


1Department of Dermatology, 2Department of Histopathology, Royal Victoria Infirmary, and 3Institute of Genetic Medicine, University of Newcastle upon Tyne, NE1 3BZ Newcastle upon Tyne, UK. *E-mail: neil.rajan@ncl.ac.uk
#These authors contributed equally to this work.
Accepted Jun 5, 2018; Epub ahead of print Jun 8, 2018
Cutaneous squamous cell carcinoma (cSCC) is one of the leading causes of skin cancer mortality (1). The recognition of, and stratification by, histological subtype is important in the prognostication of outcome. Follicular, or infundibulocystic, cSCC is a recently described subtype which is thought to arise from follicular cells and is estimated to account for approximately 1.3% of cSCC (2). Fewer than 90 cases have been reported, and this poorly understood form may be more common than previously thought (3). Hence the development of follicular cSCC in rare genetic conditions such as CYLD cutaneous syndrome (CCS) is informative and provides insights into tumour pathogenesis. Multiple familial trichoepitheliomas (MFT) is one of 3 phenotypes reported in CCS, and is associated with rare, germline mutations in CYLD (4). In this report we present a case of a follicular cSCC in a patient with the MFT phenotype.
A 56-year-old woman presented with an ulcerated tumour on the dorsum of her left-hand (Fig. 1a). It had been increasing in size over the preceeding 4 months and was reported not to have arisen from a preexisting skin lesion. She had first presented in her teens with multiple facial papules that, after excision from her melolabial skin, were confirmed to be trichoepitheliomas. At the age of 53, a benign vulval cylindroma was excised. She had a history of significant UV exposure, having spent 4 months per year in Turkey for the past 10 years. She had two children, who both developed MFT in their teens, one of whom had been confirmed to have pathogenic mutation in CYLD (c.1112C>A). Skin examination of the patient revealed freckling and subtle poikiloderma consistent with her history of UV exposure. The tumour on the dorsum of her hand was a pink ulcerated nodule measuring 20 × 26 mm (Fig. 1A). The skin on her face had numerous, skin-coloured papules consistent with trichoepithelioma. No lesions were otherwise noted on the arms or torso. A punch biopsy of the nodule on the hand revealed features compatible with either trichofolliculoma or adnexal basal cell carcinoma. Clinicopathological correlation raised the suspicion of trichoblastic carcinoma or squamous cell carcinoma. As trichoblastic carcinoma has been reported to metastasize (5), a staging workup, including computerized tomography (CT) of the chest and abdomen was performed, and did not find evidence of systemic metastasis.
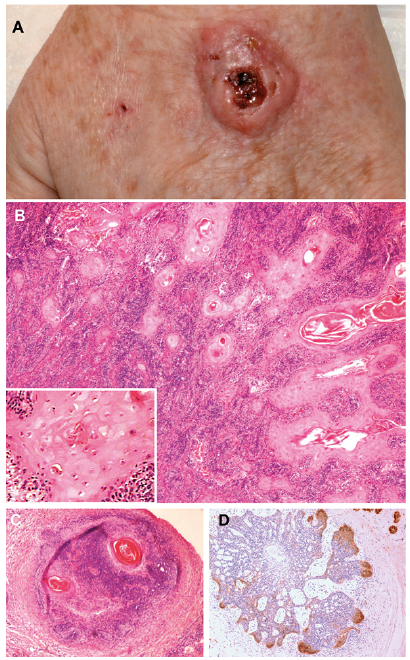
Fig. 1. (a) Follicular squamous cell carcinoma (SCC). Ulcerated nodule measuring 20 x 26 mm on the left-hand dorsum growing faster and larger than her other lesions. (b) Poorly differentiated follicular cutaneous SCC on Mohs debulk specimen. (c) H+E of positive Mohs stage demonstrating features consistent with trichofolliculoma. (d) BerEp4 immunostaining of positive Mohs stage demonstrating increased expression at the infiltrative margin. (H+E: original magnification 10x; inset: 40x).
