


1Department of Traumasurgery, Leiden University Medical Centre, Leiden, 2Burn Centre Beverwijk, Red Cross Hospital, 3Association of Dutch Burn Centres, Department of Behavioural Research, Beverwijk, and 4Department of Clinical Psychology, Utrecht University, Utrecht, The Netherlands
Itch is a common problem after burns. Although the topic receives increasing attention, the number of prospective studies is limited. The aim of this study was to assess the influence of acute traumatic stress symptoms, controlled for injury characteristics, age and sex, on itch over a period of 18 months using multilevel analysis. A total of 226 respondents provided itch scores. Participants completed the Burn Itch Questionnaire during admission (n = 208) and at 3 (n =179), 12 (n =143) and 18 (n =99) months post-burn. They completed the Impact of Event Scale to assess acute traumatic stress symptoms during admission. Skin graft requirement, a higher level of acute traumatic stress symptoms and younger age were statistically significant predictors of a higher itch score. Younger age was particularly associated with higher itch scores during admission, whereas the effect of skin grafting was particularly observed at 3 months post-burn. This study replicates the predictive role of traumatic stress symptoms, which warrants further research.
Itch is a common symptom in burn patients that affects quality of life, and is difficult to treat. Our study assessed which factors can predict the occurrence and severity of itch in burn patients. Two-hundred and twenty-six patients from 5 burn centres in the Netherlands and Belgium were included and provided data via the Burn Itch Questionnaire. We found that age, skin grafting and traumatic stress symptoms are predictors of itch up to 18 months post burn. These findings emphasize the need to understand the interaction between stress symptoms and the presence and severity of itch in burn patients.
Key words: pruritus; itch; burns; scars; predictors.
Accepted Mar 27, 2018; Epub ahead of print Mar 27, 2018
Acta Derm Venereol 2018; XX: XX–XX.
Corr: Nancy E. E. van Loey, Association of Dutch Burn Centres, Department of Behavioural Research, Zeestraat 27-29, 1941 AJ Beverwijk, The Netherlands. E-mail: nvanloey@burns.nl.
Pruritus is a common and impairing problem in patients after burn injury, with a negative impact on quality of life (1–3). Pruritus occurs in the early stages of wound healing as well as years after burn scar maturation. Prevalence rates of burn pruritus are high, affecting up to 87% of patients within 3 months of discharge (4–6). As much as 67–76% of patients experience itch 2 years post-burn, of which 23% is defined as moderate to severe itching (2, 5, 7).
Several demographic factors and injury characteristics were described to be associated with itch in burn patients. Female sex and younger age are associated with the presence and severity of itch (1, 5, 7, 8). The most consistent injury characteristic associated with higher itch scores is the percentage total body surface area (TBSA) burned (1, 5, 9, 10). Furthermore, some studies have shown that an increase in TBSA burned is associated with a higher itch severity (1, 2, 5–7, 11). Other injury characteristics associated with the severity of itch include grafted areas, a higher number of surgeries and a longer time to wound healing (1, 5, 12).
Four studies have investigated the influence of psychological factors on the occurrence and severity of itch (2, 5, 10, 13). The presence of acute traumatic stress symptoms was predictive of itch up to 2 years post-burn in a prospective cohort of 510 burn patients (5). A cross-sectional study including 67 burn patients 2–7 years post-burn found no association between post-traumatic stress symptoms and itch, but personality traits, such as aggression and social desirability, were associated with more severe pruritus (2). A cross-sectional study of 161 burn patients, on average 11 years post-burn, found that persistent pruritus was positively associated with submissive personality traits and less support seeking, while occasional pruritus was associated with anxiety (10). An experimental study including burn patients with chronic itch reported a heightened sensitivity to itch stimuli and found that patients who experienced post-traumatic stress symptoms displayed higher levels of itch (13).
Overall, although burn severity and a younger age consistently showed an association with itch, the evidence for the role of sex and psychological variables remains scarce. Moreover, only 3 of the above-mentioned studies used a prospective design and only one study investigated both demographics, burn severity characteristics and psychological factors as predictors of itch over time (2, 5, 10). Therefore, the purpose of this study was to replicate an earlier study that showed an effect of acute stress symptoms on chronic itch, controlled for the influence of injury characteristics, age and sex, over a period of 18 months using multilevel modelling.
The study was approved by the ethics committees of the Martini Hospital in Groningen, the Netherlands, and of Ghent University Hospital, Belgium. The study was conducted according to the principles of the Declaration of Helsinki. It is part of a larger prospective study that examined psychological problems and quality of life after a burn injury. The data on itch were previously used in a descriptive study in which grafted burns were compared with spontaneously healed burns (9).
Patients were recruited in 5 regional burn centres in the Netherlands and Belgium between January 2005 and January 2009. Inclusion criteria were: patients 18 years or older, length of hospital stay at least 48 h and TBSA burned at least 1%. Exclusion criteria were insufficient Dutch language proficiency, cognitive disorders that prevented reliable data collection, and self-inflicted burns.
Participants were asked to participate in the study by a local researcher who provided oral and written information on the study. After the participants provided written informed consent, they were asked to complete a self-report questionnaire during admission and at 3, 12, and 18 months post-burn. After discharge, the questionnaires were sent to their home address and included a self-addressed stamped reply envelope.
Demographic and injury characteristics. Characteristics such as sex, age (in years) at the time of burn, percentage TBSA burned, skin grafts needed (yes/no) and cause of the burn were derived from the patient record.
Pruritus. The Burns Itch Questionnaire (BIQ) was used to assess itch. The BIQ is a 22-item self-report questionnaire assessing itch intensity and impact on the quality of life (14). For the purpose of this study the overall itch intensity score (10-point rating scale, with 0 indicating no itch and 9 indicating the worse itch imaginable) was used as the dependent variable in the model.
Traumatic stress symptoms. The Impact of Event Scale (IES) is a 15-item self-report questionnaire used to assess symptoms of intrusion and avoidance, 2 central features of posttraumatic stress disorder (12). The frequency of the items is scored on a 4-point scale (0–1–3–5). The total score can range between 0 and 75 and indicates the severity of traumatic stress symptoms. The Dutch validated questionnaire was used in this study (15). The scale was completed during admission.
First, to compare the participants with complete follow-up to those lost to follow-up, Student’s t-tests were used for continuous variables and χ2 tests were used for categorical variables. Secondly, correlation coefficients between the itch scores over time and the predictors were calculated. Spearman’s rho was used for categorical variables, whereas Pearson correlations were used for numeric variables. Thirdly, to investigate the course and predictors of itch, multilevel analysis was used. This type of analysis can address variables in a dependent data structure, i.e. the 4 itch measures are nested within one person and are therefore related. Multilevel analysis takes this dependency into account. It enables examination of different effects that influence itch: (i) a time effect (e.g. a decrease in itch over time); (ii) a person-related effect (e.g. sex may be a factor that influences itch); (iii) an interaction effect between person-related factors and within-time variables (e.g. a higher TBSA burned may be related with higher itch scores over time). As multilevel analysis does not require equal numbers of observations, also cases with missing values can remain in the analysis. In other words, all available observations are used in the analysis.
Our data had a 2-level hierarchy with the repeated itch scores on the first level and the person-related predictors, such as sex, on the second level. A linear mixed effects model with a random intercept and analysis of covariance was estimated. The covariance structure for the random intercept or level 1 was set at variance components (VC) identity covariance structure, which is the default in SPSS. With only an intercept and no slope the VC covariance is the same as an identity matrix. This matrix assumes a constant variance estimate for the intercepts and no covariance between the intercepts. The 4 itch measurements were used as the dependent variable in the models. Time was entered in the model as a fixed effect with 4 categories. Two types of covariance structure were investigated (2 models): (i) Diagonal in which the variances are all different and independent and the co-variances are zero; (ii) AR(1) in which the co-variances between each measurement of the observations get weaker over time. The variances are equal (homogeneous). Overall fit of the models was tested by comparing the –2 Log Likelihood, first-order autoregressive (AR1), Akaike’s information criterion (AIC) and Schwarz’s Bayesian criterion (BIC). A lower AIC and BIC indicates a better fit of the data to the respective models. All statistical analyses were performed using SPSS 24.0. Level of statistical significance was set at p < 0.05.
Itch scores were provided by 208 (92%) patients during admission and by 179 (79.2%), 143 (63.3%) and 99 (43.8%) patients at 3, 12 and 18 months post-burn, respectively. Itch scores of 226 patients were used in the multilevel analysis. Younger patients were more often lost to follow-up at 12 months (t(224)=2.303, p = 0.022) and 18 months (t(224) = 2.403, p = 0.017). There were no statistically significant differences with regard to sex, TBSA burned and needing skin grafting. To assess possible differences within complete vs. incomplete itch series as a function of missing data, respondents with partially missing data were compared with respondents who completed all itch assessments at T1 and T2 using t-tests. Respondents with complete data did not differ from respondents with partially missing itch data at T1 (mean itch complete cases = 2.49 vs. mean itch partially missing cases = 2.66, p = 0.61) and T2 (mean itch complete cases = 2.10 vs. mean itch partially missing cases = 2.28, p = 0.64). It suggests that missing data did not depend on the level of itch.
The mean ± standard deviation (SD) age of the 226 patients upon inclusion was 40.4 ± 13.7 years (range 17–76); 78% of the patients were men. A total number of 134 patients (59%) required one or more operations. TBSA burned was 12.7 ± 12.1% (range 1–65%). The cause of burn was flame in 80% and scald in 20% of the patients. The prevalence of itch during admission, at 3, 12 and 18 months post-burn was 70.2%, 54.2%, 37.1% and 35.4%, respectively. Itch scores during admission, at 3, 12 and 18 months post-burn were 2.60 ± 2.47, 2.20 ± 2.58, 1.16 ± 1.86 and 0.93 ± 1.61, respectively. IES score during admission was 15.8 ± 14.9 (range 0–71).
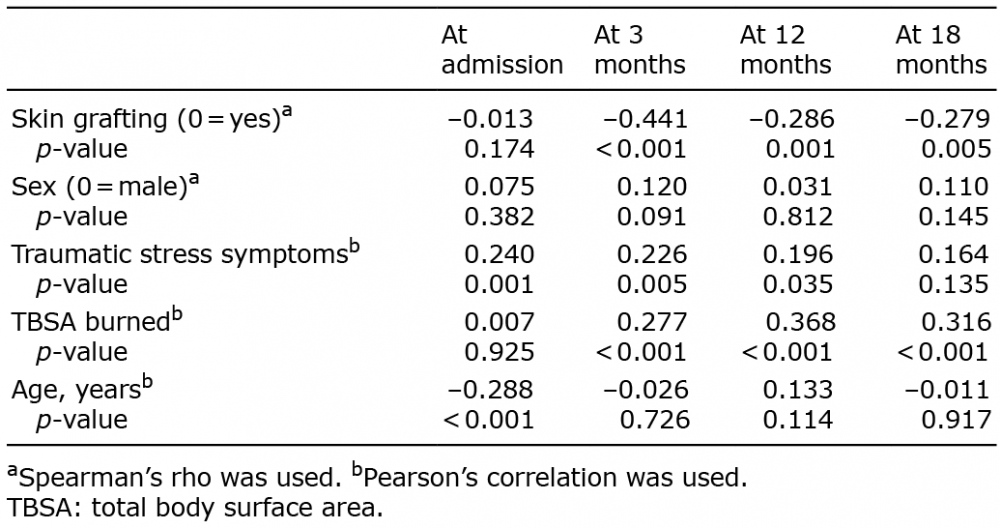
Table I presents the univariate correlation coefficients across the variables used in the model. Sex was not correlated with the overall itch intensity score at any time point. Age was negatively correlated with itch score during admission, indicating that younger persons reported a higher itch intensity during admission. Statistically significant positive correlations were found between burn severity (i.e. needing skin grafting, TBSA burned) and itch score at 3, 12 and 18 months post-burn, but not during admission. The highest correlation was 0.441 and was observed for skin grafting and itch at 3 months post-burn, indicating that more severely burned patients reported a higher itch intensity. Traumatic stress symptoms were statistically significantly positively correlated with itch during admission, at 3 and 12 months post-burn, but not at 18 months post-burn.
Table I. Correlations between injury characteristics and demographic and psychological predictor variables and itch during admission and at 3, 12 and 18 months post-burn
The repeated itch scores of each subject over time constitute the dependent variable in the model. This time-level is the lowest level. On the higher level, i.e. the person-level, are variables that may predict itch patterns. The following predictor variables were entered into the multilevel model: age (in years), sex (male/female), needing skin grafting (yes/no), TBSA burned (%), and the total IES score indicating the severity of acute traumatic stress symptoms. The amount of variance was assessed at the time-level and the person-level. This was statistically significant, justifying a 2-level model. The assessment during admission and the 3 and 12 months post-burn assessments were compared with the measurement completed at 18 months (i.e. reference point).
Two models with different covariance structures for the residuals were tested. Table II presents the fit indices of the models with a diagonal and AR1 covariance structure. The model with the diagonal structure provided a better model fit compared with the AR1 covariance structure, i.e. AIC and BIC were lower. Model 1 included the 5 predictors and Model 2 included 5 predictors and 2 interaction terms. The addition of the interaction terms skin grafting and age increased the explained variance at time level (15.5% to 25.6%), while the variance explained at individual level remained the same (27.9% to 25.9%), justifying the addition of the interaction terms.
Table II. Model comparison with 2 different covariance structures
Table III presents the estimates of the multilevel analysis with the 5 predictors. First, the different measurements of itch were all statistically significant, indicating that, on average, itch levels decreased over time. Patients who needed skin grafting, patients experiencing a higher level of traumatic stress symptoms and younger persons had a higher itch-score. Sex and TBSA burned were not predictive of itch. Table IV shows the estimates of the multilevel model with the 5 predictors and the interaction terms with time of the 2 variables that produced statistically significant predictors. The interaction terms showed that patients needing skin grafting had higher itch levels 3 months post-burn and younger persons had higher itch during admission.
Table III. Multilevel analysis for variables predicting itch over time
Table IV. Multilevel analysis for variables predicting itch over time including interaction terms
This study assessed the possible influence of injury characteristics, demographic factors and acute traumatic stress symptoms on post-burn itch patterns over 18 months using multilevel modelling. Younger patients experienced more itch. This effect was particularly present during admission. Sex was not predictive of itch. Patients who needed skin grafting were more likely to develop itch up to 18 months post-burn. The largest effect of skin grafting was observed 3 months post-burn. Furthermore, patients who experienced acute traumatic stress symptoms were more likely to develop itch, and this effect showed to be relatively stable over time.
The association between younger age and higher itch scores is consistent with earlier findings in burn patients (1, 7) and was also described in relation to other skin diseases (16). Casaer et al. (1) suggests that the lower itch score in older burn patients might be due to a lower concentration of mast cells (17), as an increased release of histamine from mast cells is considered a major contribution during the wound healing phase (18, 19). The finding that men and women had similar itch scores is consistent with the study by Willebrand et al. (10), but in contrast to 2 studies that found a significant positive association between female sex and itch up to 6 months post-burn (5, 7). Differences in injury characteristics and sample size across earlier studies may contribute to the inconsistent results.
The current study showed that needing skin grafting is a predictor of itch, with the highest itch scores reported at 3 months post-burn. The temporal distinct effect at 3 months may be attributed to the active scar maturation phase at that time, which only starts to improve after 6 months post-burn (20). The association between skin grafting and increased itch intensity confirms the findings of previous research (7). This is underlined by the finding that reinnervation of nerve fibres in skin grafts after burns showed a higher substance P nerve fibre density, which is associated with histamine-mediated pruritus for which antihistaminic therapy is indicated (21). However, post-burn itch is often resistant to antihistamine treatment or seems to have a limited effect over time (6). Recent literature shows promising effects of gabapentin in the treatment of post-burn pruritus (22). This might suggest a neuropathic path or central/peripheral sensitization proposing that peripheral nerve injury can lead to dysfunction in neural activity (19). Since grafted burn wounds concern deep partial and/or full thickness burn wounds, the nerve endings are more affected than in superficial and mid-dermal burns. Hence, possible neuropathic factors caused by peripheral nerve injury might play a role during this phase. However, preliminary findings of the study by van Laarhoven et al. (13) could not indicate a central mechanism associated with chronic itch after burns. More research is needed into the pathogenesis of acute and chronic itch in burn scars to elucidate underlying mechanisms. As reviewed by Ständer et al. (23), there are various pruritogenic mediators that affect nerve fibre activation, sensitization and reinnervation. Understanding these processes in the healing phase may be interesting to explore.
Another finding of this study was that patients experiencing traumatic stress symptoms were more likely to develop chronic itch. This replicates the findings of an earlier prospective study (5) and supports results from an experimental study showing that years after injury patients with post-traumatic stress symptoms report higher itch scores in response to histamine-evoked itch (13). A possible explanation for the association between traumatic stress symptoms and itch may be that the immediate stress response to the burn injury initiates a cascade of hormonal and immunological processes that alter cytokine profiles in the wound causing a delay in wound healing (24). Delayed wound healing is associated with a higher itch score and can lead to more severe scarring (6, 25). Our study suggests an effect of psychological stress already active during the wound healing phase that could continue for months. Another explanation may be that patients experiencing traumatic stress symptoms have a heightened attention to trauma-related triggers. However, an experimental study did not find unequivocal support for this explanation (13).
A major strength of our study includes the use of a multilevel analysis to correct for intra-personal correlations over time. Multilevel models are particularly appropriate for longitudinal designs in which repeated measures are correlated. To our knowledge this is the first study on this topic that applied multilevel analysis, strengthening the existing evidence. Secondly, this study replicates earlier findings that indicated the impact of traumatic stress symptoms on chronic itch. Further research is warranted to explain this association on a biological level. Our study has some limitations. First, although the sample size of our study population was relatively large, with 226 respondents, only 44% of them completed the questionnaire at 18 months post-burn. Although in multilevel analyses all the available observations are used, there is a risk of unknown bias. Lastly, the aim of this study was to replicate existing evidence, particularly related to traumatic stress symptoms. As such, no new predictors were investigated.
In conclusion, this study confirmed that age, skin grafting, and traumatic stress symptoms are significant predictors of itch following burns up to 18 months post-burn. The replication of the effect of traumatic stress symptoms on itch in this new sample emphasizes the need to understand the interaction between stress and susceptibility to itch.
This study was funded by the Dutch Burns Foundation, grant numbers 03.90, 04.2012 and 11.101. This study is the result of collaborative efforts of the psychosocial research group represented by Mr M. Bremer and Mrs G. Bakker, Martini Hospital Groningen; Mrs A. Boekelaar, Red Cross Hospital Beverwijk; Mrs H. Hofland, MSc and Mrs A. van de Steenoven, Maasstad Hospital, Rotterdam; Mrs A. S. Goemanne, Ghent University Hospital, and Mrs K. Joos, ZNA Stuivenberg Antwerp.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize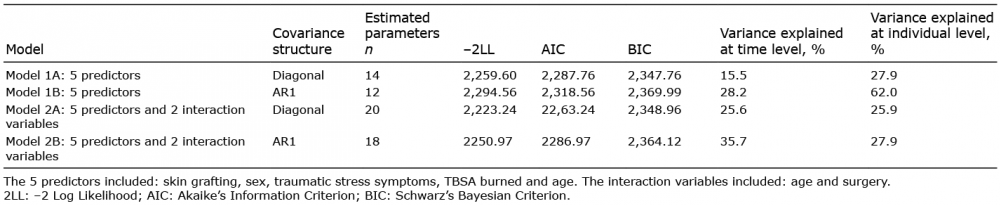 Click to show fullsize
Click to show fullsize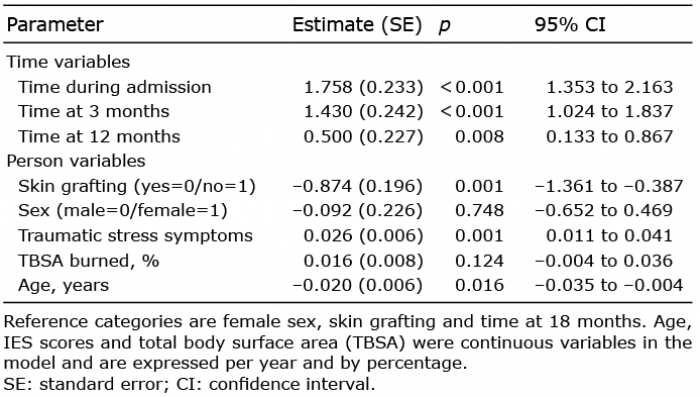 Click to show fullsize
Click to show fullsize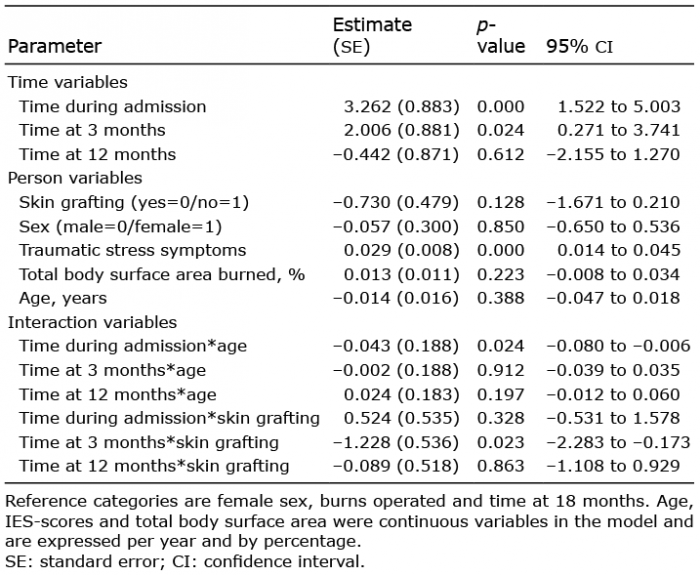 Click to show fullsize
Click to show fullsize