


1Department of Dermatology and 6Department of Psychiatry, Parc de Salut Mar, 2ISGlobal, 3IMIM (Hospital del Mar Medical Research Institute), 4Universitat Pompeu Fabra (UPF), Barcelona, 5CIBER Epidemiología y Salud Pública (CIBERESP), Madrid, 7Department of Psychiatry, Hospital Universitari Vall d’Hebron, Barcelona, Spain, and 8Department of Dermatology, University of Rochester School of Medicine and Dentistry, Rochester, NY, USA
Psoriasis is a chronic skin disease associated with considerable physical and psychological comorbidities. Stress and emotional disturbances have been implicated in both triggering the onset and exacerbation of psoriasis. In order to determine the level of perceived stress and mood alterations in patients with psoriasis and their association with disease severity, 300 individuals completed diverse validated questionnaires assessing stress and psychological mood. Evaluation of perception of disease was also measured. A significant association between psoriasis severity and mood, emotional disturbances and an impact on assessments of the quality of life were observed. Particularly, Montgomery-Asberg Depression Rating Scale, Hamilton Rating Scale and Hospital Anxiety and Depression Scale for Depression detected a significant risk for depression in relation to the disease severity. The association between depression features, anxiety and perceived stress with psoriasis severity is important and can influence the appropriate management of psoriasis.
Key words: psoriasis; anxiety; depression; stress; mood; quality of life.
Accepted Jan 7, 2019; E-published Jan 9, 2019
Acta Derm Venereol 2019; 99: XX–XX.
Corr: Fernando Gallardo, MD, Department of Dermatology, Parc de Salut Mar, Passeig Maritim, 25-29, ES-08003 Barcelona, Spain. E-mail: fgallardo@parcdesalutmar.cat
Population-based studies indicate that psoriasis associates a greater risk of comorbidities that alter mood, such as anxiety and, above all, depression. We applied a complete panel of validated questionnaires to perform a full psychopathological exploration according to the DSM-V classification of psychiatric diseases in 300 psoriatic patients. A dose-response association with depression and anxiety (the more severe psoriatic patients have more risk of having depression or anxiety) was observed. The Montgomery-Asberg Depression Rating, Hamilton Rating for Depression, Hospital Anxiety and Depression scales (for depression), and State Anxiety Inventory (for anxiety) seem to better detect such mood comorbidities in psoriatic patients.
Psoriasis affects about 2.3% of the Spanish population. An increasing prevalence has been detected, probably due to a higher awareness and earlier diagnosis, rather than an increment of the total number of cases (1, 2). Individuals are likely to present differing levels of disease severity throughout their lifetime, experiencing ‘spontaneous’ remissions and flare-ups during the disease course. The pathogenesis of psoriasis is not fully understood but includes hereditary and environmental factors.
Psoriasis is considered to be a psycho-physiological disease, a dermatological condition which evolution may be influenced by psychological aspects. Patients often point out stress as an exacerbating factor. Some studies support the fact that stress may play a relevant role in the onset and course of psoriasis in comparison with other conditions, such as urticaria or atopic dermatitis (3, 4). Relationships between emotional stress and psoriasis severity have been reported and a conclusive link between skin symptoms and mood was demonstrated (5). Moreover, large-scale studies have evaluated the association between depression, anxiety and suicidal ideation with psoriasis. A significantly higher prevalence of psychological and psychiatric disorders in patients suffering from psoriasis has been reported (6–8).
The present study aims to assess the impact of psychosocial events or mood disorders on the psoriatic population and to explore their link to the quality of life (QoL) and health status related to skin disease severity. To accomplish this, both stress level (secondary to recent-previous life events) and current psychological co-morbidities were measured among psoriatic individuals with different levels of skin disease severity using a complete set of validated questionnaires. In contrast to other studies, a large number of cases were evaluated, using an efficient methodology to record stressful life events and psychological mood variables. The impact of the stress level on the severity of psoriasis, considering both the physician and the patient’s points of view was also assessed.
This observational study recruited 300 psoriatic adult patients, who completed a set of validated questionnaires assessing perceived stress of known origin, or associated with disorders of the psychological mood. This study was conducted at the Department of Dermatology in a tertiary referral center in Barcelona over a period of 18 months and was approved by the institutional ethics committee. The study population included outpatient representative for the psoriasis population since almost all patients with moderate to severe psoriasis in our geographical area are evaluated in our center. Exclusion criteria included diagnosis of severe uncontrolled psychiatric disorders (i.e. schizophrenia or bipolar states) and/or presence of difficulties in comprehension or communication or psychiatric treatments that may influence the course of psoriasis severity (i.e. lithium salts). The socio-demographic and clinical variables collected in this study included: sex, age, psoriasis subtype, disease duration, frequency of exacerbations, and presence of arthritis and nail psoriasis. Pain and itching symptoms, related to the skin disease; smoking or alcohol intake and presence of obesity, as other elements related to the psoriasis severity, were also recorded.
The survey measured the psycho-emotional status. Stressful life events were evaluated using Holmes and Rahe’s Social Readjustment Rating Scale or Life Events Scale (LES) (9). LES describes situations, which generate stress in the majority of the population. According to a scoring system, which includes 43 items and evaluates a period of 12 months, patients are classified into 3 categories: mild, moderate or severe stress.
Hospital Anxiety and Depression (HAD) Scale was used to measure anxiety and depression (10). Hamilton Rating Scale for Depression (HRSD) and Montgomery-Asberg Depression Rating Scale (MADRS), as a clinician-administered measure for depression, were also utilized (11, 12). Spielberger State-Trait Anxiety Inventory (STAI) was administered to the participating subjects and the differences in State Anxiety Inventory (SAI) and Trait Anxiety Inventory (TAI) were analyzed (13).
The impact of disease on health-related quality of life (HRQoL was measured using the Mental (MCS) and Physical (PCS) Component Summary scores of the SF-12, and Dermatology Life Quality Index (DLQI; score of 0–30) (14, 15). DLQI is a dermatology-specific 10-item questionnaire that considers aspects of the impact of skin disease on a patient’s QoL in the preceding week, which was filled in by the patients themselves. They used a Likert scale with 4 alternatives to evaluate the impact of disease on HRQoL. Additional measurement included the 0–100 mm visual analogue scale (VAS) for pruritus evaluation.
Two dermatologists, using the Psoriasis Area and Severity Index (PASI), Body Surface Area (BSA) and Psoriasis Disability Index (PDI) (16), evaluated the severity of psoriasis. The rule of tens (PASI, BSA and DLQI indexes) was used as the reference for considering the severity of psoriasis as mild, moderate or severe (17, 18).
The data were analyzed in relation to 2 groups separated on the basis of the severity of the psoriasis: moderate–severe psoriasis (patients with PASI ≥ 10 or BSA ≥ 10 or DLQI ≥ 10) and mild psoriasis (patients with , < 10 and BSA < 10 and DLQI < 10). Student t-test and χ2 tests were used for continuous variables and categorical variables, respectively, in order to compare the different characteristics between the two groups. Logistic regression was calculated for the indexes of psychological stress and severity of psoriasis, as well as for the psychological stress indexes and visibility of psoriasis, adjusted for all confounding factors. Calculations were performed using the statistical package Stata/SE 12.1 (Texas, USA).
The sample included 300 patients (47.3% men, 52.7% women) from 18 to 89 years of age (mean = 49.7). The median number of years patients suffered from the disease was 13. The majority of patients (62%) had a classical plaque form of the disease. Specific localized forms of the disease were present in 48% of cases (palmo-plantar: n = 45 or scalp psoriasis: n = 101). Thirty percent of patients had one or more flares, needing additional treatment, during the last year and in 209 cases psoriasis was considered to be chronic with a stable clinical course. Pruritus was significantly related to disease severity. The clinical features of the disease, the presence of arthropathy or nail involvement are detailed in Table SI, stratified by the severity of the skin disease.
Disease severity, established using Finlay’s rule of tens, in our cohort was as follows: 184 (61%) patients were considered to have moderate-severe psoriasis, whereas 116 cases (39%) were considered to have mild disease. The mean ± standard deviation (SD) PASI score was 13.0 ± 8.5 and mean BSA 23 ± 13.6%. In the mild severity group, there was a female predominance (56%) with a PASI score of 2.8 ± 2.4 and a BSA of 4.0 ± 2.8%. The DLQI score in the mild group (PASI < 10 and BSA < 10) compared to the moderate-severe group (PASI or BSA≥ 10) was 2.4 ± 2.7 vs. 4.9 ± 5.2, respectively. No significant differences were found between patients with mild and moderate–severe psoriasis in terms of the different demographic variables or regarding tobacco or alcohol consumption (Table SI).
The presence of psycho-emotional comorbidities (34%) or psychiatric disorders (28%) was detected in 49% of patients regardless of skin disease severity (Table SI1). No differences between patients with mild or moderate–severe psoriasis, with regard to previous history of psycho-emotional or psychiatric disorders, were detected, except for the need for current medical treatment in psychiatric patients with severe psoriasis (Table SI). Males were less susceptible to symptoms of anxiety or depression than females but reported a greater impact on the QoL.
Differences in depression scores, related to psoriasis severity, were found. HAD score for depression for all psoriasis patients of our population showed a median of 2 with a mean of 3.24, for patients with mild psoriasis and 3.38 for those with moderate-severe disease (Table I). We did not find any significant differences in the HAD depression questionnaire in relation to the skin disease severity, measured either by PASI or BSA, but patients with severe DLQI showed a higher risk of depression with an odds ratio (OR) of 3.51 (95% CI 1.32–9.30) for the highest tertile of HAD scores (Table II, Fig. 1 and Table SII).
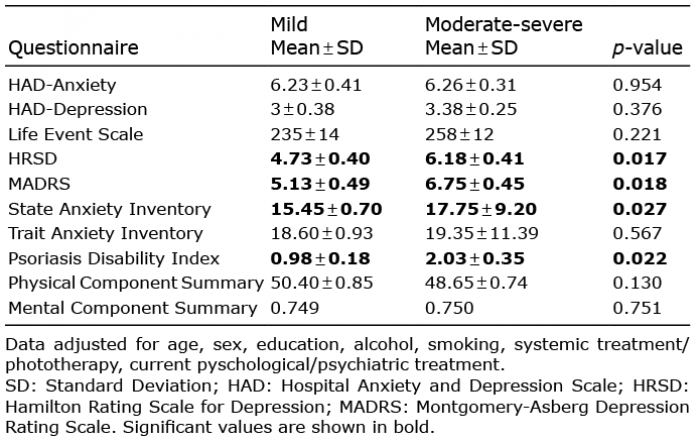
Table I. Psycho-emotional indicators according to severity of psoriasis groups
Table II. Different indexes of psycho-emotional disorders and stress level measurements according to the psoriasis severity variables
Fig. 1. Risks of having psycho-emotional symptoms according psoriasis severity variables. Odds ratio and 95% confidence interval and indication of dose-response for the different indexes of psycho-emotional disorders and stress level and measurements of psoriasis severity. PASI: Psoriasis Area Severity Index; BSA: Body Surface Area; DLQI: Dermatology Life Quality Index; HAD: Hospital Anxiety and Depression Scale; LES: Life Event Scale; HRSD: Hamilton Rating Scale for Depression; MADRS: Montgomery-Asberg Depression Rating Scale; SAI: State Anxiety Inventory; TAI: Trait Anxiety Inventory; PDI: Psoriasis Disability Index; PCS: Physical Component Summary; MCS: Mental Component Summary; T: tertile; P: percentile.
The level of depression was much higher in the moderate–severe than in the mild group, both in the MADRS and HRSD. When applying HRSD scale, we observed significant differences in depression symptoms between mild (mean ± SD 4.73 ± 0.40) and moderate-severe disease (6.18 ± 0.41) (p-value < 0.01) (Table I). Interestingly, psoriasis severity showed a clear trend associated with higher scores in the MADRS in all evaluated severity indexes (mean ± SD 6.75 ± 0.45 for moderate–severe vs. 5.13 ± 0.49 for mild psoriasis, p = 0.0018) (Tables I and II and Fig. 1). Moreover, skin severity indexes showed a significant trend in a dose-response manner, i.e., the more severe patients trend towards a higher risk for depression features (Fig. 1, Table SII). These data may indicate that MADRS test could be the most accurate one to evaluate depression risk associated with psoriasis.
Overall, anxiety commonly affects psoriatic patients, and individuals with more severe disease had worse scores on the anxiety questionnaires (Table I). HAD score for anxiety in all evaluated psoriasis patients disclosed a mean ± SD value of 6.25 ± 4.33 and no significant differences were found regarding skin disease severity in the univariate analysis. Conversely, in the adjusted model, these scores show that patients with severe psoriasis have a higher risk of anxiety compared to those with mild disease (Table SII). STAI questionnaires also detected a high risk for anxiety in patients with psoriasis (mean ± SD 16.83 ± 8.61) and revealed differences regarding those presenting with mild or moderate–severe skin complaints (p-value < 0.02) (Tables I and II, and Table SII), indicating that STAI test could be an interesting and reliable tool for evaluation of anxiety symptoms in patients with psoriasis.
Patients often acknowledged psychologically stressful life events in the last year, prior to the beginning of the study. Twenty-three percent of cases reported a low score in stressful events with less than 130 points, 43% recorded a score between 130 and 280 and 35% reported important stressful events with a total score higher than 300. There were no significant differences in the mean score of stressful events between mild and moderate–severe disease (Tables I and II). Moreover, we grouped the stressful events into aggravating or improvement categories (data not shown) and we did not find any significances, regarding skin disease severity.
Mood and affective disorders are frequently observed in patients with dermatological diseases and psychological or psychiatric co-morbidities have been found in up to 40% of psoriatic patients (19, 20). Psoriasis, as a disease causing a significant impact on the physical aspect, may cause disturbances in the functional aspects and affect patients’ self-esteem (21, 22). Importantly, several studies have pointed out that psoriatic patients are more prone to develop depression or have suicidal ideation in comparison with the general population (23). In view of the influence of psychological factors on the evolution of psoriasis, there have been numerous research studies, assessing the effects of psychological therapies, (24, 25) including hypnosis (26), biofeedback (27, 28) and treatments for stress, anxiety or depression (29, 30).
Based on reliable structured psychiatric interviews, with the use of structured questionnaires, we compared the frequency of anxiety, depression and stress levels in patients suffering from psoriasis, with regards to the severity and subtypes of the skin disease. In our study, we found higher levels of depression and anxiety attributes in patients, suffering from severe forms of psoriasis.
The detailed analysis of PASI, BSA and DLQI showed a significant relationship between depression and anxiety scales and the burden of psoriasis (31). In addition, the prevalence of mental disorders was significantly higher in patients with psoriasis, especially in those with higher disease severity; which would suggest that this ‘at risk’ population requires closer attention and possibly more intense therapeutic interventions in the management of their emotional disturbances.
Depression status was evaluated with MADRS, HRDS or HAD depression scales and we found that patients with the more severe psoriatic disease have a higher degree of depression and psoriasis severity increases, more than two-fold, the risk for developing depression features in our series. Differences within depression scores related to psoriasis severity were found. Particularly, MADRS rating for depression was the most sensitive questionnaire, in detecting pathological worries in patients with severe skin disease when measured by PASI or BSA. In addition, these scores have been reported to detect that people with psoriasis have a higher risk of depression compared with people without the skin disease. Psoriatic patients from our population showed higher scores in HRSD and MADRS than those in a non-psoriatic population (32–35).
