


Department of Dermatology, University of Occupational and Environmental Health, 1-1, Iseigaoka, Yahatanishi-ku, Kitakyushu City, Fukuoka 807-8555, Japan. *E-mail: long-ago@med.uoeh-u.ac.jp
Accepted May 29, 2018; Epub ahead of print Jun 1, 2018
The peripheral lymphoid organs are exposed to various external antigens. T-cell memory in the blood and lymph nodes is thought to sustain the defensive response against external antigens in peripheral lym-phoid organs. However, the concept of immune memory in peripheral tissues, mediated by resident memory T cells (TRM), has also been proposed (1). Cutaneous TRM also plays a pivotal role in drug eruptions (2). In some cases, drug eruption occurs during chemotherapy in a leukocyte nadir condition, indicating a possible role of cutaneous TRM in its pathogenesis (3). Patients with toxic epidermal necrolysis (TEN) sometimes develop alopecia areata (AA)-like lesions (4). TRM is located in hair follicles, thus it may also be involved in AA-like hair loss during drug eruption. We report here a case of AA-like hair loss accompanying TEN, in which an increased number of TRM was found in the lesion of AA-like hair loss.
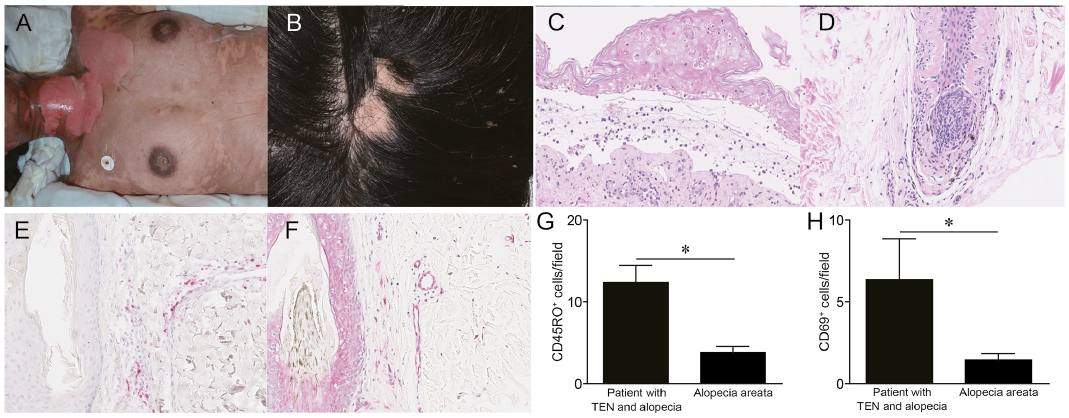
A 30-year-old Japanese woman was prescribed carbocysteine for upper bronchitis. Seven days after administration of the drug, erythematous plaques appeared on her trunk and extremities, which gradually developed into bullae, or vesicles, over her entire body (Fig. 1A). Mucosal erosions were observed in the oral cavity. At the same time, she had AA-like hair loss on the parietal region of the scalp (Fig. 1B). A skin biopsy from an erythematous plaque on the trunk revealed dyskeratotic keratinocytes and necrotic cells in the whole epidermal bulla and a sub-epidermal bulla (Fig. 1C). A metabolite of carbocysteine is a major causative agent for drug eruptions (5); however, we were unable to obtain consent from this patient for patch-testing with carbocysteine and its metabolites. A lymphocyte stimulation test (SRL Inc., Tokyo, Japan) was positive for carbocysteine (both 5 days and 2 weeks after onset), as described previously (6, 7). Although we could not exclude the involvement of metabolites of carbocysteine in the development of the drug eruption, we diagnosed her skin eruption as TEN, based on its clinical course and histological examination. Intravenous immunoglobulin therapy was administered following systemic pulsed steroid therapy, resulting in parallel improvements in the skin eruption and AA-like hair loss.
Fig. 1. Clinical manifestation and histological examination. (A) Clinical manifestation of toxic epidermal necrolysis (TEN) showing diffuse blisters and erosions on the patient’s trunk. (B) Clinical manifestation of alopecia areata (AA) showing non-scarring type of hair loss. (C) Histopathology of the skin. Haematoxylin and eosin (H&E) staining of the skin (x190) showing necrotic keratinocytes in all epidermal levels. Inflammatory cells are seen in the superficial dermis. (D) Histopathology of the skin. H&E staining of the skin (x190) showing dyskeratosis of the epidermis and atrophy of hair follicles. (E) Immunostaining for CD45RO in the scalp skin (×200). (F) Immunostaining for CD69 in the scalp skin (×200). (G, H) The number of (G) CD45RO-positive cells and (H) CD69-positive cells in the skin. The number of immunoreactive lymphocytes was determined from 3 high-power fields (×400) in the dermis of each immunostained section from the current patient and from 6 patients with AA.
Because the patient’s skin eruption exhibited the same clinical course in TEN and AA-like hair loss, we suspected that her drug eruption might be contributing to the AA-like hair loss. Therefore, we performed histological analysis of the lesion of AA-like hair loss. Skin biopsy revealed hyalinization and dyskeratotic keratinocytes in the hair follicles, with peri-follicular lymphocytic infiltration (Fig. 1D). To determine the presence of TRM in the skin, we then analysed the distribution of CD45RO+ (memory cell marker) and CD69+ (resident cell marker) cells. Interestingly, CD45RO+ and CD69+ cells also infiltrated AA-like lesional skin in this patient (Fig. 1E, F). These cells were significantly increased compared with patients with ordinal AA (Fig. 1G, H). Since TRM has been shown to contribute to the pathogenesis of drug eruption (2), these findings suggest that the patient’s AA-like hair loss might develop during the course of the drug eruption. Infiltration of CD45RO+ and CD69+ cells was shown in the lesion of AA-like hair loss in this patient with TEN, thus it is speculated that a carbocysteine or its derivative might cause TRM activation in the whole skin, including the hair follicles, leading to damage to the epidermis and hair follicles. Further research is needed to clarify the detailed mechanism of AA-like hair loss accompanying TEN.


 Click to show fullsize
Click to show fullsize