


1Department of Dermatology, University François Rabelais Tours, CHRU Tours, Tours, 2SPHERE - INSERM 1246. University of Tours and Nantes, 3Department of Teaching and Research in General Practice, University Nice Sophia Antipolis, Nice, 4Department of Allergology and Immunology, University Hospital Center of Lyon, Lyon, 5Department of Clinical Pharmacology, CHRU Tours, Tours, 6Dermatology Office, Blanquefort, 7Pediatric Office, Paris, 8Laboratory of Immunology, University Hospital Centre of Reims, Reims, and 9EA 7379 EpiDermE and CIC INSERM 1430, AP-HP, Hospital Henri Mondor, UPEC, Créteil, France
Strategies for diets in chronic spontaneous urticaria (CSU) are controversial. This systematic review assessed the interest in diet for managing CSU. We searched for original reports in MEDLINE, EMBASE, CENTRAL and LILACS. Among the 278 reports screened, 20 were included, involving 1,734 patients. Reports described 3 types of systematic diet: pseudoallergen-free diet (n = 1,555 patients), low-histamine diet (n = 223) and diet without fish products (n = 47), which induced complete remission in 4.8%, 11.7% and 10.6% of patients, respectively, and partial remission in 37.0%, 43.9% and 4.3%. Eight reports described personalized exclusion diets (66 patients) adapted to symptoms/allergological test results and led to complete remission in 74.6% of patients, although the diagnosis of CSU was doubtful. No comparative randomized studies of diets were available. The only randomized studies were based on oral provocation tests with the suspected responsible diet. Population and outcomes were heterogeneous. In conclusion, there is evidence for the benefit of diets in CSU only in individual patients with clinical symptoms. However, the level of evidence is low for the benefit of systematic diets in CSU because systematic double-blind controlled trials of diet are lacking.
Key words: chronic urticaria; spontaneous urticaria; diet; food; allergological tests.
Accepted Aug 7, 2018; Epub ahead of print Aug 7, 2018
Acta Derm Venereol 2019; 99: XX–XX.
Corr: Hélène Cornillier, Department of Dermatology, CHRU Tours – Hospital Trousseau, Avenue de la République, FR-37044, Tours Cedex 9, Tours, France. E-mail: helene.cornillier@etu-univ-tours.fr
Chronic spontaneous urticaria is an inflammatory skin and mucosa disease, defined as the occurrence of spontaneous wheals or oedema for more than 6 weeks. Chronic spontaneous urticaria treatment frequently includes H1-antihistamine drugs as first-line treatment. Strategies for diets are controversial. A systematic review was performed to assess the value of diets in managing chronic spontaneous urticaria. The review shows that the level of scientific evidence is low because controlled studies of diets and of allergological tests in chronic spontaneous urticaria are lacking. However, the data suggest no benefit of systematic diets in chronic spontaneous urticaria, but benefit of personalized diets in individual patients with clinical symptoms.
Chronic urticaria is an inflammatory skin and mucosa dermatitis, defined as the occurrence of spontaneous wheals, angioedema, or both, for more than 6 weeks. The guidelines of the European Academy of Allergy and Clinical Immunology, Global Allergy and Asthma European Network, European Dermatology Forum and World Allergy Organization (EAACI/GA2LEN/EDF/WAO) divide chronic urticaria into 2 groups: chronic inducible urticaria and chronic spontaneous urticaria (CSU) (1). Chronic inducible urticaria includes symptomatic dermographism, cold urticaria, delayed pressure urticaria, solar and heat urticaria, vibratory angiooedema, cholinergic urticaria, contact urticaria and aquagenic urticaria. The causes of CSU are frequently unknown. CSU might occur at any age, but is more frequent in young adults and has a female predominance.
CSU is the consequence of mast cell activation. Activated mast cells release histamine first, then other mediators, such as platelet-activating factor, leukotrienes and prostaglandins that induce sensory nerve activation, vasodilatation, and plasma extravasation. These effects are responsible for dermal oedema, whose clinical features are urticarial characteristic lesions. In CSU, mast cells are pre-activated via an immunological pathway (IgE, IgG, complement) or non-immunological pathway by transmembrane receptors or intracellular signals (2). Complete mast cell activation is triggered by other multiple signals, including infections, drugs, stress, foods and other agents.
Foods might be responsible for urticaria if they are rich in histamine or are able to activate mast cells via the non-immunological pathway and induce histamine release. Foods that might be involved include cheese, fish, vegetables, fruits, chocolate and alcohol (this is a non-exhaustive list). Contrary to acute urticaria being linked to food allergy, the mechanism of CSU is not an IgE-mediated type I reaction, but is rather dose-dependent, usually a delayed pseudoallergic reaction to food colouring, artificial flavouring or preservatives. Non-artificial natural ingredients in food might also cause pseudoallergic reactions. Such reactions have been associated with well-demonstrated changes in gastric permeability (3). CSU is usually considered due to intolerance when clinical manifestations have improved after 3 weeks of strict adherence to a low-pseudoallergen diet, or if provocative testing with food additives aggravates symptoms (4).
CSU treatment frequently includes H1-antihistamine drugs as first-line treatment. According to guidelines, the second-line treatment is increasing the dose of H1-antihistamine by up to 4-fold, then introducing an anti-IgE antibody (omalizumab) or immunosuppressive drugs (1, 5–8). Many other treatments have been reported anecdotally. The European (1), British (9), US (10), Australian and World Allergy Organization guidelines (11) do not recommend diet for managing CSU, but Asian guidelines (12–14) recommend an exclusion diet in specific cases.
This systematic review was performed to assess the value of diets in managing CSU.
We systematically searched for original articles referring to diet in CSU. The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines were followed for reporting.
We included all original reports (randomized control trials (RCTs), observational reports, case series, case reports and items of correspondence) describing the effect of diet in CSU with or without angioedema in children and adults. Reports of acute urticaria, inducible urticaria and urticaria vasculitis were excluded.
In November 2016, an information specialist searched the electronic databases MEDLINE via PubMed (Appendix S1), EMBASE, CENTRAL and LILACS for articles published in common European languages (English, French, Spanish and German) from 1995 to November 2016.
According to the pre-defined criteria, 2 authors (HC, AM) independently selected reports on the basis of the title, then the abstract. Then they examined the full texts of the selected reports. Duplicate publications were identified by several criteria, such as authors, location, title and intervention characteristics. Any discrepancies were resolved by consensus.
For each selected report, 2 authors (HC, AM) independently extracted information on the first author, publication year, journal, country/site, study design, characteristics of patients, type of urticaria, severity and duration of urticaria and comorbidities. Data collected on diet included tests performed before the diet, type and duration of the diet, the efficacy and side-effects, co-interventions and follow-up. We classified diets as systematic when the food elimination was not based on allergological tests and as personalized when the food elimination was based on gastrointestinal symptoms or was specific to positive results of allergological tests before the diet. To evaluate the quality of any RCT reports found, the Risk of Bias tool from the Cochrane Collaboration would be used. Any disagreements were resolved by consensus.
We planned to perform a meta-analysis if combining results of RCTs was possible; otherwise, the analysis was descriptive, reporting data as frequency (%).
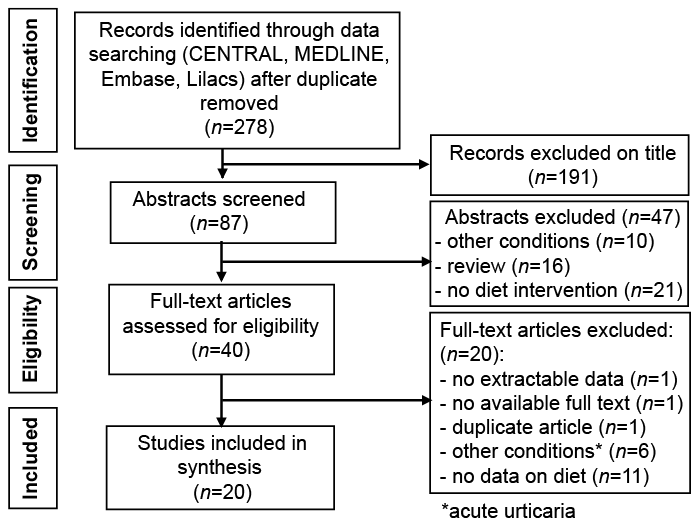
Among 278 publications screened, 20 full-text articles (1,734 patients) were included (15–34) (Fig. 1; Appendix S2 for reasons for excluding full texts). Seven of the 20 articles were case reports and 13 were prospective studies. We found no RCT. Characteristics of included publications are given in Table I.
Fig. 1. Flow of studies in the review.
Table I. Characteristics of studies related to diets in chronic spontaneous urticaria (CSU)
We identified reports of 3 systematic diets (including 1,668 patients) (Appendix S3 for description of diets): pseudoallergen-free diet (PFD; n = 1,555 patients) (15–22), low-histamine diet (LHD; n = 223) (15, 23, 24), and diet without fish products (n = 47) (25, 26); 157 patients were included in studies assessing PFDs and LHDs. Personalized diets involved 66 patients (27–34); 3 followed a gluten-free diet (GFD) for coeliac disease (27–29).
For PFDs (15–22), the median duration of the diet was 3 weeks (range 3–5 weeks); 74 patients (4.8%) showed complete remission (CR) and 575 (37.0%) partial remission (PR) at the end of the diet. Pseudoallergens were reintroduced in 1,171 patients, and recurrence was observed in 240 (20.5%). CR and PR were assessed by urticarial activity scores for all patients (UAS7 in 191 patients, UAS4 in 978, urticarial score in 386). For 153 patients, PR was further defined by reduced corticosteroid intake and improved quality of life. For 872 patients, H1-antihistamines were allowed if needed, in addition to diet, and for 244, H1-antihistamines and steroids were allowed. For 237 patients, diet was used as monotherapy, and co-interventions were not mentioned for 202.
For LHDs (15, 23, 24), the median duration of the diet was 3 weeks and led to CR in 26 patients (11.7%) and PR in 98 (43.9%). Remission was also defined by reduced urticarial activity score (UAS7 in 157 patients, UAS4 in 56, urticarial score in 10). Histamine triggers were reintroduced in 157 patients independent of the response to the diet, and CSU recurred in 66 (42.0%). H1-antihistamines were permitted in 273 patients, and 10 patients exclusively followed a diet.
Overall, 47 patients had a diet without fish products (25, 26), 25 with sensitization to Anisakis simplex after an allergological test, without clinical history of food allergy. The duration of the diet ranged from 3 to 16 months and led to CR in 5 patients (10.6%) and PR in 2 (4.3%). Fish products were reintroduced in 6 patients and induced CSU recurrence in one patient.
For systematic diets, 82/1,671 patients (4.9%) showed CR after the diet and 626 showed PR (37.5%). Overall, 16 publications gave no data on observance of diets (15, 16, 18–22, 24, 25, 27–31, 33, 34). In 4 publications, the number lost to follow-up was 103 of 241 patients.
In the 8 publications (66 patients) evaluating personalized diets (27–34), 50 (75.7%) patients showed CR after the diet: 54 had reintroduction of specific allergens, which led to CSU recurrence in 12 (22.2%).
In 16 publications (17, 19–22, 24–34), allergological tests were performed before the diet. These were always performed for personalized diets and were inconsistently performed for systematic diets. Allergological tests consisted of skin prick tests (SPTs), specific IgE testing, or both, and diets were introduced in patients with positive allergological test results in 8 publications (25, 26, 29, 30–34), patients with negative test results in 6 publications (19, 21, 22, 24, 27, 28) and all patients in 2 publications (17, 20). In patients with PFDs and negative allergological test results, 2.7% showed CR at the end of the diet and 39.4% showed PR; 20.7% experienced recurrence after reintroduction. Data were not extractable for patients with positive allergological test results. For LHDs, in one publication (33), 10 patients had a negative SPT result, with no knowledge of clinical history of food allergy: 3 patients showed CR and 7 PR at the end of the LHD. For specific cases of GFD, no history of food allergy was reported in the 3 publications (27–29), but all 3 patients had coeliac disease: 2 patients with negative SPT results to food allergens showed CR at the end of the GFD, with no reintroduction. One patient with a positive SPT result to gliadin showed CR after its elimination, but recurrence of urticarial symptoms after the reintroduction of gluten. For other personalized diets, 32.3% of patients had a history of food allergy; 17.9% had a positive allergological test result. CR was achieved in 100% with a negative SPT result and 75% with a positive SPT result, with 33% recurrence after reintroduction. The data are shown in Table II.
Table II. Data on allergological tests and reintroduction of allergens in included studies
This systematic review of 20 publications related to treating CSU with diet found that, among the 1,734 patients with CSU, 1,668 had a systematic diet and 66 a personalized diet. Systematic diets led to CR in 4.9% of patients and PR in 37.5%. Personalized diets led to a CR rate of 74.6%. Systematic diets consisted of 3 types: PFD (4.8% CR and 37.0% PR), LHD (11.7% CR, 43.9% PR), and diet without fish products (10.6% CR, 4.3% PR). In most studies, the diet could be combined with other drugs, and no study compared the diet with a control arm.
Regarding pseudoallergens, hypersensitivity, a suggested cause of CSU (4, 22), is a non-immunological reaction. The clinical history is not sufficient to diagnose hypersensitivity to pseudoallergens, and these cases account for only 1–3% of cases of CSU (19). As a diagnostic help, a therapeutic test by a pseudoallergen-free diet for 3 weeks can be followed by patients with daily or almost daily CSU. In our review, the rate of CR after 3 weeks was low overall (4.8%), but criteria to define CR or PR were not standardized. Moreover, inclusion criteria were limited to non-inducible CSU, without distinction of severity or duration of symptoms, which are important known negative prognostic factors. In CSU, natural remission is estimated to occur in 32% of patients at 3 years, 34% at 5 years and 49% at 10 years (35, 36). Remission rate of patients receiving H1-antihistamines in studies included in the meta-analysis from the Cochrane Collaboration ranged from approximately 10% to 85% depending on the drug used, posology and time when remission was assessed (4). With no control arm reported for the studies and with missing data on CSU duration and severity, it is difficult to analyse the remission rate linked to the diet. Because of the absence of a regular measurement of outcome during and after the diet period, as well as the lack of follow-up in most reports, we cannot evaluate an optimal diet duration and its effectiveness in the short- and long-term. In addition, the use of antihistamines, if needed, was permitted in some studies and not in others and obviously interferes with regime efficiency data.
Assessing the efficiency of an LHD is difficult because of too few patients and because some followed both a LHD and PFD. Histamine intolerance has been suggested as a cause of CSU, with some patients reporting exacerbation with histamine-rich foods. Siebenhaar et al. (15) showed that patients with CSU may or may not benefit from avoiding histamine in their diet, but this benefit cannot be predicted from patients’ previous experience of tolerating or not histamine-rich foods. In most patients with response, determining whether the response is due to the absence of histamine in these diets, the natural evolution of CSU or avoidance of pseudoallergens is difficult. Currently, we have few studies of one group following an LHD and another a PFD. The updated guidelines on urticaria of the EAACI/GA2LEN/EDF/WAO do not recommend a PFD or LHD because such diets are controversial and are as yet untested in well-designed double-blind placebo-controlled studies (1). They recommend more research on the effect of natural and artificial ingredients of food in causing urticaria.
Although no data on observance were reported, PFD and LHD seem to be complicated to follow in everyday life because many common foods are excluded. In the long-term, the diets would be unhealthy, with a risk of malnutrition, but data on safety with a long follow-up are lacking. Moreover, we do not know whether a PFD or LHD improves global quality of life even with disease remission.
Conflicting data exist on the association of sensitization to the fish parasite A. simplex and CSU (37–40). Two studies of 47 patients with CSU who followed a diet without fish products yielded contradictory results. This diet is simple to follow, but excludes the dietary benefits of fish, particularly for patients with hyperlipidaemia.
The personalized diets are simpler to follow than broad-spectrum diets, such as an LHD or PFD, but the diet is recommended case by case. This research can be guided by interrogation during the clinical examination. If the clinical story is in favour of the allergies, allergological tests, such as SPT, serum-specific IgE testing or oral food challenge, can be performed (41). However, these chronic urticarias should not be classified as CSU. Other personalized diets apply to only specific cases. A GFD is mandatory for coeliac disease. It was effective for treating CSU associated with coeliac disease in the 3 case reports we found. An increased permeability of intestinal mucosa may facilitate the absorption of antigens, which may induce urticarial symptoms via the formation of circulating immune complexes. Pathophysiological data are controversial (27, 42–44).
The main limitation of this study is that we found no RCT of diets and no study comparing diets. Hence, the level of evidence is low. Secondly, because of the heterogeneity of durations of diets, mode of outcomes and comorbidities, comparison of included populations was difficult. We also found high heterogeneity regarding allergological tests. Moreover, in most studies, H1-antihistamines were allowed in patients on a diet, which interferes with diet efficiency data. Thirdly, diets do not take into account the dietary habits and regional differences in food, which may affect the success rate. Fourthly, data for long-term efficacy are missing because of lack of long-term follow-up or missing data. Fifthly, the review included only reports of studies published since 1995; previous articles were not included. Finally, it is questionable whether patients undergoing personalized diets had genuine CSU.
There is evidence for the benefit of diets in CSU only in individual patients with clinical symptoms, but the level of evidence is low for the benefit of systematic diets in CSU, because systematic double-blind controlled trials of diet are missing. In our daily practice, we recommend asking patients if they can identify specific food allergens in their diet. If so, we recommend a personalized diet omitting these identified food allergens. If not, we do not recommend any diet. Further research in terms of RCTs of systematic diets is needed, taking into account biases linked to drug co-interventions and assessing observance to the diet.
The authors are indebted to Mrs Gaelle Fanelli, information documentalist from HAS, France, for her technical help. We thank all members of Centre de Preuves en Dermatologie, France: Dr Sébastien Barbarot, Pr Marie Beylot-Barry, Dr Guillaume Chaby, Dr Florence Corgibet, Pr Bernard Guillot, Pr Pascal Joly, Pr Denis Jullien, Dr Ève Pepin, Dr Jean-Luc Riboulet, Dr Émilie Sbidian, Dr Jean-François Sei, Dr Patricia Senet, and Pr Manuelle Viguier.
Funding sources: This work was supported by Centre de Preuves en Dermatologie, France
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize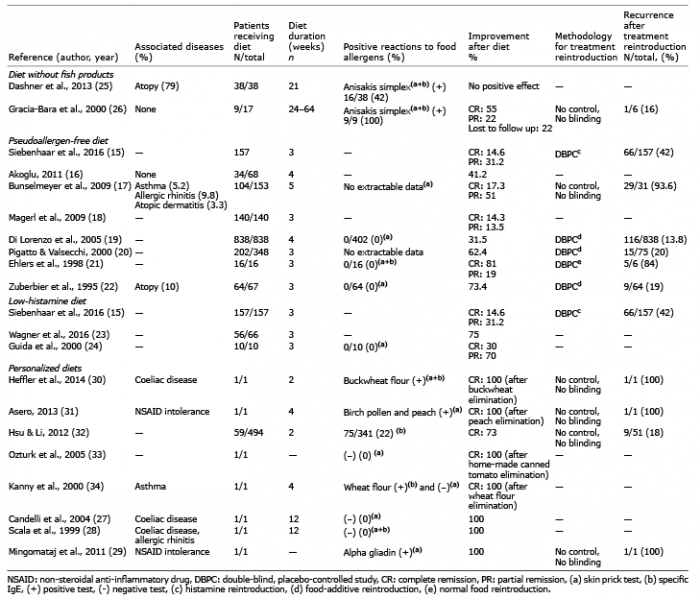 Click to show fullsize
Click to show fullsize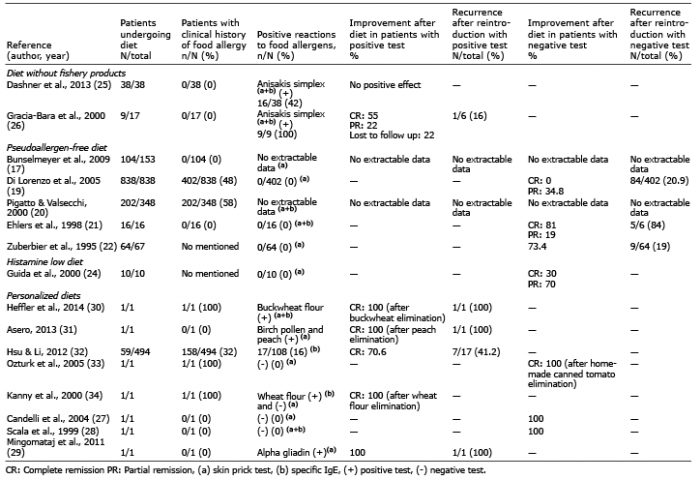 Click to show fullsize
Click to show fullsize