


Departments of 1Dermatology, Venereology and Allergology, and 2Internal Medicine II, University Hospital Würzburg, Würzburg, Germany
Oesophageal involvement in mucous membrane pemphigoid is considered rare, but it may be underdiagnosed. To assess the incidence of oesophageal involvement in a group of patients with newly diagnosed mucous membrane pemphigoid we retrospectively analysed the medical records of 30 consecutive patients with mucous membrane pemphigoid diagnosed between 2006 and 2016 at the Department of Dermatology, University Hospital Würzburg. Twenty-one patients (70%) reported symptoms indicative of oeso-phageal mucous membrane pemphigoid. Twelve patients (40%) underwent oesophagogastroduodenoscopy, and oesophageal pathology compatible with mucous membrane pemphigoid was endoscopically found in 9 cases (30%). In all patients indirect and direct immunofluorescence were performed. Patients with and without oesophageal involvement did not differ with regard to the results of indirect immunofluorescence on salt-split human skin and monkey oeso-phagus. Study results demonstrate the necessity of a standardized diagnostic work-up, including adequate tissue samples for direct immunofluorescence, to prevent underdiagnosis of oesophageal mucous membrane pemphigoid.
Mucous membrane pemphigoid (MMP) is a rare chronic autoimmune disease of the skin and mucous membranes. Oesophageal involvement is a potentially under-diagnosed “high-risk” complication necessitating intensive immuno-suppressive treatment. In our current study we analysed the medical records and diagnostic findings of 30 patients with MMP. We found that a thorough diagnostic work-up is required for early detection of oesophageal involvement. Patients with newly diagnosed MMP complaining of a loss of weight or difficulty in swallowing need to undergo oesophagoscopy including biopsies for direct immunofluorescence.
Key words: cicatricial pemphigoid; mucous membrane pemphigoid; oesophagogastroduodenoscopy; laminin 332.
Accepted Apr 12, 2018; Epub ahead of print Apr 12, 2018
Acta Derm Venereol 2018; XX: XX–XX.
Corr: Sandrine Benoit, Department of Dermatology, Venereology and Allergology, University Hospital Würzburg, Josef-Schneider-Str. 2, DE-97080 Würzburg, Germany. E-mail: benoit_s@ukw.de
Mucous membrane pemphigoid (MMP) is a heterogeneous group of subepidermal blistering autoimmune diseases that may affect all mucous membranes and the skin. The clinical presentation of MMP varies depending on the distribution and severity of the disease. This includes a wide spectrum of symptoms ranging from almost asymptomatic erosions to severe cicatrisation, which may result in blindness and/or severe stenosis of the urinary tract or the oesophagus (1). Oral and ocular mucous membranes are most frequently involved (2–4). Oesophageal involvement is generally considered to be relatively rare (4–11%) (2–5), but there is a lack of studies assessing its actual incidence. Oesophageal symptoms may sometimes represent the sole manifestation of MMP (6–9). Dysphagia, odynophagia, pain in the oral cavity or throat, weight loss, and/or inability to ingest solid food have been described as indicative of MMP with oesophageal affection (5). Similar symptoms, however, can also be caused by pharyngeal involvement or affection of the oral cavity. Apart from recommendations from an international consensus group published in 2002, no evidence-based guidelines for the diagnosis and treatment of MMP are available to date (10). As patients present to different specialists (i.e. ophthalmologists, dermatologists, gastroenterologists, otolaryngologists, urologists, and/or gynaecologists) depending on their symptoms, establishing an accurate diagnosis and the full extent of the disease may be challenging. Rare manifestations, including oesophageal involvement, are likely to remain underdiagnosed due to an incomplete diagnostic work-up at initial diagnosis and during the further course of the disease.
The purpose of this retrospective study was to assess the incidence of oesophageal involvement in a group of patients with newly diagnosed MMP and to evaluate clinical findings and autoimmunological profiles associated with oesophageal manifestations of MMP.
Medical records of 30 consecutive patients were available for retrospective evaluation. Individual cases were eligible for study inclusion if they had a definite diagnosis of MMP and were treated between January 2006 and August 2016 at our department, a tertiary university hospital-based referral centre. All patient-related diagnostic and therapeutic procedures were part of routine practice. Written informed consent was obtained for oesophagogastroduodenoscopy (EGD) and biopsies.
Data on the patients’ background and clinical history (age, sex, signs and symptoms, time of onset, time of diagnosis) as well as information on histopathological and immunological results were retrospectively retrieved from the medical records. The retrospective evaluation of data was approved by the ethics committee of the Medical Faculty of the University of Würzburg (approval number 5/14).
MMP was diagnosed considering: (i) clinical findings; (ii) indirect immunofluorescence microscopy (IIF); (iii) identification of target antigens; (iv) direct immunofluorescence (DIF); and (v) histopathological examination of biopsies taken from the skin, conjunctiva, and/or oral mucosa. A diagnosis of MMP was made if clinical findings were compatible and either DIF and/or IIF were positive and/or the target antigen was identified. Oesophageal involvement was diagnosed by EGD. Dysphagia represented the main indication for endoscopy.
A thorough clinical history was taken following a standardized questionnaire. The affected anatomical regions were documented (i.e. ocular, nasal, pharyngeal, laryngeal, oesophageal, anal and/or genital mucous membranes, and/or the skin).
IIF is a well-established method to detect circulating autoantibodies in the serum (11). Salt-split human skin and monkey oesophagus were used as substrates to detect immunoglobulin (Ig)G and/or IgA antibodies targeting components of the dermoepidermal junction. Human skin was split at the level of the lamina lucida using 1 M saline solution, thereby permitting the differentiation of dermal and/or epidermal antibody binding. Binding antibodies were visualized by incubation with fluorescein isothiocyanate (FITC)-conjugated sheep anti-human antibodies targeting IgG or IgA. IIF was followed by enzyme-linked immunosorbent assay (ELISA) and immunoblotting to identify targeted antigens.
IgG antibodies binding to the bullous pemphigoid antigens BP180 or BP230 were detected by ELISA (MESACUP BP180®, MBL, Nagoya, Japan; anti-BP230-CF-ELISA®, Euroimmun AG, Lübeck, Germany) following the manufacturers’ instructions. Immunoblots were performed to detect circulating IgG or IgA antibodies binding to the soluble 120-kDa ectodomain of BP180 (LAD-1), the BP180 C-terminal segment 4575, BP230, laminin 332, and/or type VII collagen, as described elsewhere (12–14).
To detect tissue-bound autoantibodies, biopsies for DIF were taken from perilesional skin and/or mucosa (that is within a 1-cm radius of erosions or blisters) and subsequently stored in either isotonic saline or Michel’s medium for a maximum of 72 h or promptly transferred into liquid nitrogen (11). DIF was performed according to a standardized protocol. In brief, 6 µm-thick cryocut tissue sections were obtained. At least 12 sections of every biopsy were stained with FITC-conjugated sheep anti-human antibodies targeting IgG, IgA, IgM or C3 and examined by fluorescence microscopy. Linear deposits of IgG, IgA and/or C3 at the dermo-epidermal junction were considered diagnostic of MMP.
Biopsies for histopathological examination were taken from lesional skin or mucosa, stored in formalin solution, and stained with haematoxylin and eosin following a standardized protocol.
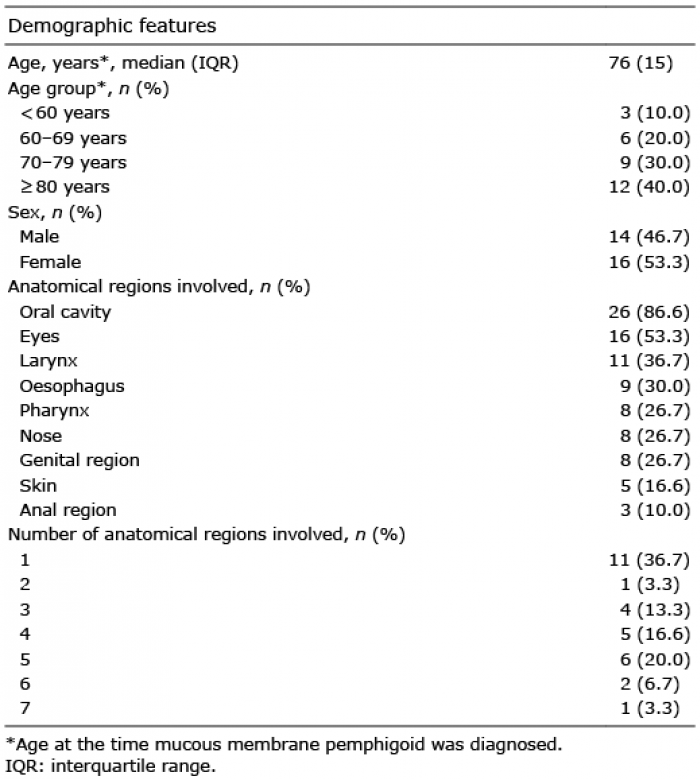
Clinical data for the patient cohort is shown in Table I. A total of 30 patients (16 women, 14 men) were diagnosed with MMP between January 2006 and August 2016. The median age at the time first symptoms occurred was 74 years (interquartile range (IQR) 16 years), the median age at the time MMP was diagnosed was 76 years (IQR 15 years). The median time interval between the onset of symptoms and diagnosis of MMP was 12 months (IQR 6 months). The median observation period following the diagnosis of MMP was 17 months (IQR 52 months).
Table I. Demographic and clinical features (30 patients)
Oral mucous membranes were affected most frequently (n = 26; 86.6%), followed by involvement of the eyes in 16 patients (53.3%). Laryngeal mucous membranes were involved in 11 patients (36.7%), oesophageal involvement was diagnosed by EGD in 9 cases (30.0%). Eight patients (26.7%) had pharyngeal, nasal or genital affection, respectively. Involvement of the skin (n = 5; 16.6%) and the anal region (n = 3; 10.0%) was relatively uncommon. In 11 (36.7%) patients, only 1 anatomical region was affected. Those patients showed either involvement of the oral cavity (n = 7) or of the eyes (n = 4).
There was a tendency towards a greater burden of disease in the 9 patients with oesophageal MMP who showed a median involvement of 5 anatomical regions (range 3–7, IQR 1) compared with the group without oesophageal involvement showing a median affection of 1 region (range 1–6, IQR 3).
Table II provides individual information on the patients included. Thirteen patients reported dysphagia (43.3%), 9 reported oral pain (30.0%). One patient (3.3%) had both dysphagia and oral pain, and one patient (3.3%) was incapable of specifying symptoms due to mental impairment. Most patients (n = 24, 80.0%) were unable to provide reliable information concerning a recent change of weight. Only 2 patients reported weight loss. Both also had dysphagia, and oesophageal affection was endoscopically confirmed in both cases.
Table II. Symptoms and clinical findings suggestive of oesophageal involvement
In total, 12 patients (40.0%) underwent EGD, 9 of them reporting dysphagia. Nine patients (75.0%) had endoscopic findings compatible with MMP. In all but one patient (n = 8; 88.9%) with MMP and dysphagia undergoing EGD, pathological changes of the oesophagus were observed. These comprised desquamation of superficial epithelial layer spontaneously or on manipulation (n = 5), erosions (n = 1), ulcers (n = 2), erythema or oesophagitis (n = 5) and cicatrization or stenosis (n = 5) (Table II). In one patient reduced peristalsis and in another patient bleeding was observed, respectively. In 2 patients whitish plaques were found. One of these patients (#28, Table II) did not report dysphagia.
Notably, the pathological findings were more prominent in the upper half of the oesophagus in most patients.
In less severe cases, non-specific endoscopic changes were observed, such as reduced peristalsis or whitish plaques. In these patients, other differential diagnoses, such as eosinophilic oesophagitis, were considered, but excluded by biopsy. Cicatrization, ulcers and/or stenosis were found in severe affection of the oesophagus. A specific sign of oesophageal involvement by MMP was desquamation of the superficial layer of the mucosa (Fig. 1), induced either by passage of the endoscope or by biopsy. This phenomenon was observed in 5 of the patients in whom EGD was performed.
Fig. 1. Oesophageal involvement in a patient with mucous membrane pemphigoid with desquamation of the superficial layer of the mucosa during oesophagogastroduodenoscopy.
Since the presence of dysphagia was the main indication for EGD, endoscopy was performed in only 3 patients without dysphagia. In one of these cases (#28, Table II), whitish plaques covering the oesophageal mucosa as possible manifestation of MMP were seen.
In most patients with oesophageal MMP (n = 6; 66.7%), EGD at the time of the initial diagnosis permitted early detection of the oesophageal involvement. In 3 patients (#1, 7 and 28) oesophageal involvement occurred in the later course of the disease, that is 12, 46 and 4 months after the initial diagnosis. The median time interval between the first onset of symptoms of MMP and the diagnosis of oesophageal involvement was 14 months (IQR 27 months).
An overview on immunological findings in all patients is given in Table III.
Table III. Immunological findings in all patients with mucous membrane pemphigoid (n=30) and in patients with oesophageal involvement (n=9)
One or several (up to 7) perilesional biopsies for DIF were taken in every patient. In total, 63 biopsies were analysed: 40 from oral, 10 from conjunctival, 6 from oesophageal, and 2 from genital mucosa, as well as 5 biopsies from the skin. Linear deposits of IgG, IgA and/or C3 along the basal membrane zone were detected in 32 biopsies (50.8%) of 22 patients (73.3%). Biopsies for histopathological examination from different localizations were available in 25 patients (83.3%). Histo-pathology was suggestive for MMP in 18 cases (72.0%). In the remaining 7 patients (28.0%), no specific pattern was detected.
Patients with and without oesophageal involvement did not differ with regard to the results of the initial DIF and histopathology. Oesophageal biopsies were avail-able in 10 patients. Histopathological examinations were invariably non-specific and did not permit diagnosis of oesophageal involvement. Oesophageal tissue samples for DIF were available in 3 patients. Linear deposits of IgG, IgA and C3 along the basal membrane zone were detected in one case.
IIF on salt-split human skin and monkey oesophagus was performed in all 30 patients. In total, 16 patients (53.3%) were positive for IgG and/or IgA antibodies on human split skin. Circulating IgG autoantibodies binding to the basal membrane zone were detected in 9 sera (30.0%). In 8 cases, IgG antibodies were found to bind to the roof of the artificial blister, in one case to the bottom. Circulating IgA autoantibodies binding to the epidermal side of the artificial blister were detected in 11 sera (36.7%). Four sera (13.3%) were found to be positive for both circulating IgG and IgA antibodies to human split skin. Circulating IgG or IgA antibodies binding to the basal membrane were detected on monkey oesophagus in 5 sera (16.7%). In 13 patients (43.3%) circulating antibodies binding to the basal membrane could be detected on neither human split skin nor monkey oesophagus, but at least one target epitope was identified by immunoblot or ELISA. Patients with and without oesophageal involvement did not differ with regard to the results of IIF.
Immunoblots assessing circulating IgG and IgA antibodies binding to LAD-1, the soluble 120-kDa bullous pemphigoid 180 (BP180) ectodomain, or to the C-terminal fragment 4575 of BP180 were performed in all 30 patients. ELISA testing for circulating IgG antibodies binding to BP180 or BP230 was performed in 25 (83.3%) and 22 (73.3%) patients, respectively. Circulating IgG autoantibodies binding to laminin 332 were assessed by immunoblot in 23 cases (76.7%), and autoantibodies to type VII collagen in 3 (10.0%) cases. Comparative statistical analysis of target antigen patterns in patients with and without oesophageal involvement was not possible due to the limited number of cases. Study data, however, indicate that circulating IgG antibodies targeting BP180, LAD-1, and particularly laminin 332, might be more prevalent in concurrent oesophageal disease.
MMP, formerly referred to as “cicatricial pemphigoid”, is a rare and heterogeneous group of chronic blistering diseases affecting the mucous membranes. Its overall incidence has been estimated to range between 1 in 12,000 and 1 in 20,000 in the general population (2); however, reliable epidemiological data are limited. In accordance with our own findings, oral and ocular involvement have been described as the most frequent manifestations of the disease (3, 4, 10, 15). The risk of serious sequelae due to cicatrization mainly depends on the anatomical regions affected. Therefore, a differentiation of “low-risk” and “high-risk” cases has been proposed, and more intensive immunosuppressive treatment is recommended for “high-risk” patients (10). Interestingly, our study data suggest a higher burden of disease in patients with oesophageal affection who showed a greater median number of affected anatomical regions compared with the group without oesophageal affection. Oesophageal involvement might thus be considered a general indicator of MMP severity.
Oesophageal involvement is a potential cause of severe stenosis and has therefore been classified as a “high-risk” manifestation (10). In the available literature, MMP affecting the oesophagus is considered to be relatively rare (4–11%) (2–5). In our present series, a significantly higher incidence (30%) was confirmed by oesophagoscopy. Only 40% of our patients, however, underwent endoscopy, which suggests that oesophageal involvement may still have been underdiagnosed. Further studies assessing oesophagoscopic findings in a larger number of patients are required to accurately define the incidence of oesophageal MMP.
This series of patients allows us to define some endoscopic features typical for oesophageal MMP. These comprise:
A thorough clinical history with a focus on clinical symptoms suggestive of oesophageal MMP was ascertained in all patients. In particular, we suggest that dysphagia is a predictor of oesophageal manifestations of MMP. All but one patients with dysphagia, in whom an EGD was performed, showed pathological findings compatible with MMP. Since for another 5 patients with dysphagia an EGD was not available, the incidence of oesophageal manifestations in MMP may be even higher than suggested by our confirmed cases.
Some patients, however, were not able to distinguish oral pain from dysphagia and/or odynophagia, and most patients were incapable of providing reliable information about recent changes in weight. Moreover, the above-mentioned symptoms are not specific, as they may also result from oral and/or pharyngeal MMP. The inability to ingest solid food as the most severe manifestation of dysphagia, though a more specific indicator of oesophageal MMP, appears only at an advanced stage of the disease. As a consequence, we suggest that EGD should be performed in all patients with a new diagnosis of MMP who have oral or pharyngeal erosions, and is mandatory in the case of dysphagia, odynophagia, weight loss and/or inability to ingest solid food. If symptoms remain confined to the eyes or anogenital region, EGD may be dispensable.
These study data suggest that oesophageal involvement occurs relatively early in the course of MMP, as it was commonly detected at the time of the initial diagnosis. Nevertheless, as oesophageal involvement may also occur during the further course of the disease, it is necessary to re-evaluate the need for an EGD on a regular basis. Once a diagnosis of oesophageal MMP is confirmed, repeated endoscopic examinations may be required. There is, however, no general consensus on how often EGDs should be performed during follow-up. If symptoms resolve and affections of other mucous membranes improve, follow-up examinations may be dispensable. Moreover, repeated EGDs are not without risk (16). Some of our patients experienced an aggravation of symptoms following EGD, and one patient died from oesophageal rupture following endoscopic dilatation. In the end, follow-up examinations need to be planned on an individual basis considering the progression and/or complications (e.g. stenosis) of the disease and the impact on further therapeutic strategies.
In our series oesophageal involvement was clinically diagnosed by EGD. This approach was considered appropriate as all patients had a definite diagnosis of MMP involving at least one other anatomical site apart from the oesophagus. Endoscopic findings compatible with MMP (e.g. ulcerations, erythema, cicatrization and/or strictures), however, are relatively non-specific and do not permit a definite diagnosis of MMP in patients with oesophageal manifestations as the only symptom. Samples for histopathological examination were available in 10 out of 12 patients, but the results were likewise non-specific. This is in accordance with the medical literature stating that histopathology is not suitable to confirm an autoimmune blistering disease, but may be useful to exclude differential diagnoses (11). By contrast, detection of linear deposits of IgG, IgA and/or C3 along the basal membrane zone by DIF allows for the diagnosis of MMP in patients presenting typical clinical symptoms. The sensitivity of this method has been reported to vary from 50% to 80%, depending on the technique (4, 17, 18). Other than in histopathological examination, a perilesional biopsy is required for DIF (see Methods section), and storage in formalin solution leads to a destruction of binding antibodies (11). Therefore, separate samples are needed for histology and DIF. In our series, adequate oesophageal tissue samples for DIF were available in only 3 out of 12 patients. This might be due to the fact that either MMP was not considered at the time of EGD, that the diagnosis MMP was already confirmed by DIF of another anatomical site at the time of EGD, or that the endoscopists in charge were not aware of the importance of DIF and/or the above-mentioned requirements.
IIF on salt-split human skin and monkey oesophagus is an integral part of routine diagnostic work-up in suspected MMP (18). A dual antibody response with both IgG and IgA antibodies has been associated with a more severe and persistent course of the disease (19, 20). Circulating autoantibodies, however, cannot be detected by standard IIF in up to 50% of cases (2, 21). Accordingly, IIF was negative in 43.3% of our patients. Additional ELISA testing and immunoblotting is recommended for the detection of IgG and/or IgA autoantibodies binding to specific target antigens (i.e. different domains of BP180, BP230, laminin 332, α6β4-integrin, and type VII collagen) (4, 18). A correlation between target antigen patterns and the patients’ prognosis has been postulated, and the detection of IgG antibodies binding to laminin 332 has been described to coincide with an increased risk of concurrent malignancy (22, 23). In addition, it was shown that anti-laminin 332 IgG antibodies are associated with pharyngo-laryngeal and oro-pharyngo-laryngeal involvement (23, 24). Interestingly, our study data suggest a higher rate of anti-laminin 332 IgG antibodies among patients with oesophageal MMP. Larger and prospective studies are required in order to determine whether detection of antibodies binding to laminin 332 is predictive of oesophageal involvement.
This study indicates that oesophageal involvement is an underdiagnosed “high-risk” complication of MMP requiring intensive immunosuppressive treatment. Based on our data, we recommend performing EGD in all patients with a new diagnosis of MMP who have oral or pharyngeal erosions. In addition, EGD should be conducted in the case of dysphagia, odynophagia, weight loss and/or inability to eat solid food to enable early detection of oesophageal affection in MMP. Oesophageal biopsies for DIF are required to permit a definite diagnosis of MMP with oesophageal involvement, especially if oesophageal symptoms represent the sole manifestation of MMP.
This publication was funded by the German Research Foundation (DFG) and the University of Wuerzburg in the funding programme Open Access Publishing.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize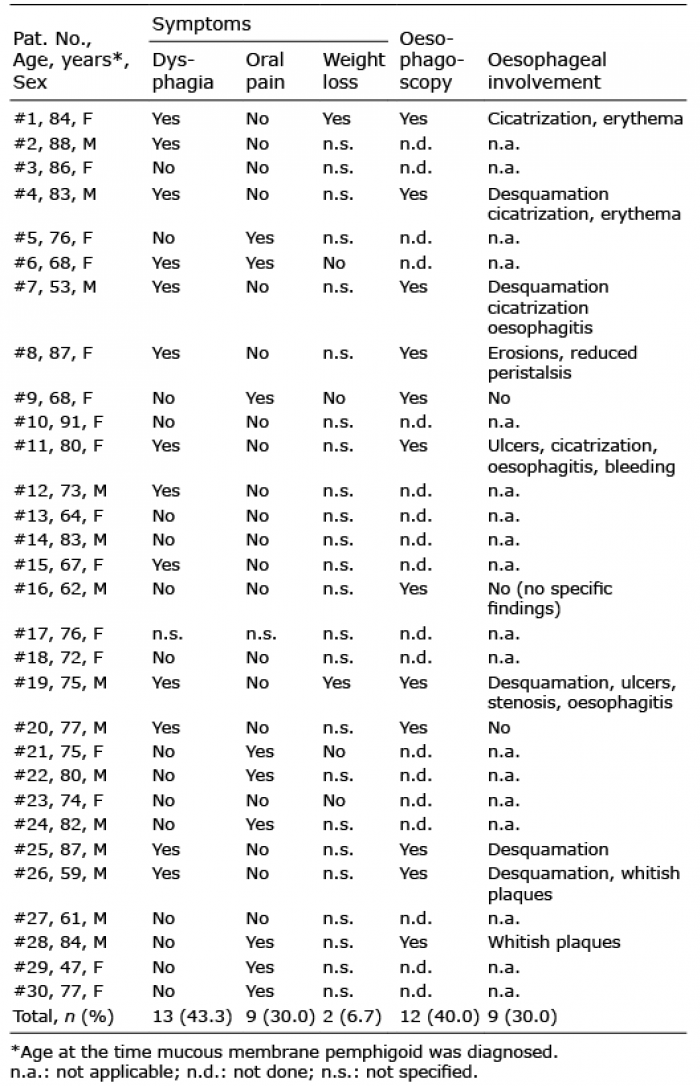 Click to show fullsize
Click to show fullsize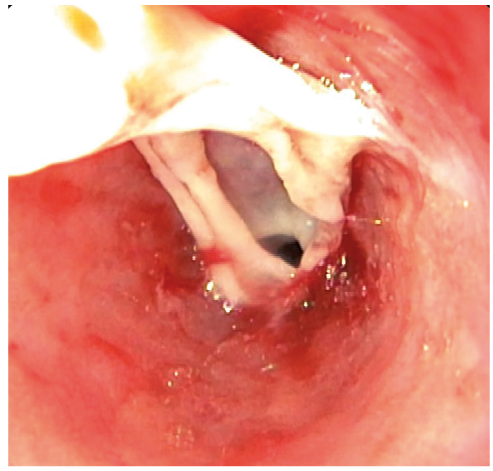 Click to show fullsize
Click to show fullsize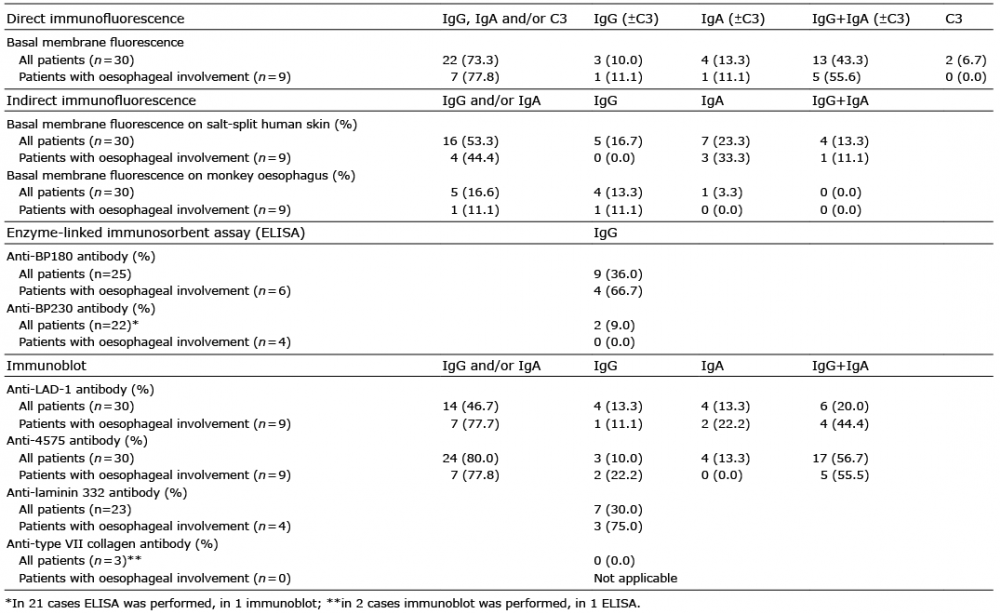 Click to show fullsize
Click to show fullsize