


1Department of Clinical Epidemiology and Applied Biostatistics, 3Institute for Medical Virology, University Hospital Tübingen, Tübingen, Germany, 2Skin Cancer Research Unit, College of Public Health, Medical & Veterinary Sciences, James Cook University, Townsville, Queensland, Australia, and 4Division of Dermato-Oncology, Department of Dermatology, University of Tübingen, Tübingen, Germany
Keratinocyte cancer is the most common malignancy in Caucasians. The aim of this study was to investigate risk-factors responsible for development of keratinocyte cancer in Australia. A case-control study was conducted, including 112 cases of squamous cell carcinoma (SCC), 95 cases of basal cell carcinoma (BCC) and 122 controls. Freckling during adolescence (SCC: odds ratio (OR) 1.04, p < 0.01; BCC: OR 1.05, p < 0.01), propensity to sunburn (SCC: OR 2.75, p = 0.01, BCC: OR 2.68 p = 0.01) and high cumulative sun-exposure (SCC: OR 2.43, p = 0.04; BCC: OR 2.36 p = 0.04) were independent risk-factors for both SCC and BCC. This study provides further evidence that a sun-sensitive phenotype and excessive sun-exposure during adulthood contribute to the risk of developing keratinocyte cancer. Wearing a hat, long-sleeved shirts, and sunscreen did not significantly reduce the risk of keratinocyte cancer in this study.
Key words: risk factor; keratinocyte cancer; sunlight; sunscreen; basal cell cancer; squamous cell cancer.
Accepted Dec 13, 2018; E-published Dec 13, 2018
Acta Derm Venereol 2019; 99: XX–XX.
Corr: Lina-Maria Serna-Higuita, Department of Clinical Epidemiology and Applied Biostatistics, University Hospital Tübingen, Silcherstraße 5, DE-72076 Tübingen, Germany, and Thomas Iftner, Institute of Medical Virology, University Hospital Tübingen, Elfriede-Aulhorn Str. 6, DE-72076 Tübingen, Germany. E-mails: Lina.Serna-Higuita@med.uni-tuebingen.de; thomas.iftner@med.uni-tuebingen.de
This study examined the complex interplay between environmental and host risk-factors for keratinocyte cancer. The results show that increasing age, lower academic qualifications, freckling during adolescence, solar lentiginous, propensity to sunburn and high-cumulative sun-exposure increase the risk of keratinocyte cancer.
Keratinocyte cancer (KC) arises from the malignant transformation of squamous epithelial cells comprising the epidermis (1). KC includes basal cell carcinoma (BCC) and squamous cell carcinoma (SCC) (1, 2). Al-though KC rarely causes death (3), surgical excision can cause significant morbidity, especially on highly-visible areas, such as the face, ears and neck (4).
KC is the most common malignancy in Caucasians (2, 5). The incidence of KC has increased worldwide by 3–8% annually (6, 7). Australia has the highest reported incidence of KC (8, 9), with the most extreme incidence rates recorded in North Queensland (10, 11). A population-based study conducted in Townsville between 1996 and 1997 found that the age-standardized incidence rates per 100,000 inhabitants for BCC were 2,058.3 for men and 1,194.5 for women, and for SCC were 1,075.7 for men and 517.7 for women (10, 11).
The increasing incidence of KC may be explained mainly by high levels of sun-exposure (7) despite the implementation of campaigns in Australia to induce a behaviour change in favour of sun protection and reduce sun exposure (12–14). However, the complex interplay between sociodemographic and environmental risk-factors and the uptake of the various forms of photoprotection is not fully understood.
Exposure to solar ultraviolet radiation (UVR) is a well-established risk-factor for KC (15). Several studies have found modifiable risk-factors for KC other than UVR (16); including diet (17), alcohol consumption (17), cigarette smoking (18–20), and infection with human papilloma virus (21). However, the individual contribution of each factor is not clear, and data on interactions between sun-exposure, host-factors and other potential risk-factors for KC are limited (22), and may explain some inconsistencies in the published literature (2).
The identification of modifiable risk-factors for KC may lead to more effective preventive strategies to reduce the incidence of KC, particularly in high-risk populations. The present study was designed to elucidate the relationship between environmental and host risk-factors in Caucasian patients from Australia who develop KC.
Eligible cases (n = 442) in this case-control study consisted of adults (18–76 years) from the population of Townsville (latitude 19.3°S), North Queensland, who had an incident of BCC or SCC during 2004 to 2009. Cases were patients who presented for treatment at the Townsville Hospital or the surgeries of local surgeons, a dermatologist and general practitioners in Townsville. Only patients with histological diagnosis of in situ or invasive SCC or BCC of at least 5 mm diameter on the body or 10 mm diameter or more on the head or neck, were included. Cases were compared with age-matched (±5 years) control subjects recruited from local community groups, service clubs and the neighbours of cases. The community-based controls were residents of Townsville with no self-reported history of skin cancer.
Exclusion criteria comprised: skin types V–VI (23), HIV seropositivity, xeroderma pigmentosum, generalized severe dermatological disease, basal cell naevus syndrome, familial atypical multiple mole-melanoma syndrome, transplant recipients, history of SCC or BCC (for controls), initial excision (for cases), and cytotoxic or immunosuppressive therapy within 12 weeks of recruitment. Subjects were also excluded if they had received any of the following treatments within 4 weeks of recruitment: oral corticosteroids on a regular daily basis; inhaled corticosteroids (beclomethasone ≥ 1,200 µg/day, fluticasone ≥ 600 µg/day, or budesonide ≥ 800 µg/day) and regular use of topical steroids to > 20% of the skin surface.
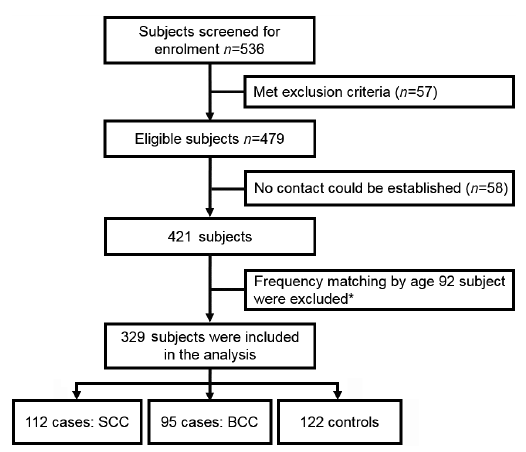
A total of 115 subjects (cases and controls) were ineligible based on the exclusion criteria or could not be contacted, leaving 421 subjects. A further 92 subjects were excluded due to frequency matching (see age matching below), leaving a final total of 329 subjects in the analysis (Fig. 1).
Fig. 1. Flowchart of study participants. BCC: basal cell carcinoma; SCC: squamous cell carcinoma. *Age-matching process is explained in detail in the data analysis section.
All cases and controls who fulfilled the eligibility criteria and provided written informed consent to participate were assessed at the Skin Cancer Research Unit clinic. Clinical evaluation was identical for cases and controls: a doctor conducted a full-body skin examination (excluding buttocks and genitals); the research nurse (MG) recorded phenotypic characteristics including natural hair colour at age 18 years (ascertained using wig samples) (24); skin colour, distribution and extent of freckling on the face, forearms and shoulders of participants during adolescence (participants were shown a freckling chart as in previous studies by the investigators) (24) and distribution of solar lentigines on the shoulders (24).
All participants also completed a self-administered questionnaire at baseline to elicit basic demographic information; daily sun-exposure habits for 5 age intervals (school years to age 17; 18–19 years; 20–29 years and 30–59 years); propensity to sunburn; tanning ability and number of blistering sunburns. Duration of sun-exposure experienced on a typical weekday and weekend was recoded as: <1, 1–4, > 4–6 and > 6 h/day. To measure cumulative sunlight exposure, the following mid-point values were applied to each category for duration of sun-exposure (< 1 h = 0.5; 1–4 h = 2.5; 4–6 h = 5; > 6 h = 8) on a weekday and weekend. The mid-point values for weekday and weekend sunlight exposure were first summed for each age-period group, then summed across age groups, and finally divided into 3 categories: low, medium, and high (25). Frequency of use (always/usually/sometimes/rarely/never) was documented separately for 3 forms of photoprotection (wearing a hat/long-sleeved shirt/sunscreen) during 5 age intervals, then dichotomized as “frequent” (always/usually) or “rare” (sometimes/rarely/ never). Participants who frequently used at least 2 of the 3 forms of photoprotection were considered “frequent multimodal sun-protection users” (26). Highest academic qualification was recoded as: (i) primary and secondary school, and (ii) trade certificate or technical/college or university degree.
Documentation included history of: immunosuppressive conditions, medications, warts, and internal cancers. Lifestyle factors included: smoking, alcohol consumption and dietary intake (typical daily consumption of: bread, cereal, rice and pasta; vegetables and legumes; fruit; milk and dairy products; meat; fish; eggs; nuts; and fluids).
The presence of a KC was histologically-confirmed by obtaining a biopsy of the lesion. Patients who had a single BCC excised were assigned as BCC-cases, whilst patients who had a single SCC excised were considered SCC-cases. Patients with histologically-confirmed BCCs and SCCs excised on the same day were also assigned to the SCC-case group. All slides were reviewed by a specialist in the histopathology of the skin (CG) to ensure that the reported histological diagnosis was accurate.
Ethics approval for this case-control study was granted by the Townsville Health Service District Institutional Ethics Committee (protocol 06/02) and the Human Research Ethics Committee of James Cook University (Approval H2070). All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
All participants provided written informed consent prior to data collection. Information collected from participants and their medical records were treated as strictly confidential.
Because the mean ± standard deviation (SD) age of cases (60.6 ± 11.4 years) and controls (55.06 ± 11.4 years) was different, frequency matching by age was performed on the original dataset. All cases and controls aged 44–58 years were included in the study. In addition, all cases, but only a random sample of controls younger than 44 years, as well as all controls, but only a random sample of cases older than 58 years, were retained in the final sample of 329 participants (Fig. 1).
This project was based on data collected to investigate the effects of environmental factors and human papillomavirus infections on the development of KC. The present analysis was performed on a fixed sample size of 329 participants. Power was assessed ex-post based on the risk of KC according to sun-exposure assuming the effect observed by Iannacone et al. (25). Using the software nQuery, the sample size of 112 cases of SCC and 122 controls had a power of 90% for detecting an absolute difference of 22% (25) in sun-exposure between cases and controls, assuming a type I error of 0.05 (2-sided).
Categorical variables were described using frequencies and proportions; numerical variables were reported as either means ± SD or medians and interquartile range (IQR), depending on the distribution of the data. Normality of the distribution was assessed by investigating kurtosis, skewness as well as Q-Q plots. Bivariate analyses for both types of KC were performed using χ2 tests or Fisher’s exact test as appropriate. Independent-samples t-tests were used to compare numerical variables that were approximately normally distributed, while Mann–Whitney tests were used to evaluate skewed variables.
Binary logistic regression was performed to assess associations between KC status and potential risk-factors. Candidate risk-factors for the multivariate model were selected based on clinical reasoning and statistically significant results in bivariate analyses. Backward selection was used to sequentially remove variables from the model. Crude (simple regression model) and adjusted (multiple regression model) odds-ratios (OR) and 95% confidence intervals (CI) were calculated.
Additional changes in the frequency of sun-exposure and the use of sun-protection across different age intervals were examined. These trends were analysed using the Cochran’s Q test. All statistical tests were 2-tailed, and the significance level was set at p ≤0.05. All statistical analyses were performed using IBM SPSS® software, version 23.0 (Armonk, NY: IBM Corp.).
Missing data were assumed to be at random (27) and multiple imputation was used to replace lost data with plausible values, based on the observed data.
Ethics approval for this case-control study was granted by the Townsville Health Service District Institutional Ethics Committee (protocol 06/02) and the Human Research Ethics Committee of James Cook University (Approval H2070). All participants provided written informed consent prior to data collection. Information collected from participants and their medical records were treated as strictly confidential.
This study included 207 (62.9%) cases (95 BCC-cases and 112 SCC-cases) and 122 (37.1%) controls. Age ranged from 27 to 76 years (mean 57 ± 0.5 years) and 53.2% of the sample was male. The demographic, pigmentary and sun-exposure characteristics of participants by case-control status are shown in Table I. Compared with controls, both BCC- and SCC-cases were significantly less educated and less likely to develop a tan post-sun-exposure; while being more likely to have light eyes, light colour hair, lentigines, a propensity to sunburn and more freckling on their face.
Table I. Demographic, lifestyle, pigmentary and sun-exposure characteristics of the study population by case-control status (n = 329)
Using the results from the bivariate analysis, a logistic regression model was generated, which found a significant association between SCC and lower academic qualifications, the presence of freckling, and solar lentigines, propensity to sunburn and a high number of accumulated hours of sunlight exposure. This model explained 39% of the variance in SCC-cases and was a good fit to the actual data (HL χ2 = 9.31 p = 0.32 df = 8) (Table II). In addition, a significant association was found between BCC and lower propensity to sunburn, the presence of freckling, and a high and medium number of accumulated hours of sun-exposure (Nagelkerkes R2: 0.315; HL χ2 = 5.93 p = 0.65 df = 8) (Table II).
Table II. Binary logistic regression analysis of risk factors for keratinocyte cancer (n = 329)
The proportion of cases and controls who spent more than 4 h/day in the sun decreased with age (Control, BCC and SCC PQ Cochran < 0.001; Fig. 2), while frequent-use of multimodal sun-protection (2 of following: wearing a hat/long-sleeved shirt/sunscreen) increased with age in both groups (Control, BCC and SCC PQ Cochran < 0.001; Fig. 3). Sun-exposure of 4+ h/day from 30 to 59 years of age was an independent predictor of BCC and SCC (Fig. 2). More cases than controls used multimodal sun-protection, without conferring any protective benefit against BCC and SCC (Fig. 3). None of the 3 forms of sun-protection (wearing a hat, long-sleeved shirt, and use of sunscreen) by periods-age (period 1: school years to age 17 years; period 2: 18–19 years; period 3: 20–29 years and period 4: 30–59 years) reduced the odds of SCC or BCC, even after adjustment. Conversely, wearing a hat for more than 3 periods was statistically significant related to the risk of SCC (Table III). Similarly, long-term use of sun-protection (2–4 age-intervals) did not reduce the likelihood of KC (Table III); since patients with a history of skin cancer may have different behaviour with respect to sun protection measures, analyses were also performed omitting information on sun protection after the first skin cancer, however, with the exception of wearing a hat for more than 3 periods, which lost statistical significance, the other results were similar to those of the full cohort (Table SI and Fig. S1). Sunscreen was the least utilized form of sun-protection. Use of all 3 forms of sun-protection increased from 1980 onwards (Fig. 4).
Fig. 2. Duration of sun-exposure for cases and controls shown by age intervals (n = 329). Sun-exposure greater than 4 h per day during summer or holidays shown by age intervals. OR: odds ratio; CI: confidence interval. 1Adjusted for sex, academic qualification, freckling during adolescence, solar lentigines on the shoulders, propensity to sunburn and accumulated hours of sun exposure. 2Adjusted for sex, freckling during adolescence, propensity to sunburn and accumulated hours of sun exposure. *Schooling generally begins at age 5 years and finishes at age 17 years in Queensland, Australia.
Fig. 3. Frequent use of multimodal sun-protection by cases and controls, shown by age intervals (n = 329). OR: odds ratio; CI: confidence interval. *Use of at least 2 of the 3 sun-protection measures (wearing a hat, long-sleeved shirt or sunscreen). **Schooling generally begins at age 5 years and finishes at age 17 years in Queensland, Australia. 1Adjusted for sex, academic qualification, freckling during adolescence, solar lentigines on the shoulders, propensity to sunburn and accumulated hours of sun exposure. 2Adjusted for sex, freckling during adolescence, propensity to sunburn and accumulated hours of sun exposure.
Table III. Bivariate and multivariate analyses of the influence of sun-protection methods on the risk of developing keratinocyte cancer (n = 329)
Fig. 4. Proportion of participants who usually/always use sun-protection*, shown by chronological time (n = 329). *Use of sun-protection measures by chronological time (wear a hat, long-sleeved shirt or sunscreen). Note that younger participants only contribute data to later time-intervals, whereas older participants contribute data across all time-intervals. Thus a potential bias due to cohort effects or attrition cannot be excluded.
History of internal cancers, and dietary intake were similar for both groups (data not shown) and previous autoimmune therapy was not significantly associated with BCC or SCC. No dose-response was evident for number of cigarettes smoked or the duration of smoking and the risk of KC even after adjustment. Likewise, there was also no association between higher alcohol consumption and the risk of SCC or BCC (Table IV). No difference in SCC or BCC risk was evident for the different types of alcohol consumed (e.g. beer/sherry/spirits) (data not shown). Although fewer SCC-cases than controls drank wine/champagne (SCC vs. Control 30.4% vs. 52.5%), the risk of KC was not significantly reduced (adjusted-OR 0.68; 95% CI 0.33–1.41, p = 0.31).
Table IV. Univariate and multivariate analyses of smoking and drinking status in relation to SCC risk (n = 329)
This case-control study found that a high propensity to sunburn increases the risk of KC, and high levels of cumulative sunlight exposure doubled the risk of developing KC compared with those who have low levels of cumulative sunlight exposure. In addition, lower academic qualifications, extent of freckling during adolescence, the presence of solar lentigines on the shoulders during adulthood, and propensity to sunburn were also independent risk-factors for the development of SCC and BCC.
These findings suggest that pigmentary characteristics indicative of a sun-sensitive phenotype and sun-exposure accumulated during adulthood (regardless of childhood sun-exposure) are important in the development of KC (28–31), suggesting that reducing sun-exposure during adulthood can help prevent KC. These findings are similar to those from a cohort-study of 56,667 women, which showed that sun-exposure during adulthood increased the risk of KC irrespective of childhood UVR-exposure (32), but differ from the case-control study by Iannacone and co-workers, which showed that childhood sun-exposure increased the risk of SCC, but not of BCC (25). Given these conflicting findings, it seems important to clarify whether there are vulnerable periods in life during which sun-exposure is more harmful.
Since sun-exposure represents the most important environmental risk-factor for KC (20) several approaches have been established to reduce exposure, including avoiding direct midday sun-exposure, wearing sun-protective clothing, and applying high sun-protection-factor (SPF) sunscreen (30, 33). Frequent sunscreen-use did not appear to reduce the risk of KC in the present study. This is consistent with a randomized controlled trial that did not show any significant difference in the incidence of KC between “daily sunscreen” and the “no sunscreen” group (34, 35). One plausible explanation is that sunscreen-users stay outdoors longer, merely delaying sunburn (or accumulating a high sub-erythemal dose) rather than preventing over-exposure (36–38). Furthermore, the effectiveness of sunscreen depends on its SPF, the amount applied, application frequency, and the user’s skin-phototype (36, 39–41). Some authors have proposed that other physical barriers, such as wearing a hat and long-sleeve shirt, can also help in preventing the harmful effects of UV radiation (35); in the present study, wearing a hat was associated with a significantly elevated risk for SCC. North Queensland is a region with very high insolation, and there is a high frequency of individuals using sun protective measures. This may be the reason for lack of risk reduction by sun-protective practices in our study. Similar findings have been reported previously by others (42).
In order to achieve comprehensive sun protection and reduce the risk of skin cancer, it is necessary to take daily measures to protect oneself from excessive exposure to solar UV-radiation (43). The American Skin Cancer Society (2017) recommends the following primary strategies: (i) seek shade when out in the sun, especially in the middle of the day when UV radiation is strongest (10.00–16.00 h); (ii) textile protection with appropriate clothing (i.e. long-sleeved shirts and long trousers or long skirts) (30, 41); (iii) use wide-brimmed hats; (iv) use sunscreen with the correct sun protection factor for the skin phototype (individuals with skin phototype I need SPF 50+ protection and those with darker skin phototypes can use SPF 15 products) (41). In addition, the sunscreen should be re-applied after each bath and every 2–3 h during a stay on the beach; and (v) avoid the use of tanning beds (44). Other recommended strategies for the prevention of skin cancer would be to reduce the sun-exposure time and outdoor activity during periods of high UV radiation (33, 39), wear sunglasses, parasols and, finally, regular skin self-examination or clinical examination, which enables early detection of skin changes (30). The combination of these approaches has been shown to reduce the burden and reduce the incidence, morbidity and mortality of skin cancer (45, 46).
This study found that a substantial proportion of cases and controls exhibited several risk-behaviours, including spending more than 4 h/day outdoors, and infrequent use of sunscreen, shirts and hats; even though the prevalence of all 3 behaviours increased significantly between 1970 and 2010. The latter is probably a consequence of the mass media campaigns introduced in Australia from 1980 onwards to raise awareness about skin cancer and sun-protection (12, 37). These findings highlight the importance of public health campaigns in encouraging life-long use of sun-protection and promoting regular skin checks (12, 47).
KCs are known to be associated with states of immune perturbation (29, 32, 48, 49). In contrast, we found that cases and controls were similar in relation to use of immunosuppressive therapy. However, as we excluded patients who received immunosuppressive therapy close to the time of diagnosis of KC, the current study was not designed to answer this question.
The present study has several limitations. Firstly, little data were collected concerning the pattern of sun-exposure (i.e. at midday vs. mornings or late afternoons). Secondly, sun-exposure habits were self-reported. Recall bias is possible, given that case subjects are more likely to be concerned about possible causes of KC, and therefore are more likely to over-estimate their sun-exposure history than controls; and thirdly the size restriction on the keratinocyte cancer included could also may lead a selection bias.
One strength of this study is the availability of data on a large number of potential risk-factors, allowing adjustment of confounding factors. Another strength is that controls were screened for evidence of BCC and SCC by a medical expert to avoid the misclassification of cases and control subjects that might otherwise result from self-reported data. Longitudinal data collected from this cohort may further elucidate the contribution of host and environmental risk-factors to the development of KC.
These findings confirm the increased risk of KC in association with sun-exposure, consistent with other studies. Importantly, this study showed that the frequency of use of sun-protection did not differ significantly between cases and controls. Further investigations are needed focusing on these variables, together with individual susceptibility factors and other potential interacting risk-factors for KC to determine which sun-protection strategies are most effective in preventing KC.
