


1Department of Dermatology, Okayama University Graduate School of Medicine, Dentistry and Pharmaceutical Sciences, 2-5-1 Shikata-cho, Kita-ku, Okayama 700-8558, 2Division of Dermatology, Shizuoka Cancer Center Hospital, Shizuoka, and 3Department of Dermatology, National Hospital Organization Okayama Medical Center, Okayama, Japan. E-mail: ugn11252@nifty.com
Accepted Apr 24, 2018; Epub ahead of print Apr 24, 2018
Extramammary Paget’s disease (EMPD) is a rare cutaneous adenocarcinoma that primarily affects the genital area in elderly patients. In general, the prognosis of EMPD in patients with carcinoma in situ is good. How-ever, when EMPD becomes invasive, it has the potential to cause distant metastases after regional lymph node metastasis (1, 2). EMPD has non-specific visual features and is frequently misdiagnosed as other common skin diseases (e.g. eczema, psoriasis, and tinea). In such cases, inappropriate treatment may result in progression to advanced stages of the disease (3). Therefore, a cancer biomarker that properly reflects disease progression is required for early diagnosis of the disease.
Serum carcinoembryonic antigen (CEA) is a widely used biomarker for various adenocarcinomas, especially for colorectal cancer (4–6). Serum CEA has been reported to be useful in the management of EMPD (7–9). How-ever, the significance of serum CEA levels in patients with EMPD remains to be established.
The present study retrospectively analysed 72 cases of EMPD at a Japanese institute for analysing the use of serum CEA levels in disease management.
Serum CEA levels were measured in 72 patients with EMPD (42 men and 30 women) from April 2004 to January 2017 at the Department of Dermatology, Okayama University Hospital, Okayama, Japan. No patient had other forms of adenocarcinoma, such as colorectal cancer. Mean patient age was 72 years (range 44–88). Clinical staging was performed according to a recently reported classification (1). However, we lacked information regarding the tumour thickness and thus could not distinguish stage I from II. Therefore, EMPD was classified as stage I–II (without metastasis; n = 55), stage III (with regional lymph node metastasis; n = 7), or stage IV (with distant metastasis; n = 10).
The effects of chemotherapy were evaluated by measuring the size of the metastatic lesion in accordance with the Response Evaluation Criteria in Solid Tumors version 1.1 guidelines. The evaluation results were recorded as complete response (CR) and partial response (PR), stable disease (SD) and progressive disease (PD). All metastatic lesions were evaluated using enhanced computed tomography (CT) except for the left inguinal lymph node in case 3, which was evaluated using ultrasonography (Table SI).
Mean serum CEA levels were compared between the EMPD stage groups using the Mann–Whitney U test. The Wilcoxon signed-rank sum test was used to compare pre- and post-chemotherapeutic serum CEA levels. p < 0.05 was considered statistically significant.
The study was approved by the ethics committee of Okayama University Graduate School of Medicine, Dentistry and Pharmaceutical Sciences and Okayama University Hospital (number 1704-005).
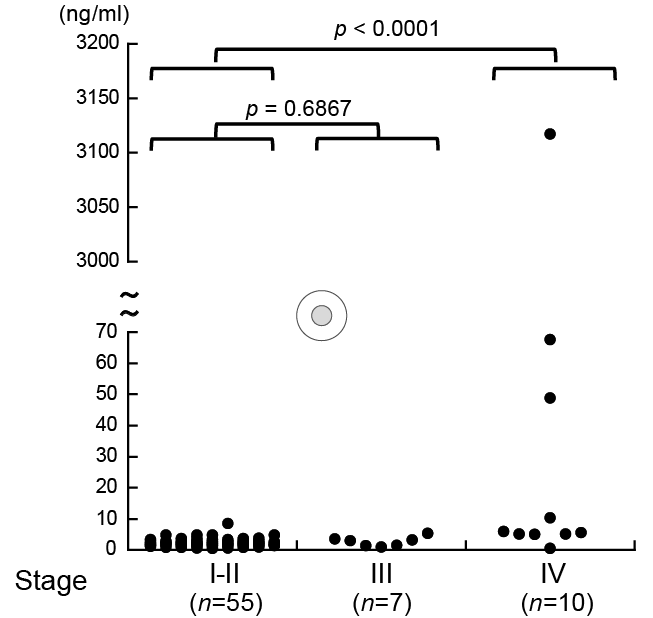
Serum CEA levels, obtained during the initial hospital visit, were significantly elevated in patients with stage IV (p < 0.0001) compared with those in patients with stage I–II EMPD. The levels were not significantly different in patients with stages III and I–II of the disease (p = 0.6867; Fig. 1). The cut-off value was set to 5.0 ng/ml; the calculated sensitivities of the serum CEA level were 1.8%, 14.3%, and 90.0% for patients with stages I–II (1 of 55), III (1 of 7) and IV (9 of 10), respectively. These findings suggest that serum CEA level is a useful marker in patients with EMPD and distant metastases.
Fig. 1. Compared with patients without metastases (stage I–II; n = 55), serum carcinoembryonic antigen (CEA) levels significantly elevated in patients with distant metastases (stage IV; n = 10, p < 0.0001). Serum CEA levels did not differ significantly between patients with (stage III) and those without regional lymph node metastasis (n = 7, p = 0.6867).
Among the 72 patients with EMPD, 9 underwent 16 courses of chemotherapy for treatment of metastatic lesions. A summary of changes in serum CEA levels is shown in Table SI. Among 19 patients undergoing imaging tests, none had a CR, 3 had a PR, one had SD, and 15 had PD. Three patients (cases 4, 7 and 8) had PR at some point during the treatment, but it eventually progressed to PD. Serum CEA levels significantly increased in all 15 patients with PD after chemotherapy compared with that before commencement of chemotherapy (p < 0.0001). In 3 patients, whose PR was determined, serum CEA levels decreased. Thus, serum CEA levels reflected the chemotherapeutic response as assessed using imaging tests.
In this study, serum CEA levels were highly sensitive in patients with EMPD and distant metastases. Reportedly, patients with EMPD and widespread metastasis had high serum CEA levels, whereas those without or with minimal metastases (n = 7) had normal serum CEA levels (7, 8). Our results not only confirmed these findings, but also showed a difference in serum CEA levels between patients with local and distant metastases. Hatta et al. (9) reported that elevated serum CEA levels are significantly associated with poor prognosis of EMPD. Our findings revealed that distant metastases are associated closely with high levels of serum CEA, but regional lymph node metastases are not. Based on our results, serum CEA levels could predict the presence of distant metastasis and help physicians decide when to initiate chemotherapy.
The false-positive rate of serum CEA level as a tumour marker has been reported to be 3.9% (10). In our study, only one of 55 patients without any metastasis (stages I–II) had an elevated level of serum CEA; we believe that this possibly was a false-positive result. Also, only one of 7 patients with regional lymph node metastasis (stage III) showed elevated serum CEA levels. In future, the significance of serum CEA levels in patients with EMPD and regional lymph node metastasis should be examined using a large subset of patients.
Among the various cancer biomarkers, serum CEA level is an established colorectal cancer marker that is used for prognosis and monitoring therapeutic outcomes (3–5). The use of serum CEA level has been extended to monitor therapeutic responses in breast and lung cancers (11, 12). A previous report demonstrated that serum CEA levels followed the disease course in a patient with EMPD (8). The current study confirmed that serum CEA levels reflected the chemotherapeutic response as evaluated using imaging tests in a larger number of patients. We believe that use of serum CEA levels in patients with EMPD can help detect distant metastasis promptly. Moreover, duration of follow-up and frequency of imaging tests for the detection of recurrent EMPD are not yet established (13). Therefore, serum CEA level monitoring has the potential to facilitate early detection of recurrent EMPD.
In a study that evaluated the use of serum CEA levels and cytokeratin 19 fragment 21-1 (CYFRA 21-1) in patients with EMPD without distant metastases, only CYFRA 21-1, not serum CEA levels, were high in some patients and were reduced following treatment (14). Therefore, it is possible that combined use of monitoring serum CEA level and CYFRA 21-1 may facilitate the management of patients at different stages of EMPD.
In conclusion, we suggest that high levels of serum CEA indicate the presence of distant metastasis in patients with EMPD, and that monitoring the levels can help evaluate their chemotherapeutic response. Large-scale studies are required to unequivocally recommend the use of serum CEA levels for improving treatment outcome of patients with advanced EMPD.
The authors are grateful to Dr Shigeki Umemura (Department of Thoracic Oncology, National Cancer Center Hospital East, Kashiwa, Japan) for providing insightful comments and suggestions on this work.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize