


1Department of Dermatology and Allergology, Room G02.124, and 2Department of Internal Medicine, University Medical Center Utrecht, NL-3508 GA Utrecht, The Netherlands. E-mail: l.f.m.ariens@umcutrecht.nl
Accept Mar 27, 2018; Epub ahead of print Mar 27, 2018
Topical corticosteroids are widely used in the treatment of chronic inflammatory skin diseases, including atopic dermatitis (AD) (1). Long-term treatment with potent topical corticosteroids can have systemic effects due to percutaneous corticosteroid absorption (2). Potentially serious systemic effects include Cushing’s syndrome and suppression of the hypothalamic-pituitary-adrenal (HPA) axis (3). Prolonged suppression of the HPA-axis may result in tertiary adrenal insufficiency caused by adrenal atrophy, which is a potential life-threatening disorder (3). The risk of tertiary adrenal insufficiency depends on several factors, e.g. age, the quantity and potency of the topical corticosteroids, the extent of the treated body surface, the condition of the skin (barrier) at the time of application, and the use of concomitant (corticosteroid-containing) drugs. Topical corticosteroid-induced HPA-axis suppression has been described; however, the development of symptomatic adrenal insufficiency is rare (4–6).
We report here a case of clinically relevant adrenal insufficiency as a result of abrupt discontinuation of topical corticosteroid treatment in a patient treated successfully with dupilumab for severe AD.
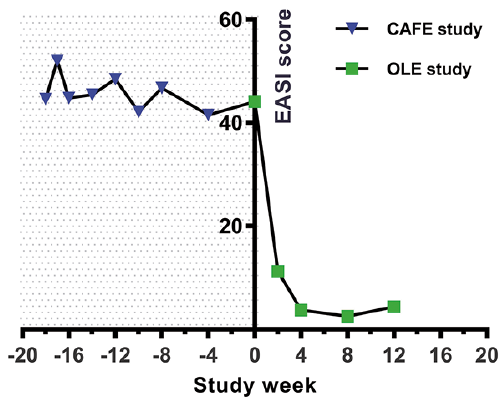
A 50-year-old man with a history of inflammatory bowel disease, anxiety disorder and hypertension was treated at our clinic for severe AD. Relevant medication use included fluoxetine (40 mg/day) for panic attacks. He had uncontrolled AD, despite treatment with potent topical corticosteroids in both outpatient and inpatient settings and treatment with various oral immunosuppressive drugs. Treatment with cyclosporine A (CsA) was effective, but had to be discontinued after several months due to kidney failure. Enteric-coated mycophenolate sodium and, subsequently, azathioprine were discontinued after >12 weeks of treatment due to ineffectiveness. After discontinuation of extended-release tacrolimus because of side-effects, the patient was treated with high-potency topical corticosteroids and systemic corticosteroids. Severe, difficult-to-control AD was the motivation to participate in a phase 3 double-blind, placebo-controlled trial investigating the efficacy, safety and tolerability of dupilumab in patients with severe AD that was inadequately controlled or ineligible for treatment with CsA (CAFÉ study) (7). Treatment with systemic corticosteroids was gradually tapered over several weeks and stopped 24 weeks before the start of dupilumab. At baseline, the patient had a severe, generalized AD with an Eczema Area Severity Index (EASI) score of 44.60. During the 16-week treatment period, the patient was treated with placebo without clinical response (Fig. 1). In this period, the patient used medium-to-high-potency topical corticosteroids (mainly betamethasone dipropionate 0.05% ointment) 1–2 times daily with a mean amount of 150 g/week. After completing the 16-week treatment period, the patient participated in the Open-Label Extension (OLE) study in which he was treated with 300 mg dupilumab weekly. Four weeks after enrollment, disease severity improved significantly (EASI 3.70) (Fig. 1). The rapid clinical improvement was followed by abrupt cessation of self-supplied topical corticosteroids. Two weeks after discontinuation of topical corticosteroids the patient presented at our clinic with flu-like symptoms, including dizziness, pains in the joints and muscles, lack of appetite and fatigue, suspected for adrenal insufficiency. The patient’s morning serum cortisol level was 69.1 nmol/l (normal 09.00 h plasma cortisol 150–802 nmol/l), which was consistent with suspected HPA axis suppression (8).
Fig. 1. Eczema Area and Severity Index (EASI) score during the CAFÉ and Open-Label Extension (OLE) studies.
The patient was diagnosed with symptomatic tertiary adrenal insufficiency as a result of abrupt discontinuation of long-term use of topical corticosteroids after successful treatment with dupilumab. As recommended by the endocrinologist, oral hydrocortisone (40 mg/day) was started at a tapering dose and the patient received instructions considering dosing hydrocortisone in periods of physical and emotional stress. Treatment with dupilumab was successfully continued and the patient clinically recovered from adrenal insufficiency after a few days of treatment with hydrocortisone. Hydrocortisone treatment could be tapered over a period of 6 months. After discontinuation of hydrocortisone treatment adrenocorticotrophin (ACTH) stimulation testing showed recovery of the HPA axis.
In this case, several risk factors may have contributed to the development of symptomatic adrenal insufficiency. As impairment of the skin barrier facilitates the percutaneous absorption of topical corticosteroids and the potential for adrenal suppression, severity of AD and application of potent corticosteroids on large body surfaces may have increased the risk of adrenal insufficiency in this patient. In addition, the patient was treated with fluoxetine for panic attacks, which is a moderate CYP3A4 inhibitor. Corticosteroids are mainly metabolized in the liver by CYP3A4, and concomitant use with CYP3A4 inhibitors might prolong the effect of corticosteroid medications and therefore increase the risk of adrenal insufficiency.
Adrenal insufficiency in this patient became clinically significant after abrupt cessation of long-term applied potent-topical corticosteroids following very strong and fast effect of dupilumab. Dupilumab is a fully human monoclonal antibody against the IL-4 receptor, inhibiting the IL-4 and IL-13 signalling pathways and is the first biologic systemic treatment for AD. Recent phase 3 studies have shown promising results of dupilumab in the treatment of moderate to severe AD (7, 9). After recent approval by the US Food and Drug Administration (FDA) and the European Commission (EC), dupilumab will be broadly available and hence be used on a wider scale in the management of moderate-severe AD. Treatment with dupilumab may result in fast and strong clinical disease improvement in the majority of patients, resulting in rapid tapering or abrupt discontinuation of topical corticosteroid treatment. Especially patients with severe AD, using large amounts of potent-topical steroids are at risk for developing clinical significant adrenal insufficiency. In these patients, it may be considered to evaluate the risk of adrenal insufficiency by assessing morning serum cortisol levels before discontinuation of topical cortico-steroid treatment. If the HPA-axis is completely suppressed, reflected by non-measurable serum cortisol levels, the risk of tertiary adrenal insufficiency is significant and patients should receive instructions considering extra dosing of hydrocortisone in periods of stress.
In conclusion, with the availability of new successful and strong-acting systemic treatment options for AD, such as dupilumab, physicians should be aware of the risk of tertiary adrenal insufficiency as a result of prolonged HPA axis suppression by long-term use of (potent) topical corticosteroids. Patients should be informed about the risk and symptoms of adrenal insufficiency, and testing should be considered, especially in patients at higher risk or those presenting with non-specific symptoms.
Funding sources: The patient described in this case report participated in 2 phase III dupilumab clinical trials sponsored by Regeneron.
Conflicts of interest: MSdB-W is principal investigator, advisory board member, and consultant for Regeneron Pharmaceuticals, Inc. and Sanofi Genzyme; and principal investigator and advisory board member for AbbVie. The other authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize