


1Department of Dermatology and Allergology and 5Department of Plastic Surgery, Tampere University Hospital and Faculty of Medicine and Life Sciences, University of Tampere, Tampere, 2Department of Dermatology, Skin Cancer Unit, Helsinki University Central Hospital, Helsinki, 3Research, Development and Innovation Center, Tampere University Hospital and Health Sciences, Faculty of Social Sciences, Tampere University, and 4Department of Pathology, University of Tampere and Fimlab Laboratories, Tampere, Finland
The incidence of cutaneous squamous cell carcinoma is increasing worldwide. In most epidemiological studies, only the first case of cutaneous squamous cell carcinoma is registered, underestimating the burden of the disease. To determine the frequency and detailed characteristics of cutaneous squamous cell carcinoma in a Finnish patient cohort, we performed a retrospective 10-year study taking into account multiple tumours in one patient. On the pathology database search and medical record review we identified 774 patients with a total of 1,131 cutaneous squamous cell carcinomas. The crude incidence increased from 18.6/100,000 persons in 2006 to 28.1 in 2015. The location of tumours differed between men and women: the greatest difference concerned cutaneous squamous cell carcinoma of the ear, with 93% of cases occurring in men. One fourth (24%) of patients had more than one tumour. A small shift from poorly to well-differentiated tumours was seen. In conclusion, the incidence of cutaneous squamous cell carcinoma increased, with many patients presenting with multiple tumours.
Key words: squamous cell carcinoma; keratinocyte carcinoma; non melanoma skin cancer; incidence; histopathology.
Accepted Jan 7, 2019; E-published Jan 9, 2019
Acta Derm Venereol
Corr: Niina Korhonen, Department of Dermatology and Allergology, Tampere University Hospital, Teiskontie 35, FIN-33521 Tampere, Finland. E-mail: niina.korhonen@fimnet.fi
Cutaneous squamous cell carcinoma is one of the most common cancers of the skin. A more precise and timely knowledge of these tumours is needed in order to provide optimal care. This study describes the epidemiology of cutaneous squamous cell carcinomas in a patient cohort in Finland, analysing the anatomical distribution, histopathological features and treatment modalities to reflect the typical day-to-day clinical practice.
Cutaneous squamous cell carcinoma (cSCC) is one of the most common cancers of the skin. Although rarely fatal (1), cSCC reduces the quality of life of patients through functional impairment and severe cosmetic and psychosocial sequelae (2, 3). The incidence of cSCC is increasing in white populations worldwide (4). Thus, cSCCs have a substantial and increasing impact on healthcare costs (5). Most cSCCs occur in people aged 60 years or older (6), a population expanding rapidly in aging societies in the near future. Consequently, cSCCs are creating an increasing demand on healthcare systems due to restricted resources (5, 7).
Although the burden of disease caused by cSCC is known to increase, the available registry data on cSCC epidemiology may still underestimate its impact on the healthcare systems (4, 8). In most epidemiological studies, only the first case of cSCC in a patient is registered while subsequent and multiple tumours are not taken into account (4). For future planning, a more precise and timely knowledge of cSCC epidemiology and tumour characteristics is needed for optimal patient care (7).
We carried out a retrospective 10-year study to determine the frequency and characteristics of all detected and treated cSCCs in a Finnish regional university hospital cohort. Finland is a Nordic country with approximately 5,5 million inhabitants of whom 30% have Fitzpatrick’s skin phototypes I or II and 60% type III (9). We have analysed the anatomical distribution, histopathological features and treatment modalities to reflect typical day-to-day clinical practice in patients with cSCC, including those with multiple tumours.
The pathology database of Fimlab Laboratories was searched for the histopathologic diagnosis of ‘cutaneous squamous cell carcinoma’ between 1 January 2006 and 31 December 2015. Fimlab provides the laboratory services in Pirkanmaa region of Finland, meaning that all patients with a cSCC diagnosis in the region were identified. In situ cSCC were excluded. We reviewed the clinical records of Tampere University Hospital, which is the region’s largest hospital and the tertiary referral centre of Pirkanmaa, for all identified cSCC patients. Data regarding demographic factors, including patient age at diagnosis of the primary tumour, sex and associated diseases, particularly immunosuppression, were registered. If the clinical notes indicated that the patient had cSCC before year 2006, this was registered.
Features of the tumours including the anatomic localisation, differentiation and depth of invasion were obtained. Degree of differentiation was classified either as well, moderate or poorly. Diagnostic duplicates, i.e. tumours first biopsied and then (re-)excised, were taken into account and reassessed to identify the actual number of primary cSCCs. Patients with multiple primary cSCCs diagnosed in the study period were included, and each case of cSCC was analysed separately. The histopathological features of each cSCC were based on the pathology reports of both the biopsy and the surgical excision specimen, using the sample with the poorest differentiation and the deepest invasion depth of the tumour. Based on the clinical notes, the tumours were assigned to one of the following 10 anatomic sites: lip, eyelid, ear, face (which excluded the 3 aforementioned sites), scalp and neck, trunk, upper extremity, lower extremity, anogenital area or oral cavity.
The treatment method was recorded in each case. The clearance of microscopic surgical margins, i.e. the excision borders free of tumour cells to the edge (lateral resection margins) and to the bottom (deep resection margins) was recorded in millimetres (mm). Results of radiological imaging i.e. X-ray, ultrasonography, computed tomography examinations performed due to cSCC were registered.
The demographic variables and clinical data of the cSCCs were assessed using descriptive statistics and frequency tabulation. For the crude incidence calculations, annual population numbers of Pirkanmaa region (situated at latitudes around 61°N) were obtained from the Official Statistics of Finland (10). In 2006 (beginning of the study period), the population of Pirkanmaa was 473,490 and in 2015 (last year of the study), 506,114. The annual crude incidence rates were expressed as the number of cSCC cases per 100,000 people. The numerator of the incidence rate was the number of cSCC diagnosed each calendar year, independent of the number of patients. Thus, a patient could be counted more than once a year if we were certain that the new tumours were not residual or recurrent.
Categorical data were described by number of patients with percentages. Differences between the categorical variables were tested by Pearson chi-square test or Fisher’s exact test. The analyses were carried out using IBM SPSS Statistics for Windows, Version 23.0 software (IBM Corp., Armonk, NY). Due to the skewed distributions, continuous variables were shown by medians with ranges and differences between the two distributions were tested by Mann-Whitney test. Statistical analysis were performed using IBM SPSS Statistics version 23. Trends in the time period were tested by Single ordered Kruskall-Wallis test or Cochran-Armitage trend test using StatXact-4 version 4.0.1 (Cytel Software Corporation).
The institutional review board of Tampere University Hospital, Finland approved this retrospective study.
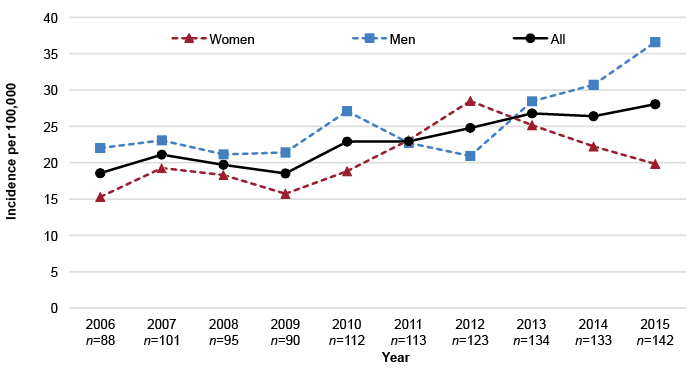
The pathology database search yielded 1,698 cases of invasive (non-in situ) cSCCs. After the medical record review, 567 diagnostic duplicates, i.e. overlapping data on biopsy and excision of the same case of cSCC, were excluded, leaving 1,131 tumours in 774 patients in the study cohort. The annual number of cSCCs has risen during the study period from 88 (51 in men and 37 in women) in 2006 to 142 (91 in men and 51 in women) in 2015. The crude incidence (per 100,000 persons) increased from 18.6 in 2006 to 28.1 in 2015 (Fig. 1). No significant difference between men (22.0 to 36.6) and women (15.3 to 19.8) was found (p = 0.722).
Most cSCC cases were detected in people aged 80–89 years. The annual number of cSCC rose, especially in people aged 85 years or older. Also the age-specific incidence increased with age (Fig. 2). The median age of cSCC patients was 78 (range 39–100) years in men and 83 (range 16–99) years in women. The age distribution of patients differed in men and women (p< 0.001) (Table I).
During the study period, 588 patients (76.0%) had one cSCC, 116 (15.0%) had two cSCCs and 70 (9.0%) had 3 or more cSCCs (Table I). Total of 77 (9.9%) patients have been treated for cSCC before the start of the study period. Immunosuppression was present in 81 (10.5%) patients, due to organ transplantation (n = 37), rheumatoid arthritis (n = 23), chronic leukaemia (n = 10) and lymphoma (n = 11). Of the organ transplant recipients, 8 patients had a heart transplant, 26 kidney transplant and 3 liver transplant. None of the patients had HIV, and none had received treatment with BRAF inhibitors. Out of all 1,131 tumours, 191 (16.9%) cSCCs were diagnosed in the immunosuppressed patients. These patients had a median of two (interquartile range [IQR] 1–6, range 1–26) tumours per patient during the study period, while the immunocompetent patients had a median of one (IQR 1–2, range 1–9) tumour (p < 0.001).
Tumour characteristics are summarized in Table II. The most common location of cSCC was the face (excluding ears, lips and eyelids), accounting for 50% of all cases. The proportion of facial cSCC, out of all the cSCCs, increased with age: among patients 85 years or older 63% of tumours were located on the face. Total of 12% of the cSCC were located on the upper extremity, which was the second most frequent location. The location of tumours was different in men and women (p < 0.001). A total of 9.4% of cSCCs were located on the ear, of which 93% were in men. Scalp, neck and trunk were more commonly affected in men than in women.
The number of tumours on the face increased over the study period with the annual incidence (per 100,000 persons) increasing from 8.9 in 2006 to 13.8 in 2015. The incidence of trunk cSCC increased from 0.6 in 2006 to 1.8 in 2015, and, the annual proportion of trunk cSCCs out of all cSCCs increased from 3.4% to 6.3%. Conversely, the annual proportion of cSCC of lip and lower extremity declined from 5.7% in 2006 to 0.7% in 2015 and 9.1% in 2006 to 4.9% in 2015, respectively. There was an overall increasing trend of cSCCs over the study period (p = 0.018) but no statistically significant change in any specific localisation of tumours.
The majority of cSCCs were well differentiated (46%). Patients with a well-differentiated cSCC were 4 years younger than those with a poorly differentiated cSCC (median age 79; IQR 71–85 and 83; 77–88, p < 0.001). The tumour differentiation showed a small but not statistically significant (p = 0.301), shift from poorly to well differentiated. In 2006 tumours were well differentiated in 42.0% and poorly in 10.2% of cases, while in 2015 they were well differentiated in 52.1% and poorly in 6.3% of cases. Most tumours (32%) had an invasion depth of 2 mm or less, although information on the depth of invasion was available in only 60% of the cases. During the study period the coverage of invasion depth data was improved from 35% in 2006 to 66% in 2015.
All the cSCCs were treated with excision to achieve the macroscopic resection margins recommended by the international guidelines. Lateral resection margins were on average larger (median 4 mm, range 0–30) than the deepth resection margins (median 2 mm, range 0–20), although 31.6% and 42.0%, respectively, of these data were not mentioned in mm in the pathology reports or there was only scar or premalignant changes left in the final resection (definite margins could not be identified).
Adjuvant radiotherapy was used in 76 (6.7%) cases. Radiotherapy was used in 4.2% of well differentiated and 19.1% of poorly differentiated cSCC cases. In the majority of radiotherapy-treated cSCCs the depth of invasion was over 4 mm (in 24 out of 40 cases where invasion depth data was available on the pathology report). Radiological imaging was performed for 61% of all cSCC patients. Ultrasonography was the most commonly used imaging technique (430 patients). Chest X-ray was used in 363 patients and computed tomography in 86 patients. Radiological imaging was performed in 51% of well differentiated cSCC cases, compared to 74% of poorly differentiated cases.
Fig. 1. Annual number and crude incidence (per 100,000 persons) of cutaneous squamous cell carcinoma, 2006–2015.
Fig. 2. Annual incidence (per 100,000 persons) of cutaneous squamous cell carcinoma in age groups, 2006–2015.
Table I. Patient characteristics
Table II. Tumour characteristics
This study shows that the annual number and crude incidence of cSCC increased during the 10-year study period. The actual number of cSCC cases obtained, represented a true reflection of the workload, since each case was verified by reviewing the medical records and multiple tumours of the same patient were taken into account. This increase is in line with the results of previous studies in other countries (4, 8, 11–13), although differences in data collection methods mean that the numbers cannot be directly compared (4, 14).
The incidence of cSCC increased with age, being highest among those over 80 years old. Patients with a poorly differentiated cSCC were in mean 4 years older at the time of diagnosis than those with a well-differentiated cSCC. Like many other societies, Finland is facing the challenges of an aging population since the proportion of persons aged ≥ 65 years is estimated to rise from the present 20% to 29% by 2060 (15). This will lead to an older patient population with an increased risk of skin cancer and an increased workload for the dermatological health services (6, 7) and multiprofessional skin cancer team, which is often required (7).
During the study period, one fourth of patients had more than one cSCC and one tenth had been treated for cSCC before the study period. The mean risk of developing a subsequent cSCC within 3 years of the initial diagnosis has been estimated to be 18% (range 9–23%) (16) and 30–50% of patients with cSCC will develop another one within 5 years (17). The strongest predictors of future risk of keratinocyte carcinoma (cSCC and basal cell carcinoma), are a past history of an excised skin cancer and high age (18). In one study, the majority (67%) of patients with keratinocyte carcinoma who underwent a whole body skin examination had additional lesions requiring treatment (19). Currently there is no standardised follow-up schedule for patients with cSCC but the European Dermatology Forum (EDF), the European Association of Dermato-Oncology (EADO) and the European Organization of Research and Treatment of Cancer (EORTC) consensus group proposes follow-up clinical examinations annually for 5 years even for patients with a low risk cSCC (17), imposing considerable demands on dermatological services.
In our study, most cSCCs were located in sun-exposed areas, such as the face and upper extremity. Cumulative lifetime exposure to ultraviolet (UV) radiation from the sun is the principal risk factor for the development of cSCC (14, 20). In our study, there was no statistically significant change in the localisation of tumours during the study period, but the annual proportion of trunk cSCCs to all cSCCs increased during the study period. The same observation has been reported in other Nordic countries (11, 21). This may reflect the increased UV radiation exposure of the trunk as a result of changed tanning habits (fewer clothes, intentional outdoor tanning, sunbed use), implying lying postures and changes in fashion trends (11, 21). A notable difference between men and women was observed in the localisation of cSCC concerning the ear, scalp and neck, possibly related to sex differences in hair coverage (22, 23).
Depth of invasion and microscopic surgical resection margins in mm were often not mentioned in the pathology reports or definite margins could not be identified. Deep resection margins were generally smaller than lateral resection margins. Tumour depth is of great importance in identifying high risk cSCC and should be reported in all cases (24). Changes have already been made in our pathology laboratory to improve the histopathological information by modifying the structure of the pathology report form. The incomplete excision rate of cSCC ranges between 6–16% and the authors of a prospective observational study on incomplete excisions recommend more careful tumour markings and using deeper margins (25).
During the study period the degree of differentiation in cSCCs showed a minor shift from poorly to well differentiated. This may be a reflection of earlier detection of cSCC during recent years of the study period. However, approximately 48% of cases were moderately to poorly differentiated which is a high risk feature of cSCC (17).
The study has several limitations. Due to the retrospective nature of the study, it was not possible to collect all relevant information of the cSCCs, including the clinical diameter of the tumours. The cohort was drawn from a single hospital, although this indicates that all cases of cSCC in the geographical area of the hospital were probably included.
The incidence of cSCCs is increasing, especially in older patients. CSCCs are a future challenge, meaning that more and older patients may require treatment by a multiprofessional skin cancer team. Considering that patients may have multiple tumours, are at risk to develop new SCCs and also other additional skin cancers may be found, it is extremely important to examine patients’ whole body at the follow-up visits (16, 17, 19). Prophy-lactic measures, such as, education on sun avoidance and protection, and early detection and intervention are necessary in order to reduce the development of more invasive cSCCs (14, 17).
The study was financially supported by The Finnish Dermatological Society (a grant awarded to Dr. Korhonen). This organisation had no involvement in the study design; collection, analysis and interpretation of data; writing of the manuscript; and decision to submit the manuscript for publication.


 Click to show fullsize
Click to show fullsize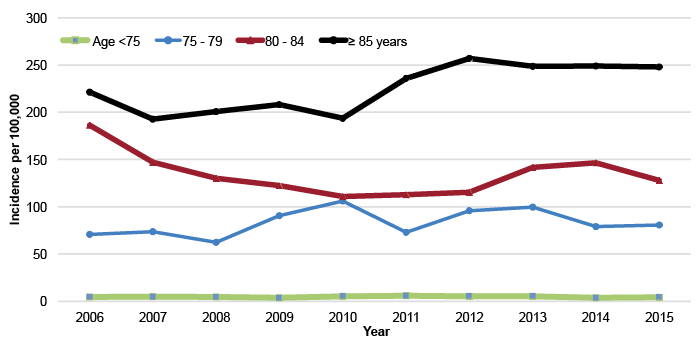 Click to show fullsize
Click to show fullsize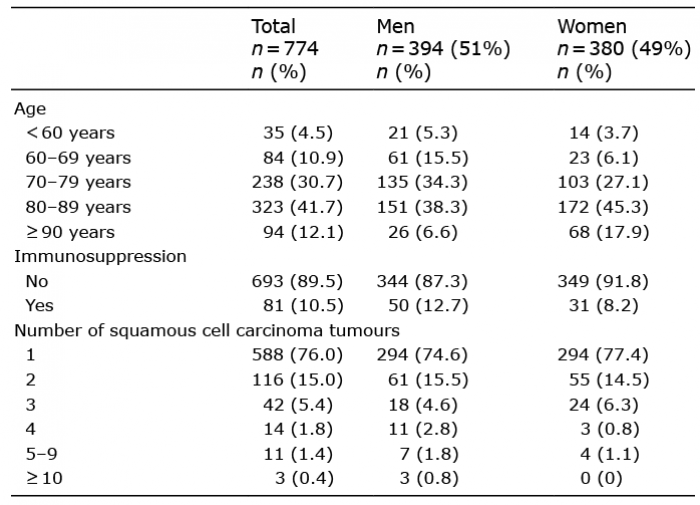 Click to show fullsize
Click to show fullsize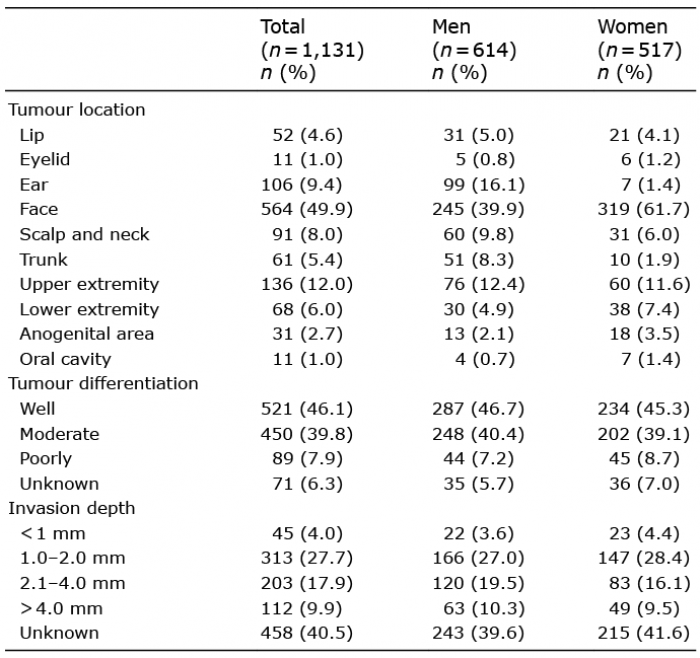 Click to show fullsize
Click to show fullsize