


Departments of Dermatology: 1National Taiwan University Hospital Hsin-Chu Branch, Hsinchu, 3National Taiwan University Hospital, 4College of Medicine, National Taiwan University, Taipei, 5Chang Gung Memorial Hospital, Linkou Branch, Taoyuan, 7Drug Hypersensitivity Clinical and Research Center, Chang Gung Memorial Hospital, Linkou, 8Far Eastern Memorial Hospital, New Taipei, 9Chung Shan Medical University Hospital, Taichung, Taiwan and 10Chung Shan Medical University, Taichung, 2Institute of Biomedical Engineering, College of Medicine and College of Engineering, National Taiwan University, and 6School of Medicine, College of Medicine, Chang Gung University, Taoyuan, Taiwan
Safety data for secukinumab in patients with psoriasis and viral hepatitis are lacking. The aim of this study is to investigate the risk of reactivation of hepatitis B virus (HBV)/hepatitis C virus (HCV) in patients with psoriasis who are receiving secukinumab therapy. This multicentre study screened 284 patients with psoriasis with available HBV and HCV serological data and 63 patients with concurrent HBV/HCV infection were enrolled. In the absence of antiviral prophylaxis, 7 of 46 (15.2%) patients with HBV exhibited HBV reactivation during secukinumab therapy. The risk of reactivation was significantly higher in HBsAg-positive patients, compared with HBsAg-negative/HBcAb-positive patients (24.0% vs. 4.17%, p = 0.047). One of 14 (7.1%) HCV patients showed enhanced replication of HCV with hepatitis. No virus reactivation occurred in patients receiving antiviral prophylaxis. HBsAg-positive and HBsAg-negative/HBcAb-positive psoriasis patients can develop virus reactivation during secukinumab therapy, thus necessitating close monitoring of viral load and considering an antiviral prophylaxis for all HBsAg-positive patients with psoriasis.
Key words: psoriasis; secukinumab; hepatitis B; hepatitis C; interleukin-17A inhibitor; biologics.
Accepted Jun 5, 2018; Epub ahead of print Jun 8, 2018
Acta Derm Venereol 2018; XX: XX–XX.
Corr: Tsen-Fang Tsai, Department of Dermatology, National Taiwan University Hospital, No.7 Chung San South Road, Taipei, Taiwan. E-mail: tftsai@yahoo.com
This study showed that biologic agents alter the competence of the host immune-surveillance system to combat hepatitis virus infections and hepatitis B virus (HBV) or hepatitis C virus (HCV). Reactivation can occur in patients with psoriasis with concurrent HBV or HCV treated with secukinumab, an anti-interleukin 17 agent. The risk of virus reactivation varied in patients with psoriasis with different virological profiles. It is advisable to monitor the viral load/serum transaminase level and consider antiviral prophylaxis for all hepatitis B surface antigen-positive patients with psoriasis who are being treated with secukinumab.
In the past decade, the emergence of biologic therapies, including anti-tumour necrosis factor (anti-TNF-α), anti-interleukin (anti-IL) 12/23 p40 monoclonal antibody, and the recently approved anti-IL-17/IL-17R antibody, has substantially improved the treatment outcome of patients with psoriasis (1). However, safety concerns over the use of biologics still exist, especially in view of opportunistic infections, such as those caused by mycobacterial, bacterial, viral and fungal agents (2). Moreover, biologic agents alter the competence of the host immune-surveillance system to combat hepatitis virus infections, which may increase virus reactivation and replication, resulting in injury to the liver (3, 4). Recent years have witnessed an increase in the number of cases of reactivation of hepatitis B (HBV) or hepatitis C (HCV) virus in patients with psoriasis who are receiving biologics (3, 5, 6).
Secukinumab, a monoclonal antibody that selectively binds and neutralizes IL-17A, has demonstrated high efficacy in treating moderate-to-severe plaque psoriasis (7). However, IL-17, a major effector cytokine of T-helper 17 (Th17), has been shown to mediate host defence mechanisms in response to various infective agents (8). Emerging research has also shown that Th17 response is involved in various viral infections (9–11). Studies suggest that IL-17 plays a role in eliciting innate defence at mucosal sites and inducing infection-associated immunopathology during viral infections (12). Moreover, Th17 response is involved in the pathogenesis of viral hepatitis. The number of intrahepatic IL-17 and circulating IL-17-producing peripheral blood mononuclear cells was found to be signi?cantly increased in patients with HBV and HCV infection (4). Available data also suggest that IL-17 plays an important role in suppressing HBV activity (4), and that Th17 cells drive the immune-mediated pathology of HBV and HCV (4). However, safety data for secukinumab in patients with psoriasis and viral hepatitis are lacking because these patients are always excluded from pivotal trials. Therefore, we conducted a multicentre study to assess the risk of virus reactivation in patients with psoriasis with concurrent HBV or HCV infection during secukinumab therapy and the usefulness of antiviral prophylaxis in real-life practice.
This multicentre study prospectively included all patients with psoriasis with concurrent HBV or HCV infection, who had been treated with secukinumab from June 2015 to January 2018, at 4 dermatology centres from the different regions of Taiwan. All patients had been treated with secukinumab for a minimum of 3 months. Subcutaneous injections of secukinumab (300 or 150 mg) were administered at baseline and weeks 1, 2 and 3, and thereafter every 4 weeks. The dosage of secukinumab was determined by the physicians on the basis of body-weight, economic reasons, and reimbursement policy in Taiwan. In Taiwan, because of the relatively high prevalence of HBV and HCV infection (13), all patients treated with secukinumab underwent pretreatment screening for HBV and HCV markers. The serological findings for positive HBV infection was subdivided into 3 categories according to the 2014 National Psoriasis Foundation recommendations: (i) chronic HBV infection (HBsAg-positive), (ii) resolved HBV infection (HBsAg-negative, HBsAb-positive, and HBcAb-positive), and (iii) occult HBV infection (HBsAg-negative, HBsAb-negative, and HBcAb-positive) (14). HCV infection was de?ned by the seropositivity of anti-HCV antibody.
HBV DNA/HCV RNA levels and serum alanine transaminase (ALT) and aspartate transaminase (AST) levels were monitored at baseline, regularly during secukinumab therapy (months 1, 3 and 6, and thereafter every 3 months), and at the end of treatment or follow-up. Patients without viral load data at baseline or at a minimum of 2 different time-points were excluded. As recommended by various guideline (14, 15), patients with positive HBV- or HCV-carrier status are suggested to receive antiviral prophylaxis. However, based on the Bureau of National Health Insurance (BNHI) reimbursement policy in Taiwan, prophylactic use of antiviral therapy for HBV carriers is restricted to patients with cancer undergoing chemotherapy, or organ-transplant patients undergoing immunosuppressants. The BNHI does not reimburse the cost of antiviral therapy for patients without cancer or organ transplant who receive biologics. If patients declined prophylaxis, they are regularly reviewed by hepatologists.
Ethics approval was obtained from the local Institutional Review Board of the National Taiwan University Hospital (201709006RIND and 201106079RC); National Taiwan University Hospital, Hsin-Chu branch (103-030-E); Chang Gung Memorial Hospital, Linkou and Taipei branches (98-2267A3).
HBV virological reactivation was de?ned as a 10-fold increase in the HBV-DNA load, compared with the baseline value or a switch from the ”undetectable” to the ”detectable” status, and/or hepatitis B e antigen (HBeAg) seroconversion from negative to positive after secukinumab therapy (6, 16, 17). Hepatitis was defined as a ≥ 3-fold increase in ALT level that exceeded the upper limit of the normal value or an absolute increase in ALT level to > 100 IU/l (18). Enhanced replication of HCV was de?ned as the reappearance of HCV RNA for spontaneously resolved or treated patients or an increase of over 10-fold in post-secukinumab serum HCV RNA compared with the baseline level (19). HCV reactivation was defined as an enhanced replication of HCV with hepatitis (20, 21).
To detect intergroup differences, the data were analysed using the Student’s t-test or Wilcoxon rank-sum test for continuous variables, and the Fisher’s exact or χ2 test for discrete variables. The serum viral loads observed during the follow-up period before and after secukinumab therapy were compared using the paired t-test for normally distributed data and Wilcoxon signed-rank test for non-normally distributed data.
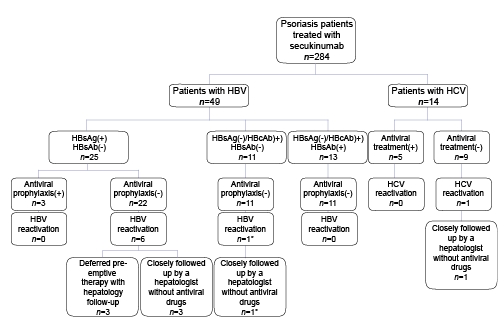
A total of 284 consecutive patients with psoriasis who were receiving secukinumab therapy were screened for this study. Finally, the data for 49 patients with HBV infection and 14 patients with HCV infection were included (Fig. 1). Pre-therapy demographic data and serological and virological findings of patients are summarized in Table I and Table SI.
Fig. 1. Schematic representation of psoriasis patients with concurrent hepatitis B virus (HBV) or hepatitis C virus (HCV) infection on secukinumab therapy enrolled in this study. *Positive viral load at baseline.
Table I. Baseline demographic data and laboratory ?ndings for patients with psoriasis and different hepatitis B virus (HBV) and hepatitis C virus (HCV) infection status
Twenty-five of the 49 patients (51%) had chronic HBV infection, 13 (26.5%) had resolved HBV infection, and the other 11 (22.5 %) were infected with occult HBV at the time of recruitment (Fig. 1). One patient presented with concurrent HBV and HCV infection. Serum HBV-DNA load was undetectable in one (4%) patient with chronic HBV infection and 11 (45.8%) patients with occult or resolved HBV infection at baseline. Four of 49 patients (8.2%) used concomitant immunosuppressants or immunomodulators in addition to secukinumab. Three patients with HBV infection received antiviral prophylaxis, in the form of 600 mg telbivudine or 0.5 mg entecavir daily (Table I). None of the patients developed HBV reactivation. HBsAg-negative/HBcAb-positive patients (with resolved or occult HBV infection) had lower viral loads, compared with patients who tested positive for HBsAg at baseline (10.8 vs. 188,861.7 IU/ml, p < 0.001), but one of them developed HBV reactivation during the 3-month-long secukinumab therapy (Fig. 1).
Clinical and demographic data for the 14 subjects who had concomitant psoriasis and HCV infection are summarized in Table I. The mean HCV RNA level was 1,770,739.5 ± 3,908,098.4 IU/ml, and 4 patients presented with a slight increase in the baseline AST/ALT levels. Four patients had been treated with pegylated interferon-alpha2b and ribavirin. Among them, 3 patients achieved sustained virological response and the HCV RNA level was undetectable before the initiation of secukinumab therapy. Another patient with type Ib HCV infection and liver cirrhosis (Child-Pugh score A) received antiviral drugs. Because he met the criteria for National Health Insurance (for antiviral drug), he received dasabuvir (250 mg) twice daily, and ombitasvir (25 mg)/paritaprevir (150 mg)/ritonavir (100 mg) daily, along with secukinumab. The HCV viral load promptly decreased within 3 months of antiviral therapy.
Table SI shows the characteristics, management, and outcome of the 8 patients who experienced HBV reactivation or enhanced replication of HCV. There were no signi?cant differences in the mean serum ALT level and HBV or HCV viral load between the baseline and post-therapy (Fig. S1). However, 7 of 46 (15.2%) patients with HBV who did not receive antiviral prophylaxis developed HBV reactivation after 3.4 ± 2.8 months (range 1–9 weeks). The risk of HBV reactivation appeared to be significantly higher in HBsAg-positive patients, compared with HBsAg-negative/HBcAb-positive patients (24.0% vs. 4.17%, p = 0.047). One of the 14 patients with HCV infection (7.1%) developed enhanced replication of HCV with hepatitis after 3 months of secukinumab therapy. All of these patients were clinically asymptomatic at the time of reactivation. Of these 8 patients, 3 with HBV infection were receiving pre-emptive antiviral therapy with telbivudine, and the other 5 were closely followed by hepatologists without antiviral drugs. The viral load decreased rapidly within 3 months of antiviral therapy. In 4 HBV-infected patients who were not receiving antiviral therapy, the HBV DNA load remained stable as a low-titre value, without acute hepatitis. Nevertheless, biologic hepatitis was observed only in the one patient who showed enhanced replication of HCV, whose viral load and elevated ALT level subsequently reduced, without the administration of antiviral drugs (Table SI). None of these patients adjusted or discontinued the secukinumab therapy.
Two cases, one with HBV and the other with HCV, developed hepatic cancer during the secukinumab treatment. The 58-year-old male with a 10-year history of psoriasis had chronic HCV infection (Type Ib). He had not received interferon alpha-2a or ribavirin previously, but was followed up regularly at a hepatologist clinic. Liver cirrhosis, abnormal liver function and hepatic tumour were not noted before secukinumab treatment. He had an 85% reduction in Psoriasis Area and Severity Index (PASI), but developed hepatocellular carcinoma (HCC) after a 6-month treatment of secukinumab without a significant change in HCV viral load. Another 52-year-old man had psoriasis for 20 years and was diagnosed as HBeAg-negative chronic hepatitis B infection without liver cirrhosis 7 years prior to secukinumab treatment. He had not received any antiviral drugs, abdominal ultrasonography or hepatology outpatient clinic follow-up previously. Six months after secukinumab treatment, he was diagnosed with combined hepatocellular-cholangiocarcinoma with initial presentation of pain in the right flank. However, no evidence of viral reactivation or elevation of serum aminotransferase levels were observed.
Biologic agents can disturb the delicate balance between the degree of virus replication and host immune control, which may thereby cause virus reactivation. Perez-Alvarez et al. (22) found that HBV reactivation occurred in 35 of 89 (39%) HBsAg carriers receiving TNF-α inhibitors. However, the aforementioned studies included not only patients with psoriasis, but also patients with other rheumatic and digestive diseases (22). A more recent review by Snast et al. (17) included 40 patients with psoriasis with chronic HBV infection and found that virus reactivation was documented in 8 (20%) patients on biologic therapy. Our previous study showed that 2 of 7 (29%) patients, not receiving antiviral prophylaxis, exhibited HBV reactivation during treatment with IL-12/23 p40 monoclonal antibody ustekinumab (6). In the present study, the HBV reactivation rate in patients with psoriasis who were positive for HBsAg and did not receive antiviral prophylaxis was 24%, which was lower than that observed in previous studies. Differences in the definition of virus reactivation, the interval of viral DNA or RNA load monitoring, concurrent use of immunosuppressants, and the intensity and duration of biologic therapy can account for the differences in the incidence of reactivation (22–24).
Studies investigating the safety profile of biologic agents in the context of HCV infection are scarce and are limited to small case series with a short follow-up. A systematic review of the literature by Brunasso et al., including the data of 153 patients with HCV infection treated by anti-TNF-α agents, showed that 8.8% among patients affected by rheumatoid arthritis and 4.2% among patients with psoriasis (25) had changes in the HCV-related conditions (worsening of HCV viral load and/or elevation of liver enzyme levels and/or histological demonstration of hepatic worsening). Our previous data also showed that one of 4 patients with psoriasis (25%) with HCV developed HCV reactivation during ustekinumab therapy (6). In this study, one of 14 (7.1%) patients with psoriasis treated with secukinumab experienced HCV enhanced replication, which was consistent with the frequency noted in medical literature. A higher titre of serum HCV RNA has been associated with an increased risk of the development of HCC (26) and may affect the treatment response in advanced HCV infection (27). However, the relationship among HCV viral load, aminotransferase activities, liver fibrosis and liver-related mortality remained controversial (28, 29). More large-scale studies are needed to better elucidate the relationship between changes in HCV viral load and liver outcomes during treatment with secukinumab.
Antiviral prophylactic therapy is strongly recommended by the European Association for the Study of Liver Disease (EASL) guideline for avoiding reactivations in HBsAg-positive patients undergoing immunosuppressive therapy (30). None of the patients receiving antiviral prophylaxis developed virus reaction in our study, reinforcing the importance of receiving prophylaxis. Moreover, EASL 2017 guidelines also suggested that HBsAg-negative/HBcAb-positive patients with positive viral load at baseline may be managed as if they were HBsAg carriers, and antiviral prophylaxis could be administered before starting immunosuppressive therapy, although the risk of HBV reactivation varies widely in patients with occult HBV infection (30). In EASL Recommendations of Hepatitis C 2016, there is no special management or antiviral prophylaxis recommended for HCV in the setting of biological therapy (31, 32). The optimal timing of direct-acting antivirals and biologics in HCV-infected patients is also unknown (33).
Accumulating research has uncovered pivotal roles of the IL-23/Th 17 cell axis in HBV and HCV infection. The increase in IL-17 level can be correlated with severe liver damage, which might contribute to viral clearance, in patients with acute HBV infection (12, 34). Moreover, many studies have indicated that serum IL-17 level and IL-17 production in CD4+ T cells were elevated in subjects with HCV infection (35, 36). The Th17/IL-17 axis was also found to be involved in HBV or HCV infection-associated fibrogenesis, resulting in clinical liver cirrhosis (33).
However, only one case report (37) and 3 patients with coexisting HBV infection undergoing secukinumab therapy were included in a recent study (17). None of the patients experienced hepatitis or virus reactivation. Nevertheless, of the 4 patients, 3 had resolved HBV infection, and the other patient, an inactive-HBV carrier, received an antiviral (entecavir) along with secukinumab. The effect of IL-17A antagonists on the course of HBV and HCV infection, in particular in patients positive for HBsAg and anti-HCV, has not been thoroughly investigated in previous studies.
Previous studies have suggested that IL-17 is associated with increased risk of tumorigenesis, invasiveness and metastasis (38–40). Increased pretreatment levels of IL-17 were also associated with poor prognosis and early recurrence of HCC (38). Nevertheless, some researchers suggested that L-17A play a role of enhancing the immune system against tumorigenesis (41, 42). In the pooled safety data from pivotal clinical trials, the analysis showed that the incidence of malignancy in patients receiving secukinumab is in line with expected rates for patients with psoriasis (43).
This study has certain limitations; it has a hospital-based design and small sample size. Because of the spontaneous fluctuating nature of HBV/HCV viral load (44-46), the lack of a comparison group including patients with psoriasis without systemic treatment might interfere with assessment of the exact effect of secukinumab on virus reactivation.
Although there is a considerable risk of virological reactivation during secukinumab therapy, the benefit-risk ratio in patients with psoriasis with concurrent HBV or HCV infection can be justified. During secukinumab therapy, HBV reactivation can occur in both HBsAg-positive and HBsAg-negative/HBcAb-positive patients with detectable HBV DNA. Antiviral prophylaxis effectively reduces the risk of virus reactivation in HBsAg-positive, who are receiving secukinumab therapy. Considering the high rate of reactivation, antiviral prophylaxis was suggested for all HBsAg-positive patients with psoriasis who are receiving secukinumab treatment. Close follow-up with periodic HBV DNA should be considered in patients with psoriasis with concurrent HBV infection, but low viral loads receiving secukinumab therapy in the absence of combination antiviral therapy. Patients with psoriasis with concurrent HCV still have a risk of developing enhanced viral reactivation with hepatitis throughout the secukinumab treatment period. Thus, periodic monitoring of HCV RNA loads with serum aminotransferase determination is recommended for the follow-up of these patients. In addition, the risk of HCC should be closely monitored, even in patients without viral reactivation, during treatment with secukinumab.
Funding. This work was supported in part by grants from the National Taiwan University Hospital, Hsin-Chu branch (HCH 106-HCH055 and 107-HCH057) and Chang Gung Memorial Hospital (CMRPG2F0332), and in part by Basic Research Award, Asia-Pacific La Roche-Posay Foundation 2014. The funders had no role in study design, data collection and analysis, interpretation of findings, manuscript writing, and target journal selection.
Competing interests. All authors have completed the ICMJE uniform disclosure form (available at www.icmje.org/coi_disclosure.pdf), and declare that: T-FT has conducted clinical trials or received honoraria for serving as a consultant for AbbVie, Boehringer Ingelheim, Celgene, Eli-Lilly, Galderma, GSK, Janssen-Cilag, Leo Pharma, Merck-Serono, Novartis International AG, and Pfizer Inc. H-YC, P-JL, T-SW and RCH have received speaking fees from AbbVie, Novartis Pharmaceuticals Corp., Janssen-Cilag Pharmaceutica, and Pfizer Ltd. Y-CT have received speaking fees from Novartis Pharmaceuticals Corp., Janssen-Cilag Pharmaceutica, and Pfizer Ltd. Y-HH has conducted clinical trials for serving as a principal investigator for Galderma, Eli-Lilly, Novartis Pharmaceuticals Corp., and Janssen-Cilag Pharmaceutica, received honoraria for serving as an advisory board member for Pfizer Ltd, AbbVie, and Celgene, and received speaking fees from AbbVie, Eli-Lilly, and Novartis Pharmaceuticals Corp. RH and K-LC have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize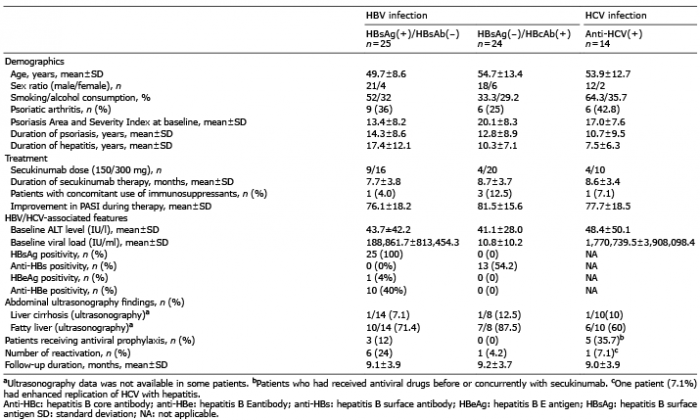 Click to show fullsize
Click to show fullsize