The authors wish to thank Cindy McCutchan for her assistance with data collection and entry, Jana Bender for designing the relational database and the following doctors and research nurses for their assistance examining the study participants: Dr Pamela Caleo; Dr Kerry Kelly; Dr Alexander Kippin; Dr Carl Lisec; Dr Janet Langren; Dr Tania Zappala and RNs, Margaret Clough; Mary Horsford; Irene Raws; and Julie Twomey.
This study was funded by The Cancer Council Queensland, The Parkes Bequest to James Cook University and The Townsville Hospital Foundation. Dr Harrison also received salary support from the Cancer Council Queensland’s “John McCaffrey Fellowship for Cancer Control in North Queensland”.
We acknowledge support by Deutsche Forschungsgemeinschaft and Open Access Publishing Fund of University of Tübingen.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize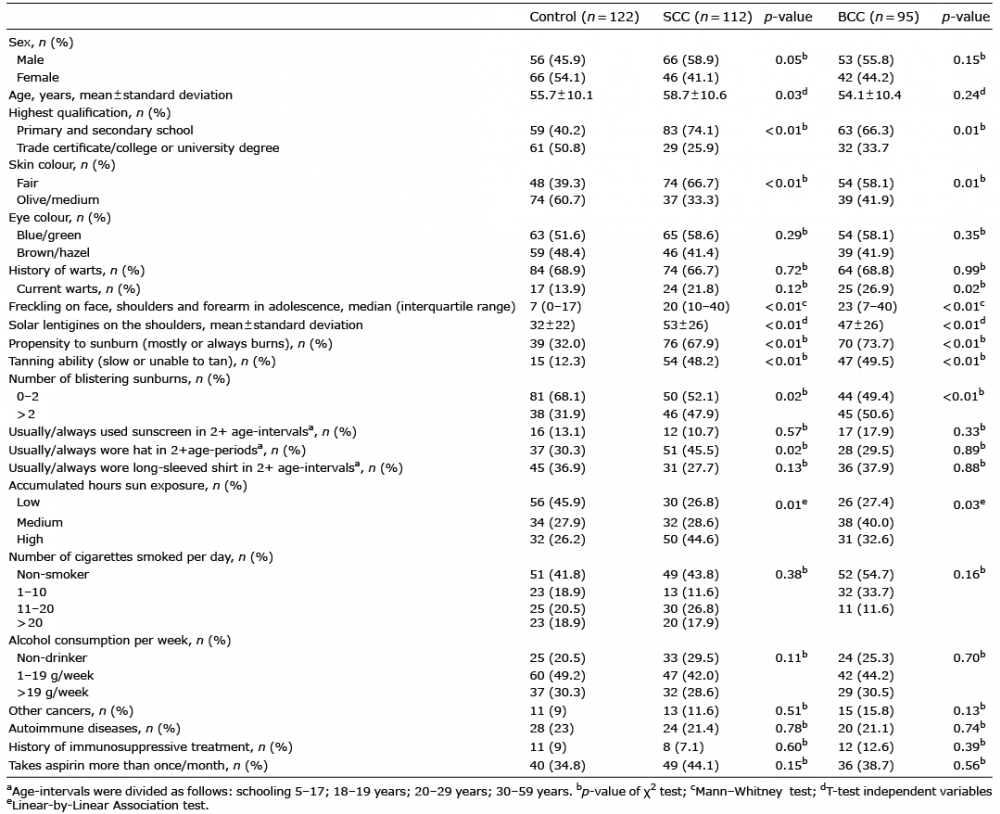 Click to show fullsize
Click to show fullsize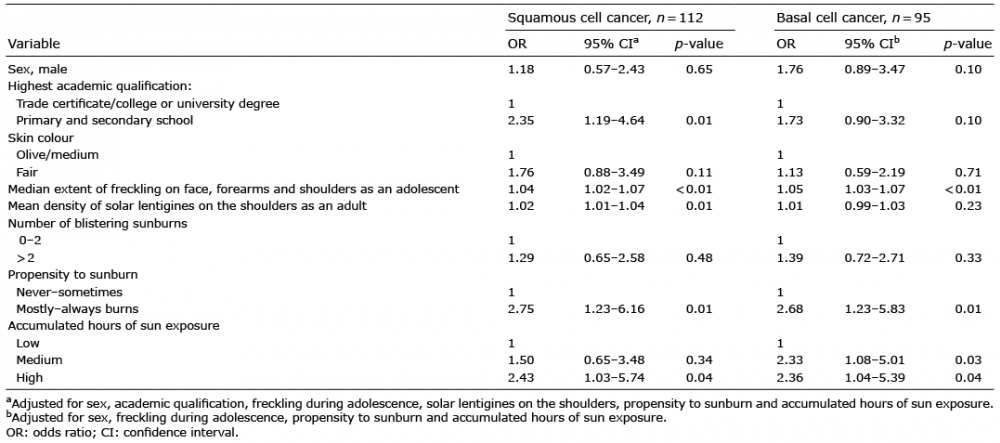 Click to show fullsize
Click to show fullsize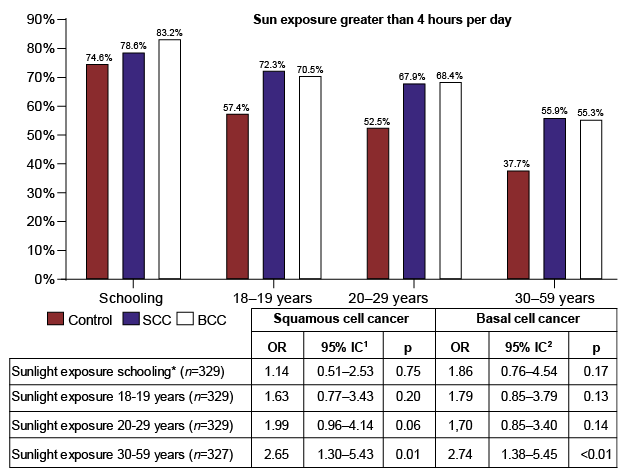 Click to show fullsize
Click to show fullsize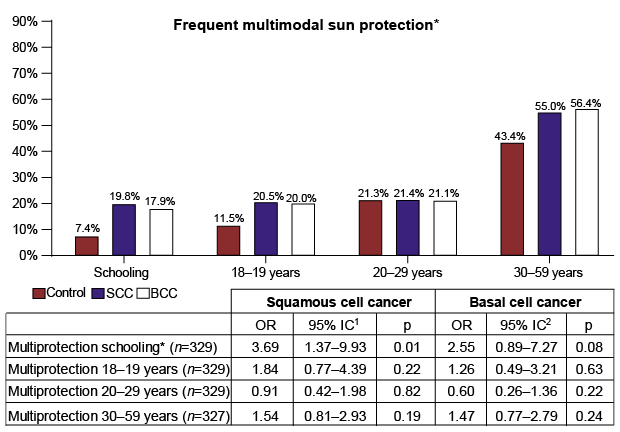 Click to show fullsize
Click to show fullsize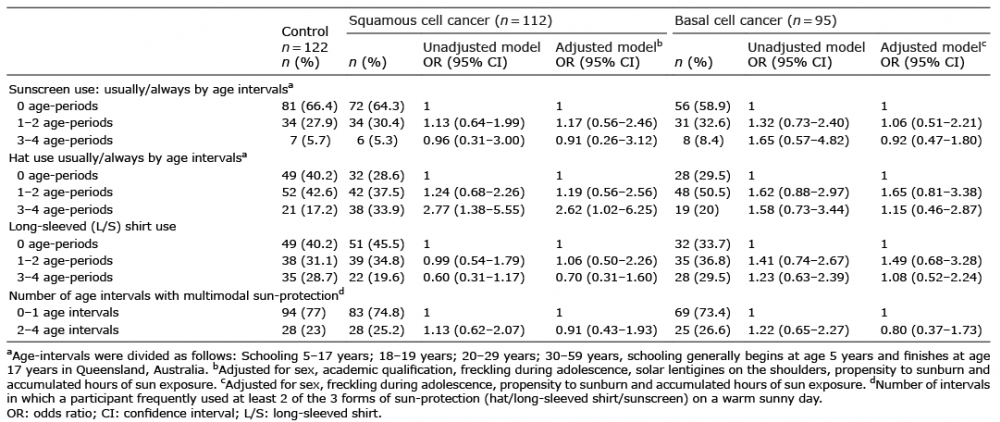 Click to show fullsize
Click to show fullsize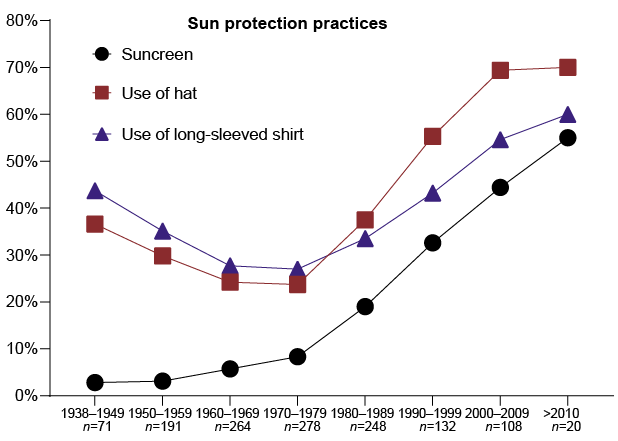 Click to show fullsize
Click to show fullsize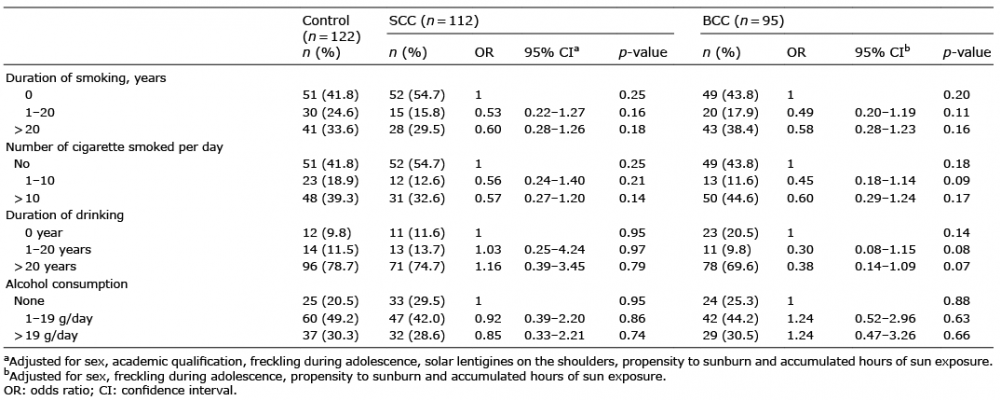 Click to show fullsize
Click to show fullsize