


1Department of Dermatology, University Hospital of Brest, FR-29609 Brest, 2Laboratory Interactions Neurons-Keratinocytes (LINK), University of Western Brittany, Brest, 3Deparment of Dermatology, University Hospital of Bordeaux, Bordeaux, 4Courlancy Polyclinic, Reims, 5Association Française de l’Eczéma, Redon, 6EA4636, University of Rennes 2, Rennes, 7European Market Maintenance Assessment, Vincennes, 8EA EpiDermE, University Paris-Est, Paris, 9Department of Dermatology, University Hospital Henri Mondor, Créteil, France. E-mail: laurent.misery@chu-brest.fr
Accepted Apr 12, 2018; Epub ahead of print Apr 12, 2018
Atopic dermatitis (AD) profoundly alters quality of life in adults. There are few studies concerning patient burden in AD (1), since burden of disease is a recent concept that includes broader aspects of disease-related disability (2), such as psychological, physical, social, and economic factors (2–4). It is possible that the burden of skin diseases may be as great as that of other chronic diseases (5).
This study (Eczema Cohorte Longitudinale Adultes; ECLA) assessed the burden of AD using the Atopy Burden Score – Adult (ABS-A), a recently developed specific tool, and compared the results with those obtained with 3 different quality of life scales.
Patients with AD were members of the French Association of Eczema (Association Française de l’Eczéma) or outpatients recruited in 4 dermatology centres in France (Brest–Bordeaux–Créteil–Reims).
The patients answered questions on their socio-demographic data, disease history and management data; location of lesions; impact on sexuality, partners and family, and professional life; and the financial cost of the disease. Disease severity was evaluated using the Patient-Oriented SCORing Atopic Dermatitis (PO-SCORAD) index. In addition, patients were asked to complete 3 generic quality of life questionnaires (Short Form-12 (SF-12), Dermatology Quality of Life Index (DLQI) and Euro-QoL-5 Dimensions (EQ-5D)) and an AD-specific burden questionnaire, the ABS-A.
The PO-SCORAD index has a self-assessment score of AD (6). Although the PO-SCORAD is not recommended to assess clinical signs of AD, it is convenient to define the following large classes of severity: mild (PO-SCORAD score < 25), moderate (between 25 and 50) and severe (> 50).
The SF-12 is a short version of the Short Form-36 (SF-36), a generic measure enabling assessment of health status in the general population (7). Two scores, the Physical Component Summary (PCS-12) and the Mental Component Summary (MCS-12), can be calculated from the 12 questions of the SF-12. There is no overall score. A higher score indicates a better quality of life (8).
The DLQI is a health quality of life scale specific to dermatological disorders (9). A total score (between 0 and 30) is calculated and can be expressed as a percentage. A higher score indicates a worse quality of life.
The EQ-5D has 5 dimensions (Mobility, Self-care, Usual activities, Pain/Discomfort, Anxiety/Depression) (10). At the end of the questionnaire, a visual analogue scale (EuroQoL-visual analogic scale; EQ-VAS) records the respondent’s self-rated health on a 20-cm vertical scale (score range 0–100).
The ABS-A is an 18-item questionnaire specifically developed to evaluate the burden of AD in daily life (11). Each of the 18 items is rated with a 7-level scoring system and evaluates specific aspects of the burden of AD during the past 7 days. A higher score indicates a higher burden.
Statistical analysis was performed using Student’s t-test, analysis of variance (ANOVA) or non-parametric tests (Wilcoxon or Kruskal–Wallis) for quantitative variables. For qualitative variables, intergroup comparisons were performed with the χ2 test, or Fisher’s test. The level of significance was set at 5%. Data were analysed using SAS® software version 8.2 (SAS Institute, Inc., Cary, NC, USA).
A total of 1,024 patients (596 women (58.3%) and 427 men; mean ± standard deviation (SD) age: 42.7 ± 15.2 years) answered the questionnaire. Of these patients, 283 (27.6%; 50 ± 13.9 years) had mild AD, 414 (40.4%; 41.1 ± 14.8 years) moderate AD and 327 (31.9%; 38.5 ± 14.6 years) severe AD (p < 0.001). There was no significant difference between the 3 latter groups with respect to body mass index (BMI), economic income, academic level and family situation.
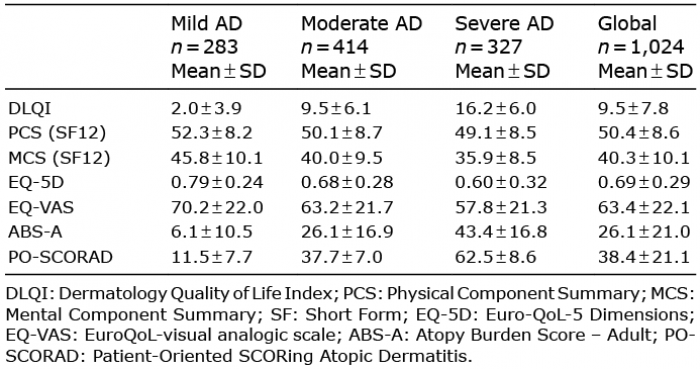
The quality of life and burden scores were higher when disease severity measured with the PO-SCORAD was increased (p < 0.001) (Table I). There were no significant differences between men and women. Changes in quality of life and burden were higher in patients who also presented with asthma (p < 0.001), with the exception of the MCS (p < 0.05), and in patients with hay fever (p < 0.001), with the exception of the EQ-VAS. There were significant positive correlations (p < 0.0001) between the burden assessed with the ABS-A and DLQI (r = 0.84). However, significant correlations between the burden and other quality of life instruments were lower with the generic tools MCS (–0.51), EQ-5D (–0.31) and PCS (–0.24).
Table I. Assessment of burden and alterations in quality of life in patients with atopic dermatitis (AD) with regard to different test scores (p < 0.001)
The patients were also asked questions regarding the consequences of AD on working activity. It was found that 13.7% of patients, including 2.8%, 15.3% and 21.2% in patients with mild, moderate or severe disease, respectively (p < 0.0001) took one or more periods of sick leave due to AD in the previous year. The mean ± SD number of sick leaves (0.1 ± 0.6, 0.3 ± 1.6 and 0.5 ± 1.8 for patients with mild, moderate or severe disease, respectively) and their duration (0.1 ± 0.9, 1.1 ± 3.8 and 6.6 ± 35.7 days for patients with mild, moderate or severe disease, respectively) also differed significantly according to disease severity (p < 0.0001). Similarly, 82.3%, 35.3% and 16.5% of patients, respectively, reported no impact of AD on their place of employment (p < 0.001).
Compared with patients with mild and moderate disease, patients with severe disease showed a significantly higher impact on quality of life and burden (p < 0.0001).
To the best of our knowledge, this study is the first to compare the evaluation of patient burden with the evaluation of quality of life in adult patients with AD, and the first to use both the ABS-A, a new tool for evaluating the burden of AD, and 3 different scales for evaluating quality of life, thus validating the accuracy of the ABS-A. Another interesting aspect is the large number of patients included in this study. Validation of the ABS-A established the good internal consistency and reliability of the questionnaire, and the ABS-A were significantly correlated with both components of the SF-12 and with the DLQI, confirming its concurrent validity (6). The current study confirmed these results in a large number of patients and associated the ABS-A with another scale for evaluating quality of life (EQ-5D), (10), which has rarely been used in dermatology until now (12).
This study confirms that AD in adults has a profoundly negative impact on the lives of affected individuals and their families. The results reveal many effects on patients’ working activity, especially absences from work, including their number and duration. It is notable that many patients think about AD at their places of employment, and these thoughts may have negative effects on productivity, especially in patients with severe AD.
The authors would like to thank SANOFI for their financial support.
Conflicts of interest: LM: Beiersdorf, Bioderma, Expanscience, Galderma, GSK, Johnson&Johnson, Leo Pharma, Novartis, Pierre Fabre, Roche-Posay, Sanofi, Uriage. JS: Sanofi. FH: Beiersdorf. CT is an employee of EMMA. The other authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize