


1Dermatology Department, 2SBIM, 3Pathology Department, 5Department of Nuclear Medicine, 6Oncology Department, 7Oral and Maxillofacial Surgery Department, 8Department of Radiotherapy, Saint Louis Hospital, and 4Paris 7 Diderot University, Paris, France
Cutaneous squamous cell carcinoma (cSSC) is one of the most common skin cancers and can lead to patient death. Early detection of node metastasis is a major goal for dermatologists and oncologists. The procedure sentinel lymph node biopsy has been proposed to improve early detection of node metastasis. The aim of this study was to evaluate the efficacy and impact of this technique on the prognosis of cSSC. A total of 37 patients (Saint Louis Hospital, Paris, France) who had undergone sentinel lymph node biopsy and 290 cases from the literature were analysed. The mean rate of positive sentinel lymph node biopsy was 0.14 [95% CI 0.09–0.22]. However, relapse-free survival and overall survival were not affected by sentinel lymph node status (log-rank test; p = 0.08 and p = 0.31, respectively), suggesting that this procedure is not mandatory in the management of cSSC.
Key words: squamous cell carcinoma; sentinel lymph node; overall survival; relapse-free survival.
Accepted Apr 12, 2018; Epub ahead of print Apr 12, 2018
Acta Derm Venereol 2018; XX: XX–XX.
Corr: Pr Nicole Basset-Seguin, Dermatology Department, Hôpital Saint Louis, APHP, 1 Avenue Claude Vellefaux, FR-75010 Paris, France. E-mail: nicole.basset-seguin@aphp.fr
Early detection of node metastasis is a major goal in oncology. The aim of this study was to evaluate the impact of the sentinel lymph node biopsy (SLNB) procedure on the prognosis of cutaneous squamous cell carcinoma (cSSC). A series of 37 patients and 290 cases from the literature were included. Overall survival and relapse-free survival were not affected by sentinel lymph node status. The presence of a poorly differentiated tumour was the only risk factor associated with a positive SLNB, as well as with relapse. Only one histopathological risk factor, poor differentiation of the tumour, was correlated with positive SLNB results and with recurrence in the case of negative SLNB results.
Sentinel lymph node biopsy (SLNB) is a common procedure for improving initial staging in oncology. In dermatology, SLNB is recommended for the most frequent aggressive cutaneous neoplasms, such as melanoma (1, 2) and Merkel cell carcinoma (3). However, due to lack of evidence, SLNB is not currently recommended by a European consensus for use in cutaneous squamous cell carcinoma (cSCC), which is a frequent and potentially aggressive skin tumour (4). Although mortality in cSCC is lower than in melanoma or Merkel cell carcinoma, cSCC is associated with local recurrence (4.6%), node metastasis (3.7%) and distant metastasis leading to patient death (2.1%) (5). Early diagnosis of nodal metastasis, which is the primary progression route for cSCC, is a major goal for dermatologists and oncologists, in order to optimize the care of these patients. Risk factors (size, thickness and invasion beyond the fat, perineural invasion, poor differentiation, head and neck location, immunosuppression) (4–6) and tumour-node-metastasis (TNM) classifications (7, 8) have been proposed to evaluate tumour prognosis. SLNB efficiency was analysed in a large study (n = 847) of SCC cases in the oral cavity and oropharynx, with positive SLNB results observed in 18–60% of patients with high sensitivity (93%) (9, 10). SLNB was therefore proposed to complete the staging procedure for cSSC. However, the exact impact of SLNBs on cSCC remains unclear and controversial, and the procedure can result in overtreatment and higher morbidity for low-progression patients. The aim of this study was to evaluate the benefits of SLNB and the impact of SLNB results on progression and death in cSCC.
This study combines a mono-centre retrospective series using exhaustive data and pooled analysis with a systematic literature review.
Patients were selected from the cohort of cutaneous cell carcinoma (cSCC) patients treated at the Saint Louis Hospital (Paris, France) between January 2008 and March 2014 and were followed until September 2016. Patients were selected from the Multidisciplinary Tumour Board (MTB) list, in which all patients with cSCC are reported, and cross-referenced with the list of all those who underwent a sentinel lymph node biopsy (SLNB). In our centre, SLNB procedures were offered to patients with unique cSCC TxN0M0 profiles. Main indication of SLNB procedure was patients with T2 (AJCC 7th edition (7)) tumours. For T1 and T3 tumours, staged according to AJCC guidelines (7), the decision to undergo SLNB was made individually after decision of the MTB. If the SLNB showed histological evidence of micro-metastases, radical lymph node dissection (RLND) of the involved basins was recommended.
For each patient, primary tumours were diagnosed histologically using haematoxylin and eosin (H&E) staining. Tumour thickness (mm), differentiation, perineural invasion and diameter (cm) were recorded.
SLNB was carried out according to Morton’s protocol (1). Histopathological examination of each sentinel lymph node was performed after formalin fixation and formalin embedding. Lymph nodes were bisected and examined on 3 H&E-stained (HES) sections cut at 100-µm intervals. One spare section was collected after each HES section, in order to perform AE1AE3 keratin immunohistochemistry (IHC) at least once per lymph node.
For all patients, clinical data (sex, age, time of follow-up, risk factors for skin cancer, TNM classification), histological data, treatments and outcome were reported.
Initial visits and follow-up where held in the Saint Louis Hospital, but, in certain cases, continued with the externally referred physician. In case of recurrence, patients were presented to the MTB again for evaluation and therapeutic decisions. For patients who had not been seen in the hospital for more than one year, recurrence information was obtained by phoning their referring physician. For patients who had not been seen by their referring physician in the last year of follow-up, survival status was obtained through their birth town civil status register. The study (reference number 2068938) was approved by the Commission National de l’Informatique et des Libertés (CNIL).
An electronic search was conducted of National Library of Medicine’s MEDLINE, Web of Science database and Cochrane Library databases for articles published until April 2016 in English, French and German. The reference lists of selected articles were reviewed to find studies of patients with SLNB and cSCC. Trials and series were included for analysis. Case reports were excluded. The search used the following combination of key words or MeSH terms: “sentinel lymph node biopsy, “skin tumour” and “squamous cell carcinoma”. Inclusion criteria used to select studies was series in whom patients underwent SLNB for non-relapsing unique cSCC. Selected patients from the series who had no other cSCC (other skin cancer, other SCC) were excluded from analysis. Data were extracted from reports by one reviewer (RL) with 2 blinded rounds of extraction. Data were pooled using a random-effect. To control for selection bias, when information was not available for all cases in a study, data were excluded from the detailed pooled analysis. To ensure comparability of the results, the methodology for histological analysis of the sentinel lymph node (HEC level and/or IHC) was reported for each study.
SLNB is used to correct node staging for cN0 cSCC cases, to plan a surgical therapeutic strategy, and to prevent nodal and metastatic progression in patient follow-ups. The main aims of the study were to evaluate positive SLNBs and the impact of SLNB results in cSCC progression and death. These objectives were studied in our population and in the published studies.
A further aim was to determine which clinical findings were predictive of positive SLNB and recurrence of cSCC, such as tumoural characteristics (staging, size, thickness, differentiation, and presence of perineural or vascular invasion) and patient characteristics (sex, age, time of follow-up). All patients recruited to our centre and and all of those reported in the literature were studied to determine these criteria using available data.
Summary statistics of both our patients and the published studies were reported as median [interquartile range; IQR] for continuous variables and as counts (percentages) for qualitative data. Percentages of positive SLNBs were estimated by averaging results from published studies and results from our study using a random effect model to take into account heterogeneity between studies.
Overall survival (OS) was defined as the delay between the date of diagnosis and the date of death. Relapse-free survival (RFS) was defined as the interval between the date of diagnosis and the first date between progression and death. OS and RFS were estimated using the Kaplan–Meier estimator.
Characteristics of patients with and without SLNBs were compared using either the Wilcoxon rank sum test or the Fisher’s exact test.
Among patients with negative SLNB results, association between baseline characteristics and RFS was estimated by hazard ratio using Cox proportional hazards models.
All statistical tests were 2-sided, with p-values of 0.05 or less denoting statistical significance. All analyses were performed using R package, version 3.0.2 (2013 Sept 5; http://www.R-project.org/).
A total of 327 patients were analysed; 37 from our series and 290 from the literature.
At our centre, 41 patients underwent SLNBs for cSCC during the inclusion period. Of these, 4 were excluded from analysis: 1 due to multiple lesions, 2 due to non-invasive cSCC (1 in situ and 1 keratoacanthoma), and 1 due to recurrent disease. The 37 remaining patients presented a solitary localized cSCC in all cases. The median age of patients was 72 years (IQR 65–78 years); 30 men, 7 women. Ten cases (30%) had additional immunosuppressive risk co-factors for cSCC (haematological malignancy in 6 cases, organ transplant in 4 cases).
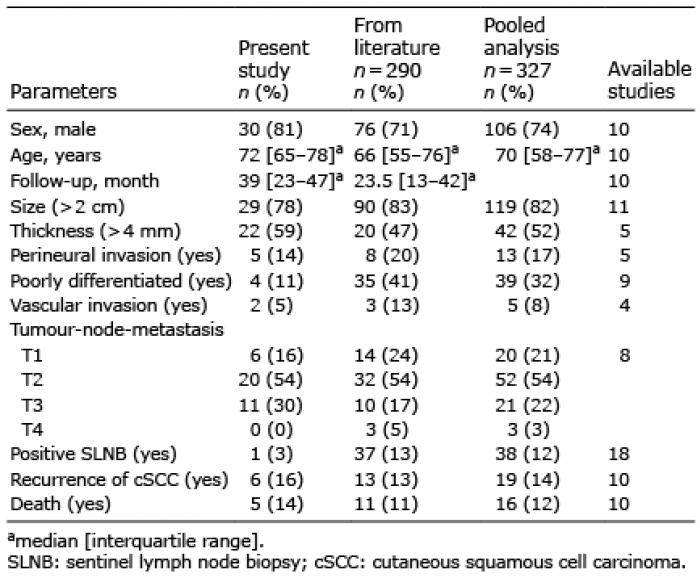
Within these 37 SNLBs, lymph node tissue was not found in one case, and the median number of nodes detected for the 36 others was 1, with an IQR of 1–2. Of these 36 remaining SNLBs, only one was observed to be positive (3%). The main patient characteristics are described in Table I.
Table I. Clinical characteristics of patients
The patient with a positive SLNB was a 69-year-old man, previously treated by chemotherapy for chronic lymphoid leukaemia. He presented in January 2014 with a 3-cm lesion on the face, for which histological examination revealed a well-differentiated SCC with a tumour thickness of 7 mm with no perineural or vascular invasion. The lesion was a T2-staged tumour for which initial excision was complete. SLNB evaluation was positive in 1 of the 2 lymph nodes examined. Following positive SLNB, the patient underwent lymph node resection, which did not find any other pathological nodes out of the 39 examined. Parotidectomy revealed an additional metastatic nodule. After surgery, the patient underwent radiotherapy. There was no recurrence after 2 years of follow-up.
Tumour staging categories using the AJCC (7) classification for cSCC were 6 patients (16%) with T1, 20 patients (57%) with T2, and 11 patients (30%) with T3. Clinical and histological high-risk factors were tumour size > 2 cm in 29 cases (78%), thickness > 4 mm in 22 cases (59%), perineural invasion in 5 cases (14%), and poor differentiation in 4 cases (11%) (4–7).
Median follow-up time was 38.7 months (IQR 23.4–46.7 months). During follow-up, 6 patients presented with recurrence. These patients all had negative SLNBs. Three patients presented with local recurrence and 3 with nodal and/or regional metastasis. Among the 3 patients with local recurrence, only one continued to progress and died from his tumour. Among the 3 patients with nodal and/or regional metastasis, 2 progressed and died from tumour dissemination. Two other patients died in the absence of recurrence, one after vascular surgery and the other due to an unknown cause.
In our series, no patient with stage T1 cSCC presented with recurrence. Three patients with stage T2 cSCC experienced recurrence (14%) and 2 of these patients died after progression of the tumour (10%). Three patients with stage T3 experienced recurrence (30%) and one of these patients later died as a result of tumour progression (10%).
Methodology for histological analysis of the sentinel lymph node (HEC level and/or IHC), was always performed on multiple sections of node biopsy.
Seventeen studies of SLNB in cSCC were found in a literature review (11–27), and a total of 290 individual cases were analysed (see Table I).
Tumour staging categories using the AJCC (7) classification for cSCC were 14 patients (24%) with T1, 32 (54%) with T2, 10 (17%) with T3, and 3 (5%) with T4. Clinical and histological high-risk factors were tumour size > 2 cm in 90 cases (83%), thickness > 4 mm in 20 cases (47%), perineural invasion in 8 cases (20%), and poor differentiation in 35 cases (41%) (4–7).
The median follow-up time was 23.5 months (IQR 13–42 months). During follow-up, 13 patients presented with recurrence, and 11 died.
Methodology for histological analysis of the sentinel lymph node (HEC level and/or IHC) was reported in 12 of the 17 studies. The HES was always performed on multiple sections of node biopsy and IHC was complemented in 10 of the 12 studies.
A total of 327 cases were analysed for SLNB outcomes in cSCC in 18 series, including ours. SLNBs were identified in 324 cases (99%) and were positive in 38 cases (12%). The mean positive rate of SLNB, using a random effect model for pooled analysis, was 0.14 (95% CI 0.09–0.22) (Fig. 1).
Fig. 1. Forest plot of sentinel lymph node biopsy (SLNB)-positive rates. The meanpositive rate of SLNB was 0.14 (95% CI 0.09–0.22) with a random effects model in meta-analysis of series.
Recurrence analysis was performed in 7 of these studies (12, 15, 19–22) and 98 cases. Eighteen patients experienced recurrence, with an RFS of 94.6% (95% CI 90.1–99.3%) at 1 year and 72.9% (61.9–85.8%) at 4 years. Among these patients, 3 had positive SNLB results and 15 had negative SLNB results. RFS (Fig. 2a) was not affected by SLNB status (p = 0.08, log-rank test). The methodology for histological analysis of the sentinel lymph node (HEC level and/or IHC) was reported in all studies that included recurrence analysis. The HES was always performed on multiple sections of node biopsy and IHC was complemented in 6 of the 7 studies.
Fig. 2. (a) Relapse-free survival based on sentinel lymph node biopsy (SLNB) status among 98 patients from 7 studies. Relapse-free survival was not affected by SLNB status (p = 0.08, log-rank test). (b) Overall survival based on SLNB status among 134 patients from 10 studies. Overall survival does not affected by SLNB status (p = 0.31, log-rank test).
Survival analysis was performed in 10 studies (12, 15, 18–22, 25–26) and 134 cases. Sixteen patients died, with an OS of 98.4% [95% CI 96.3–100%] at 1 year and 79.6% [95% CI 70.3–90.2%] at 4 years. Among these patients, 2 had positive SNLB results and 14 had negative SLNB results. OS (Fig. 2b) were not affected by SLNB status (p = 0.31, log-rank test). Methodology for histological analysis of the sentinel lymph node (HEC level and/or IHC) was reported in 9 of the 10 studies that included survival analysis. The HES was always performed on multiple sections of node biopsy, and IHC was complemented in 7 of the 9 studies.
Predictive factors for positive SLNB results are described in Table II. A poorly differentiated tumour was the only factor significantly associated with positive SLNBs.
Table II. Predictive markers for positive sentinel lymph node biopsies (SLNB)
Predictive factors for progression-free survival (PFS) in negative SLNB results are described in Table III. Again, poorly differentiated tumours were the only factor significantly associated with recurrence in patients with negative SLNB results (HR 3.33, 95% CI 1.17–9.36, p = 0.02).
Table III. Association between relapse-free survival and potential prognostic factors in negative sentinel lymph node biopsies (SNLBs)
We report here a large series of cSCC with SNLB analysis with exhaustive clinical and histopathological data. The SLNB-positive rate was lower than in the literature (3% vs. 14%, respectively). This difference could be explained by a lower rate of poorly differentiated cSCC (11% vs. 41%, respectively) in our study. Despite this finding, there was no difference in the recurrence and death rates between our cases and the literature (16% vs. 13%, and 14% vs. 11%, respectively). There was no difference in patient’s TNM status, tumour size or thickness, or perineural and vascular invasion between our study and studies selected from the literature.
This study shows that 14% of patients who underwent SLNBs have microscopic nodal metastases, after correction by a random effect model that takes into account heterogeneity in published studies. These results are in agreement with previous reviews on SLNBs in cSCC (28, 29). Only one histopathological risk factor, poor differentiation of the tumour, was associated with positive SLNB result. Poor tumour differentiation was also associated with recurrence in the case of negative SLNB results. The rate of positive SLNB results was greater than the expected rate of node metastasis in described in a previous review of cSCC cases (14% vs. 3.7%) (5), confirming a higher risk in patients who underwent SLNBs. TNM status was not significantly related to SLNB status, but revealed a trend toward increased positive SLNB results as tumour stage increased from T1 (6.2%) to T2 (22.9%) and T3 to T4 (40.9%).
The key result of this analysis was the absence of changes in PFS and OS in relation to with SLNB status. This information could impact on the decision about whether to propose SLNBs for cSCC. This has not been previously reported in the literature. Although the SLNB does not seem to be an aggressive procedure and has rare side-effects (15, 30, 31), its poor prediction value means that its use should be reconsidered.
One of the limitations of this study was the lack of a consensus definition of high-risk factors, as well as heterogeneous information about these factors among various studies. TNM was reported in 8 studies, and grading does not seem to be a key point in SLNB decisions, with inclusion of T1 stage 1 in 21% of cases of SLNB. Usual high-risk factors (4, 6, 32–35) were not reported exhaustively in the literature. Size was reported in 11 studies, thickness in 5, perineural invasion in 5, tumour differentiation in 9, and vascular invasion in 4. This heterogeneity decreases the power of our analysis.
There were no data showing that a diagnosis of lymph node metastasis in cSCC at the microscopic stage is of better prognostic value than when diagnosed at the macroscopic stage. In order to evaluate the usefulness of SLNB in cSCC more precisely there is a need for further powerful studies that include descriptive data for histopathological risks factors, tumour staging (AJCC, Brigham and Women’s Hospital), and/or comparison with control groups without SLNB (radiological and/or clinical follow-up).
In conclusion, this study added to our knowledge of the rate of positivity of SLNBs in cSCC. SLNB status does not correlate with PFS and OS in cases of cSCC. One risk factor (differentiation status) was associated with SLNB positivity and relapse, and relapse in the case of a negative biopsy. Therefore, SNLB should be used only in patients with higher risk factors, such as poorly differentiated tumours, and its use should be re-evaluated for prognosis of relapse and death in those situations.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize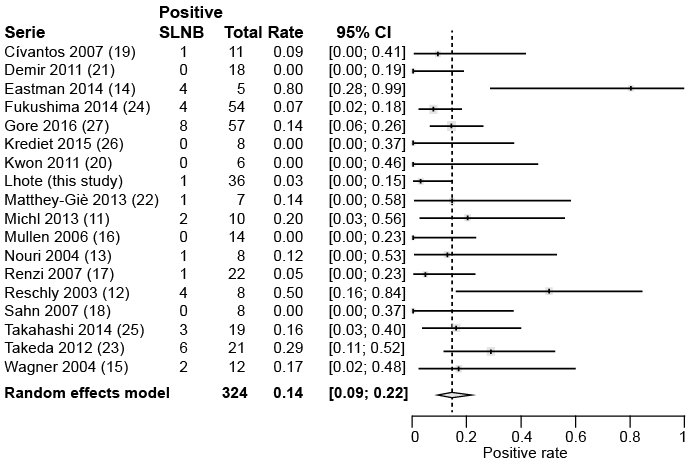 Click to show fullsize
Click to show fullsize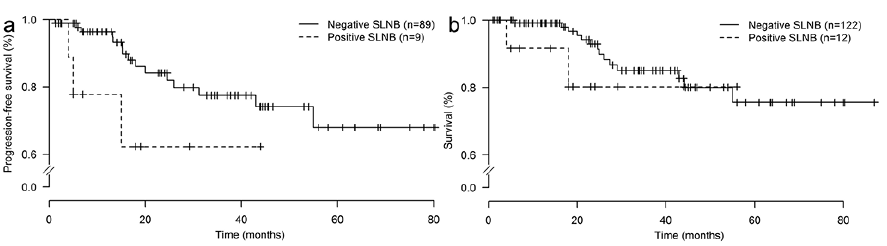 Click to show fullsize
Click to show fullsize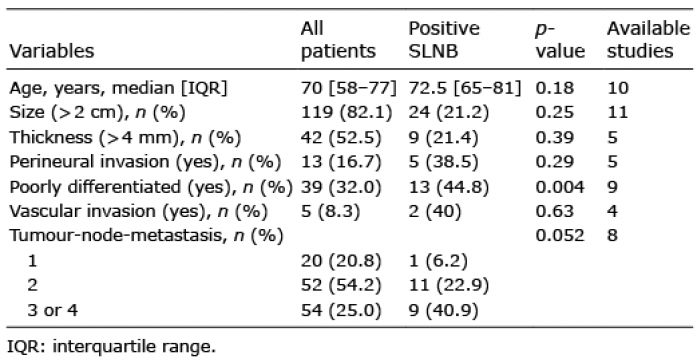 Click to show fullsize
Click to show fullsize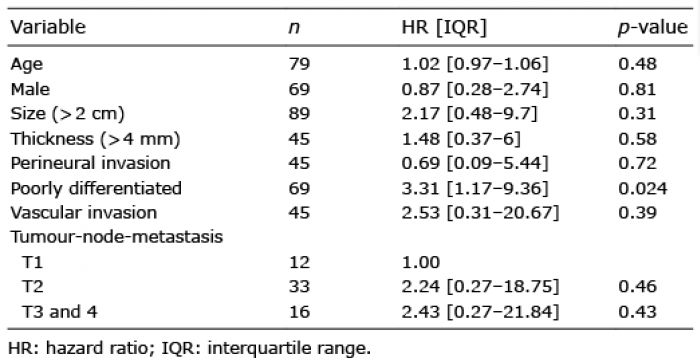 Click to show fullsize
Click to show fullsize