The tumour was then excised using Mohs micrographic surgery (MMS) and took 4 stages to clear, leaving a defect of 52 by 52 mm. The debulk specimen showed poorly differentiated follicular cSCC, which was 6 mm thick and had an infiltrative growth pattern (Fig. 1B). Positive Mohs stages, however, showed basaloid nests of immature palisading tumour cells in the dermis, consistent with trichofolliculoma (Fig. 1C). BerEp4 staining was negative in the debulk and positive in the Mohs stages (Fig. 1D). There was no evidence of recurrence or distant metastasis during a 3-year follow-up period.
Follicular cSCC is a relatively uncommon subtype of cSCC that has only been recently recognised (3), and hence our finding of this tumour type on the genetic background of a germline CYLD mutation is of interest. The genetic mechanism underpinning this link is not yet clear. CYLD loss has been reported in sporadic human cSCC (6), and has been shown to increase cSCC invasion in mice. It is of interest that recently in oral squamous cell carcinoma, CYLD loss is seen as driving factor that facilitates invasion, via upregulation of TGF-Beta signalling (7), a pathway implicated in cSCC (8). We have not studied our sample for CYLD loss; however, given that CYLD loss is seen in cylindroma and spiradenoma, it is possible that it may play a role in the development of follicular cSCC.
Patients with CCS may present with 3 distinct but overlapping cutaneous phenotypes: MFT, where the predominant tumours are facial trichoepitheliomas, familial cylindromatosis (FC) where the predominant tumours are scalp cylindromas, and Brooke-Spiegler syndrome (BSS), where any combination of trichoepitheliomas, cylindromas and related spiradenomas are seen (4). MFT, FC and BSS are all associated with mutations in CYLD, a tumour suppressor gene in which more than 100 mutations have been reported (9). The genetic factors that cause these different presentations are unknown, and all patterns can present in individuals from multigenerational families where the same CYLD mutation is seen (4).
Cutaneous malignancy is an infrequent but recurrent feature in CCS, and hence monitoring is needed to detect clinically suspicious growing tumours. In patients with predominantly cylindromas and spiradenomas (FC and BSS), cylindrocarcinoma and spiradenocarcinoma are recognised to have a basal cell adenocarcinoma-like morphology and typically arise from benign pre-existing cylindroma and spiradenoma on biopsy (10). In patients with predominantly trichoepitheliomas, 3 patterns of malignancy are seen. MFT patients may develop pink papules which are basal cell carcinomas and these have been shown to arise in contiguity with trichoepithelioma, suggesting that transformation is from pre-existing benign trichoepitheliomas, a feature corroborated by histology (11). Secondly, some patients have been reported to develop nodules which may be ulcerated, with histology relating to follicular carcinoma, including trichoblastic carcinoma (5) or malignant hair matrix tumour (12). A third pattern has been outlined in recent reports, describing patients with larger lesions (3–5 cm) that are ulcerated, rapidly growing and distinct from surrounding tumours. Histological reports from these larger tumours are consistent with a diagnosis of cSCC (13, 14). In one case, the tumour recurred despite repeated surgical excision and radiotherapy, resulting in the patient’s demise associated with intracranial invasion (14). Taken together with our case, these occurrences are difficult to dismiss as coincidental. It may be of clinical relevance that these reports are of patients from China and India (13, 14). White patients with European ancestry that have MFT typically develop small (< 1 cm) skin-coloured trichoepitheliomas (TEs) on the melolabial skin, forehead and chin. It has been previously observed in isolated reports that in patients from Asian and African genetic backgrounds, facial TEs may be much larger (4). Furthermore, confluent scalp cylindromas as seen in FC (historically termed “turban tumours”) have not been reported in patients with Asian and African ancestry. This could suggest that there may be genetic factors that influence tumour type and location in CSS that also impact on formation of cSCC.
We report the novel finding of follicular cSCC in CCS, and the lack of recurrence 3 years after excision with MMS. Notably, it took 4 stages to achieve clear margins and it is likely that standard margins for excision would have resulted in incomplete excision. cSCC in CCS may have an adverse outcome, and as such, patients should be instructed to report tumours that are ulcerated, increasing in size or are visibly different to the benign tumours these patients develop for clinical and histological assessment. The morbidity associated with cSCC in these rare cases supports the use of MMS, as performed in our case.
NR is a Wellcome Intermediate Clinical Fellow WT097163MA.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize