


1Department of Clinical and Experimental Medicine – Section of Dermatology, 2Department of Adulthood and Childhood Human Pathology “G. Barresi” – Otorhinolaryngology and Auditory Microsurgery Unit, University of Messina, Messina, Italy
Psoriasis is a systemic inflammatory disorder associated with many other chronic and progressive diseases. There are few studies on the association of psoriasis with alterations in auditory function. A clinical and instrumental pilot study of auditory function was performed with 77 psoriatic patients and 77 age- and sex-matched healthy controls. The main results were: (i) hearing loss, mostly of sensorineural type, was significantly more frequent in patients than in controls; (ii) conductive and mixed hearing loss were more frequent in arthropathic than in non-arthropathic psoriatic patients; (iii) duration of psoriasis > 10 years or smoking were associated with higher frequency of hearing loss; (iv) psoriasis was more severe in patients with hearing loss than in those without hearing loss. Tympanogram abnormalities were found in patients more often than in controls. These data expand the list of extracutaneous conditions associated with psoriasis, and support the need for further basic and clinical research in this field.
Psoriasis is a systemic inflammatory disorder associated with many chronic and progressive diseases. This study investigated auditory function in 77 psoriatic patients and 77 age- and sex-matched healthy controls. Overall, hearing loss and alterations of tympanogram are more frequent among psoriatic patients. Patients with psoriatic arthropathy suffer from hearing loss more often than non-arthropatic ones. Hearing loss is also more frequent when psoriasis lasts for more than 10 years and among smokers. Finally, psoriasis is generally more severe in patients with hearing loss. These data expand the list of extracutaneous conditions associated with psoriasis.
Key words: psoriasis; ear involvement; hypoacusis; metabolic syndrome; psoriatic arthropathy; sensorineural hearing loss.
Accepted Apr 12, 2018; Epub ahead of print Apr 12, 2018
Acta Derm Venereol 2018; XX: XX–XX.
Corr: Francesco Borgia, Department of Clinical and Experimental Medicine – Section of Dermatology, University Hospital “G. Martino”, via Consolare Valeria n°1, IT-98125 Messina, Italy. E-mail: fborgia@unime.it
Psoriasis, which for a long time was considered exclusively cutaneous, is now recognized as a systemic inflammatory disorder that shares pathogenic pathways with many chronic and progressive diseases (1). The constantly updated list of these conditions includes psoriatic arthritis, metabolic syndrome or single components of the syndrome, cardiovascular diseases, inflammatory bowel diseases, uveitis, obstructive sleep apnoea, non-alcoholic fatty liver disease, and psychiatric disturbances (2–5). The external ear is commonly involved in psoriasis (6), with typical psoriatic lesions usually present at the conchal bowl as intensely itching, well-demarcated, erythematous plaques with a silvery scale. Ear psoriasis may sometimes appear as non-specific erythematous, dry, and scaly skin; nevertheless, diagnosis is easy when typical lesions are detectable in other areas of the body (7, 8). Interestingly, despite the high prevalence of clinical manifestations involving both the auricle and the external auditory canal, the potential impact of psoriasis on the function of the auditory system has, until now, been little studied. Only 2 cases of sudden-onset autoimmune sensorineural hearing loss have been reported in patients affected by psoriatic arthritis, and there is a lack of data about possible morpho-functional alterations of the external and middle ear and hearing impairment (9, 10). This pilot study aimed to assess the possible presence of hearing loss in a population of psoriatic patients. In addition, a qualitative and quantitative evaluation of clinical manifestations and functional impairment of the external auditory canal and/or tympanic membrane was performed in these patients, via examination and instrumental measurements.
A case-control study was performed on out-patients aged 18 years or over, who attended our dermatological centre for observation due to psoriasis. None of the patients had been treated with systemic drugs for psoriasis in the last 3 months (topical treatments were allowed), and none had a history of otological diseases (genetic hearing loss, head injuries, otological surgery, exposure to ototoxic agents, acoustic traumas or professional/particular noise exposure, chronic external otitis, recurrent middle ear infections requiring otological surgery). As a control group, we considered an equal number of sex- and age-matched subjects with negative personal and family history of dermatological diseases, and without any possible concurrent causes of auditory impairment, as listed above. Severe cardiovascular problems, namely class 3 or 4 heart failure according to the New York Heart Association (NYHA) classification, were exclusion criteria for psoriatic patients and controls. None of the subjects included in the study used hearing aids.
After obtaining approval from our institutional review board and written informed consent from participants, for each patient a dermatologist recorded the duration of psoriasis, smoking and alcohol intake, Psoriasis Area and Severity Index (PASI) score, Dermatology Life Quality Index (DLQI), body mass index (BMI) and comorbidities (arthropathy, obesity, metabolic syndrome). Psoriatic arthritis was diagnosed in collaboration with a rheumatologist. Obesity was diagnosed, in line with WHO criteria, if BMI was 30 or higher. Metabolic syndrome was diagnosed in the presence of 3 or more criteria of the National Cholesterol Education Program’s Adult Panel III (ATP III) (11). All non-dermatological parameters were also recorded for control subjects. Dermatological examination of the external auditory canal (EAC) was performed, and its status was assessed using an arbitrary 4-level clinical scoring system, based on the presence of desquamation, earwax and stenosis: grade 0 = no alteration; 1 (mild) = conchal desquamation; 2 (moderate) = presence of EAC desquamation and/or earwax; and 3 (severe) = stenosis (due to EAC desquamation and/or earwax).
Otological visit and tests were performed within 7 days after the dermatological enrolment visit. First, the status of the tympanic membrane was evaluated by otomicroscopy, a diagnostic method that enables examination of the external ear and tympanic membrane at high magnification by use of a Zeiss OPMI pico otomicroscope (Zeiss, Oberkochen, Germany). This examination was performed in all patients before hearing assessment. Tympanic membrane involvement was scored visually by the same otorhinolaryngologist in both patients and controls, to reduce the risk of subjective interpretation. The involvement of tympanic membrane was scored using an arbitrary 4-level (0–3) clinical scoring system: grade 0 = no involvement; 1 (mild) = retraction; 2 (moderate) = retraction plus opacity and/or scaling of the epidermal layer; 3 (severe) = sclerosis (thickening of the tympanic membrane due to alterations of its 3 layers).
Audiometric tests were carried out by an audiometrist in a sound-proof cabin with Audiometer AMPLAID 171 (Inventis Biomedica, Padua, Italy), and the results were evaluated by an otorhinolaryngologist according to the normative hearing data of the WHO. The audiometrist and the otorhinolaryngologist were not informed whether the subject examined was a psoriatic patient or a control. Pure-tone threshold (the softest sounds that a person hears, at each frequency, approximately 50% of the time) was analysed for both air and bone conduction. The degree of clinical hearing loss was classified according to the normative hearing data of the WHO and based on a 4-frequency pure-tone average (500, 1,000, 2,000 and 4,000 Hz) (12). Hearing thresholds (HT) < 25 decibel (dB) were considered within age-independent normal limits. According to HT, patients were subdivided in 2 groups: Hearing Loss Patients (HLPs, HT ≥ 25 dB) and No Hearing Loss Patients (NHLPs, HT 25 dB). Mild hearing loss ranged from > 25 to 40 dB; moderate hearing loss from >40 to 70 dB, severe hearing loss from >70 to 95 dB, and profound hearing loss >95 dB. Audiological data were also analysed using age- and sex-adjusted determination of hearing loss based on 95th percentiles (HL95) at mean frequencies of 500, 1,000, 2,000, 4,000 Hz, as described by Morrel (13). Compliance of tympanic membrane (tympanometry) was analysed with the impedance meter AMPLAID 775 (Inventis Biomedica). The origin of the hearing deficit, either conductive or sensorineural (cochlear, retrocochlear), was defined through the combined interpretation of audiometric evaluation (conductive component in case of air-bone gap > 15 dB) and impedance audiometry results.
Statistical analysis was performed using Microsoft Excel 2007 (Microsoft, Redmond, WA, USA). The primary endpoint of the study was to evaluate hearing loss in psoriatic patients. Secondary endpoints were: (i) qualitative and quantitative assessment of clinical manifestations and functional impairment of external auditory canal and/or tympanic membrane in these patients; and (ii) correlation of clinical/instrumental otological parameters with clinical parameters of psoriasis.
Because of the lack of previous studies on morpho-functional alteration of external and middle ear and hearing impairment in psoriatic patients (with the exception of the 2 case reports mentioned earlier), it was not possible to calculate statistics based on the estimate of expected differences between patients and controls.
Results were expressed as mean ± standard deviation (SD) in case of continuous quantitative variables (after verifying normal distribution of data through the Kolmogorov-Smirnov test), and frequency of each value for qualitative variables. Correlation analysis was performed by Spearman’s rank correlation test. Study population was then stratified based on age, obesity/BMI, smoking habit, PASI score, duration of psoriasis, arthropathy, metabolic syndrome. Outcome variables considered in different analyses, were: alterations of EAC, alterations of tympanic membrane, hypoacusis, tympanogram, PASI score, DLQI. To evaluate differences between groups, we used Student’s t-test for quantitative data with normal distribution, or Mann–Whitney U test for quantitative data without normal distribution. For qualitative data, frequencies were compared using the χ2 test. To evaluate the relative importance of each risk factor in the development of hypoacusis, we performed multivariate logistic regression analysis considering the presence of hypoacusis as dichotomic dependent variable, and sex, age, BMI, presence of diabetes and presence of metabolic syndrome as independent variables. In all analyses, p < 0.05 was considered significant.
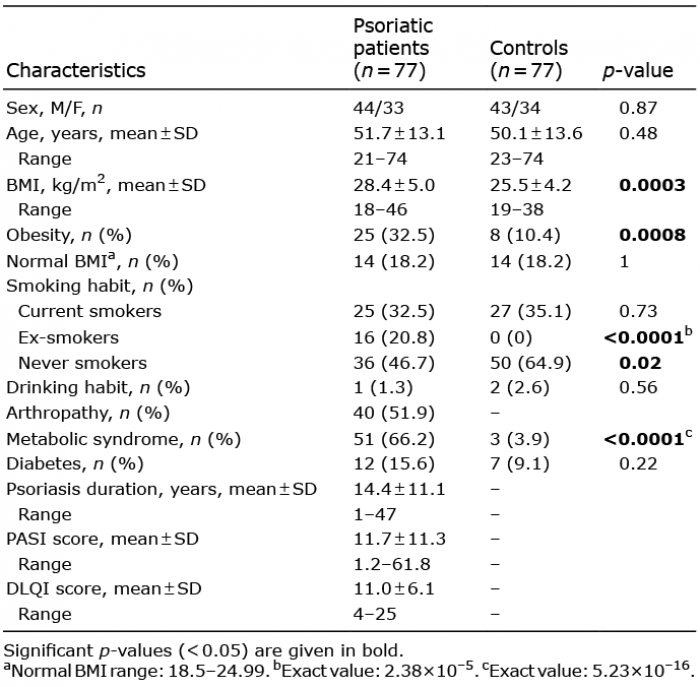
Sociodemographic characteristics of the 77 psoriatic patients and 77 controls enrolled in the study are shown in Table I. Clinical features and hearing function of each ear were studied separately according to similar studies on auditory system involvement in other metabolic disorders (14, 15). Dermatological examination of the EAC revealed mild alterations in 26% of psoriatic patients vs. 33.1% of controls, while moderate or severe involvement were observed only in patients (45.5% and 3.9% of cases, respectively). Alterations in the tympanic membrane were mild in 41.6% of patients and 48.1% of controls, moderate in 24.7% of patients and 8.4 % of controls, and severe only in psoriatic subjects (3.9%). No signs of serous otitis media were detected during otomicrosopic examination. The above differences between patients and controls were significant (p < 0.0001 for EAC alterations, p < 0.005 for alterations of the tympanic membrane).
Table I. Sociodemographic characteristics of psoriatic patients and controls
The results of hearing assessment are summarized in Table II. Hearing loss, assessed using age- and sex-independent criteria, was detected in 81/154 ears (52.6%) of psoriatic patients and 23/154 ears (14.9%) of controls (p < 0.0001). Patients had sensorineural type hearing loss in 57 ears, conductive hearing loss in 9, and mixed-type hearing loss in the remaining 15 ears. Among controls, hearing loss was found in 23 ears (14.9%), of which 21 had sensorineural hearing loss and 2 mixed-type hearing loss. The difference between patients and controls was significant only for sensorineural hearing loss (p = 0.04).
Table II. Results of audiometric evaluation
Among patients, type A tympanogram with normal compliance was observed in 99 ears (64.3%), while type AD, B or C tympanograms, which indicate middle ear dysfunc-tion, were recorded in 45 (29.2%), 3 (1.9%) or 7 (4.5%), respectively. In the control group, tympanograms were of type A in 140 ears (90.9%) and type A1 in 14 (9.1%).
Moderate to severe alterations in the EAC were significantly associated with psoriatic arthropathy (p = 0.037) and metabolic syndrome (p = 0.023). Higher degrees of alteration were significantly more frequent in patients with longer duration of psoriasis (p = 0.0078). Subjects (patients+controls) with normal BMI showed only mild (46.4%), moderate (39.3%) or no EAC alterations (14.3%), whereas higher BMI levels (overweight/obesity) were significantly (p = 0.043) associated with a corresponding increase in subjects (psoriatic or not) with moderate-to-severe EAC involvement. The mean ± SD PASI score of patients with severe EAC alterations was 21.1 ± 9.9, significantly higher than that of patients with no (8.6 ± 6.2, p = 0.0056) or mild EAC alterations (7.8 ± 6.1, p = 0.002). Significant (p = 0.018) differences also existed between the mean PASI score of patients with mild or moderate EAC alterations (14.6 ± 14.1). Severity of tympanic membrane alterations significantly increased with age, much more in patients than in sex- and age-matched controls (p < 0.0001), and with disease duration (p = 0.002). In the entire population (patients+controls), smoking habit and metabolic syndrome were also associated with significantly worse conditions of tympanic membrane (p = 0.021 and 0.045, respectively). The frequency of hearing loss, mostly of sensorineural type, increased with age in psoriatic patients much more than in healthy controls (p < 0.0001); some patients had conductive hearing loss, which was not present among controls. Conductive and mixed hearing loss were significantly (p = 0.006) more frequent in patients with psoriatic artropathy than in patients without psoriatic arthropathy. Psoriatic patients with disease duration > 10 years showed significantly (p < 0.0001) higher frequency of hearing loss, mainly of conductive and mixed type; smoking was also associated with hearing loss (p < 0.0001), with mild improvements in ex-smokers. Psoriasis was more severe in patients with hearing loss than in those without hearing loss, as suggested by PASI score (13.6 ± 12.7 vs. 9.5 ± 9.1, p = 0.025) and DLQI (12.2 ± 6.5 vs. 9.7 ± 5.4, p = 0.012). Last but not least, significant differences in the relative proportions of tympanogram types were observed in correlation with psoriasis duration: the frequency of type AD tympanogram was higher in patients whose cutaneous disease had lasted more than 20 years.
The results for overall goodness-of-fit of the model were: R2 = 0.173, χ2 = 34.355, p < 0.00001. The only predictors with a significant p-value were age (coefficient = 0.041, p = 0.009) and, with definitely higher impact, presence of psoriasis (coefficient = 2.166, p < 0.0001). p-values for sex, BMI, presence of diabetes and presence of metabolic syndrome were 0.128, 0.713, 0.856 and 0.330, respectively.
These data reveal an increased frequency of morphofunctional alterations in the auditory system in psoriatic patients. Otomicroscopic findings show more alterations of the EAC and tympanic membrane in psoriatic patients than in controls, with positive correlation between severity of otological involvement and duration of psoriasis or PASI score. Mean PASI of patients with severe EAC lesions was significantly higher than in patients with mild EAC involvement. Mean PASI of those with moderate EAC alterations was also significantly higher than that of patients with mild EAC alterations. Auricle and the external third of EAC mainly contain elastic cartilage covered with skin and appendages, including hair cells and sebaceous (lipid-producing) and apocrine (ceruminous) glands (8, 16). Sebumetry shows significantly higher values in non-lesional forearm skin and plaques of psoriatic patients vs. corresponding areas of controls (17). Cutaneous chronic inflammation and keratinocyte hyperproliferation cause progressive skin thickening, with tendency to substenosis and cerumen accumulation in the EAC, and stenosis of the tympanic membrane. This pathogenic mechanism is similar to that of keratosis obturans (18), but in a less severe form. The above processes cause impairment of sound transmission to the middle ear. In addition, BMI and metabolic syndrome were also correlated with the severity of ear involvement. It is known that BMI correlates with hearing loss at all frequency ranges, with a higher BMI associated with more severe hypoacusis (19, 20). In the current study population, an increase in BMI towards values suggesting overweight or obesity was associated with significant progressive reduction in the number of patients with mild alterations and corresponding increase in those with moderate and severe alterations of the tympanic membrane. The significant association between moderate to severe otomicroscopic findings and psoriatic arthropathy appears difficult to explain. Comparison of audiometric tests between groups revealed more pronounced hypoacusis in psoriatic patients than in controls, with a clear prevalence of sensorineural hearing loss. Hearing loss can be categorized as conductive, sensorineural, or mixed (21). Sensorineural hearing loss (SNHL) is caused by damage to the inner ear (cochlea) or to the nerve pathway from the inner ear to the brain. This is the most common type of permanent hearing loss; main causes include inherited disorders, noise exposure, and age-related presbycusis (decrease in hearing acuteness resulting from degenerative changes in the ear that occur particularly in old age). In our study, SNHL increased in psoriatic patients proportionally to age, at a higher rate than observed in age- and sex-matched healthy subjects. This can be interpreted as an expression of more precocious ageing of the auditory system, probably linked to metabolic syndrome. Indeed, there is a well-known correlation between vascular risk factors and auditory symptoms (hypoacusia, tinnitus, dizziness), with a role of impaired cochleo-vestibular microcirculation in the premature and irreversible deterioration of auditory and vestibular function. Data from the current study show a clear trend towards statistical significance (p = 0.07), in agreement with literature data (22, 23). Duration of psoriasis > 10 years represents an additional risk factor for SNHL. Conductive hearing loss is caused by outer-ear, tympanic membrane, or middle-ear abnormalities involving the chain of the ossicles (20). The main causes of conductive hearing loss include cerumen impaction, otitis media, and otosclerosis. Its increased frequency in the psoriasis group, although inconstant and not age-related, is probably multifactorial. It may be secondary to the alterations in psoriatic skin of the EAC and tympanic membrane, which impair transmission of acoustic waves. Moreover, the higher frequency of both conductive and mixed hypoacusis among subjects with psoriatic arthropathy could suggest that arthropathic impairment of the chain of the ossicles might cause or worsen the conductive defect. Tympanometry was also worse in psoriatic patients than in healthy controls. Tympanometry, or measurement of the acoustic impedance of the ear, gives information about the state of the middle ear, providing a graphic representation of the relationship of air pressure in the external ear canal with impedance (resistance to movement) of the ear-drum and middle ear system. A normal tympanogram is designated type A; pathologic subcategories are indicated as AD, AS, B, C, D, E (24). In our study population, a significant correlation was observed between psoriasis duration and distribution of the different types of tympanogram. In particular, patients affected by psoriasis for more than 20 years showed increased frequency of type AD tympanogram, commonly found in cases of flaccid tympanic membrane or ossicular discontinuity (abnormal separation of the middle ear bones). In such cases, it is likely that the stiffening of the tympanic-ossicular complex (tympanic membrane alterations and/or arthropathic impairment of the chain of the ossicles) may reduce the elasticity of the system, thus inducing lower compliance.
This study has some limitations. First, although hearing loss and psoriasis appear to be clearly associated, changes in hearing levels were not evaluated at different time-points. Therefore, additional longitudinal studies are needed to identify the possible causal role of psoriasis. Secondly, the mechanism(s) that link psoriasis and hearing loss were not analysed, and further research in this field appears necessary, as well as for the possible clinical and therapeutic implications. Thirdly, the “relative weight” of psoriasis in the pathogenesis of hypoacusis is difficult to evaluate, because of the rather high percentage of patients with metabolic syndrome. High values of BMI can also be linked to hearing loss. Indeed, high BMI is a cardiovascular risk factor, and the association between cardiovascular risk and impaired microcirculation of the internal ear is known. Also known is the association between impaired microcirculation of the internal ear and hearing loss (25). Analysis of our results with multivariate logistic regression supports the idea of a direct link between psoriasis and hypoacusis, independent of other known factors, although a larger sample of patients and controls is required to improve the precision and reliability of the multivariate model.
These data confirm and reinforce the idea of psoriasis as a multisystemic disease, and further expand the scope of clinical research in this field by showing that ear involvement is frequent in psoriatic patients, and does not concern only the external ear. The clear association between psoriasis and hearing loss supports the need for further studies, aimed at better defining the underlying pathogenic mechanism(s) and updating diagnostic, and perhaps therapeutic, protocols accordingly. In this context, the role of dermatologists includes not only diagnosing and treating the cutaneous manifestations of psoriasis, but also searching for extracutaneous manifestations of the disease and coordination of the various specialists in a dedicated multidisciplinary team involved in this task.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize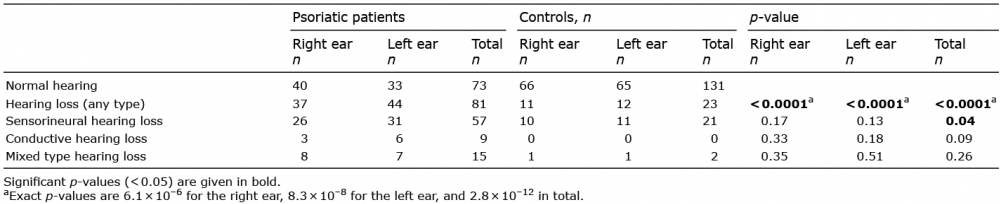 Click to show fullsize
Click to show fullsize