our hospital.
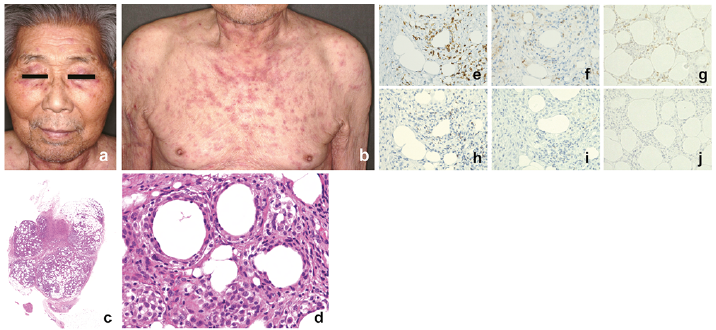
Physical examination revealed plaques, which ranged from 5 to 20 mm in diameter, on the face, neck, upper chest and upper limbs (Fig. 1a, b). Laboratory investigations revealed pancytopaenia (white blood cell count 2.5×109/l (normal range 4.0–9.0 × 109/l); red blood cell count 2,910 × 109/l (4,270–5,700 × 109/l); platelet count 67 × 109/l (150–350 × 109/l)) with prolonged erythrocyte sedimentation rate (81 mm/h), and elevated serum levels of C-reactive protein (6.03 mg/dl), lactate dehydrogenase (441 U/l), ferritin (641.9 ng/ml) and soluble interleukin-2 receptors (sIL-2R) (630 U/ml). Biopsy of the subcutaneous nodule in the left upper limb at the onset of the disease demonstrated lobular panniculitis (Fig. 1c) with infiltrating atypical lymphoid cells with pleomor-phic nuclei (Fig. 1d). Focal rimming of adipocytes by the atypical cells, karyorrhexis and foamy histiocytes were also observed (Fig. 1d). Immunohistochemistry showed that the cells rimming the adipocytes were positive for CD3, CD8 (Fig. 1e), T-cell intracellular antigen-1 (Fig. 1h) and T-cell receptor (TCR)-βF1 (Fig. 1g), and negative for CD4 (Fig. 1f), CD20 (Fig. 1i), CD30, CD56 and TCRγδ (Fig. 1j). TCR-β gene clonal rearrangement was detected by PCR analysis from 2 identical samples of plaques. Bone marrow aspiration smears showed that 8.4% of total cells were atypical large lymphoid cells with enlarged and irregular nuclei. Bone marrow biopsy revealed moderate hypoplastic bone marrow tissue with infiltration of lymphoid cells expressing CD8 in the stromal layer of bone marrow tissue, but without haemophagocytosis (Fig. S1a, b). A chest X-ray revealed bilateral patch areas of consolidation in the middle-lower lung lobes (Fig. S1c), which were confirmed as peribronchial infiltration on computed tomography. Culture of bronchoalveolar lavage fluid, plasma cytomegalovirus pp56, plasma Epstein-Barr virus DNA and interferon-γ release assays for tuberculosis were all negative, and the serum level of β-D-glucan was normal. Transbronchial lung biopsy showed perialveolar infiltration of predominant CD8+ T cells (Fig. S1d, e). Accordingly, we diagnosed the patient as SPTCL with bone marrow and lung involvement.
Fig. 1. Clinical and pathological findings. (a) Plaques around the eyes, and (b) on the neck, upper chest, and upper limbs. Haematoxylin and eosin-stained biopsy specimens of the subcutaneous nodule in the left upper limb showed (c) lobular panniculitis (original magnification ×2) and (d) focal rimming of adipocytes by infiltrating atypical lymphoid cells with pleomorphic nuclei and foamy histiocytes (original magnification ×400). Immunohistochemistry were performed for (e) CD8, (f) CD4, (g) TCRβF1, (h) T-cell intracellular antigen-1, (i) CD20 and (j) TCRγδ. (Diaminobenzidine and haematoxylin, original magnification×400).
After the first course of CHOP chemotherapy (cyclophosphamide 375 mg/m2, doxorubicin 50 mg/m2 and vincristine 1.4 mg/m2 at day 1; prednisolone 100 mg for days 1–5), the symptoms resolved completely within 2 weeks. A total of 6 monthly courses of CHOP were completed, and prednisolone was tapered. Two months later, a relapse occurred, with plaques, pulmonary consolidation and fever despite 7.5 mg/day prednisolone. Administration of oral etoposide (50 mg daily for 3 weeks followed by a rest period of one week) as the second-line chemotherapy with increased dosage of prednisolone to 20 mg/day led to clinical remission again and prednisolone was tapered gradually and stopped. The treatment has completely suppressed recurrences for 30 months.
SPTCL was first described by Gonzalez et al. (2) in 1991 as an uncommon form of cutaneous lymphoma with primary involvement of adipose tissue. Previously, the disease was thought to consist of an α/β TCR phenotype and a γ/δ TCR phenotype. Because γ/δ TCR phenotype have a more aggressive clinical course frequently accompanied by extracutaneous involvement and HPS than α/β TCR phenotype, the World Health Organization - European Organisation for Research and Treatment of Cancer (WHO-EORTCC) classification of 2005 defines SPTCLs as those cases with an α/β TCR phenotype, and established a new category of primary cutaneous γ/δ T-cell lymphoma (CGD-TCL) (3). It was reported that there was no case with visceral involvement out of 63 cases of SPTCL with an α/β TCR phenotype (1). To our knowledge, only 7 cases of SPTCL with extracutaneous involvement have been reported (4–8) (Table SI). The affected sites included bone marrow in 4 cases (5, 6); breast in 2 cases (4, 7); and liver (7), spleen (7) and mesenteric fat (8) in one case each. Only one case had multiple sites of extracutaneous involvement in addition to our case (7).
At present, a standard treatment protocol for SPTCL, especially for cases with visceral involvement, has not been established because of the rarity of the disease. A wide variety of treatment modalities have been reported, including corticosteroids, immunosuppressive agents, combination chemotherapy/radiotherapy, and bone marrow transplantation (1, 9, 10). Anthracycline-based regimes, such as CHOP therapy, were commonly used (9). Because almost all cases with SPTCLs present indolent clinical courses, prednisolone or cyclosporine A monotherapy might be sufficient, as reported recently (7, 11, 12). Five cases with extracutaneous involvement were treated with combination chemotherapy including CHOP therapy (4–6, 8), while 2 cases were treated with cyclosporine A monotherapy (5, 7) (Table SI). Even in cases treated with combination chemotherapies, 4 cases were refractory to the first-line chemotherapies, experienced recurrence or died within 2 months after diagnosis (4–6, 8). Prolonged etoposide monotherapy resulted in long-term remission in our case following a relapse episode after CHOP therapy, while 3 cases were previously reported to experience recurrence after combination chemotherapies including etoposide (5, 6, 8). Chronic daily oral low-dose etoposide therapy is reportedly effective in refractory lymphoma (13). Because the therapy is available on an outpatient basis with mild adverse events compared with combination chemo-therapies, administration of etoposide is also useful and effective in elderly patients with refractory lymphoma (14). The current case is the first reported case of SPTCL with multiple extracutaneous involvement treated with etoposide monotherapy. This case indicates that etoposide might be an effective and safe drug to treat SPTCL patients with visceral involvement.


 Click to show fullsize
Click to show fullsize