Both patient groups had high mean anxiety scores; however, we found that patients with moderate–severe psoriasis have higher mean scores in anxiety tests. The highest adjusted OR for anxiety was found in STAI tests among patients with higher psoriasis severity (assessed with DLQI), which indicates that the risk of neurotic symptoms increases in patients with severe psoriasis.
Emotional stress is considered as one of the psychological variables most commonly related to health. Psoriatic patients and physicians commonly associate stress or worry with the course of the disease. Psoriasis is associated with poor life satisfaction, affective expression and psychological well-being, as well as anxiety or depression (36). However, there is limited and conflicting evidence concerning the role of psychological stress in relation to the onset or exacerbation of psoriasis (5). Clearance of psoriasis may improve stress, patients’ well-being, anxiety or depression symptoms. Some studies have shown that patients with severe psoriasis have progressively adapted to the impact of the disease (37, 38).
Several studies have demonstrated that psoriasis is associated with stress in more than half of patients (39). LES is the most frequently used questionnaire for measuring levels of emotional stress (9). In our series, adjusted ratings for variables, considered as aggravating or improving factors in stressful life events within one preceding year, disclosed that most psoriatic patients (76%) suffered from moderated to high levels of stress. This observation reinforces the role of stress in the patho-genesis of psoriasis. Stressful life events may represent not only a cause but also an effect and could explain the lack of differences observed in relationship to psoriasis severity or in cases with specific anatomical localizations (palmo-plantar or facial and scalp psoriasis).
DLQI scores change significantly with the clinical activity of psoriasis and can aid decision-making in the patient management. Perception of illness by patients does not always coincide with the objective measurements of psoriasis clinical severity (40). In our series, the DLQI test is associated with the emotional disturbances in different indexes. Impact on the functional aspects of patients was also observed in relation to the skin severity. In our experience, PDI test seems to be a more accurate tool, when evaluating functional impact of psoriasis, in comparison to SF-12 (both PCS and MCS) questionnaires. PDI is closely related to the QoL impairments and we have not found differences regarding either the extension of the skin disease or the presence or absence of specific localized forms of psoriasis.
In conclusion, our study suggests the presence of a significant relationship between emotional disturbances and severity of the disease. We detected a remarkable impact of psoriasis on functional activity and QoL. Stress, not only secondary to psychological disorders but also in relation to recent stressful events, is commonly reported in psoriatic patients. Recognition of the association between stress and psoriasis seems to be an important factor that should be considered in their management. These data reinforce the notion that psycho-emotional, functional and QoL interventions can therefore be directed more appropriately, especially for patients with moderate–severe disease.
We thank Raquel Garcia-Esteban (ISGlobal) for her contribution in the statistical analysis.
This study was supported by grant “Agència d’ Avaluació de Tecnologia i Recerca Mèdiques” (AATM project 1892/I/04), Generalitat de Catalunya, Barcelona, Spain.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize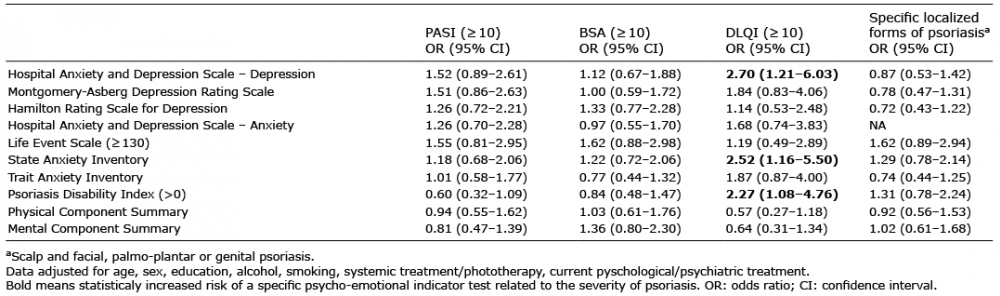 Click to show fullsize
Click to show fullsize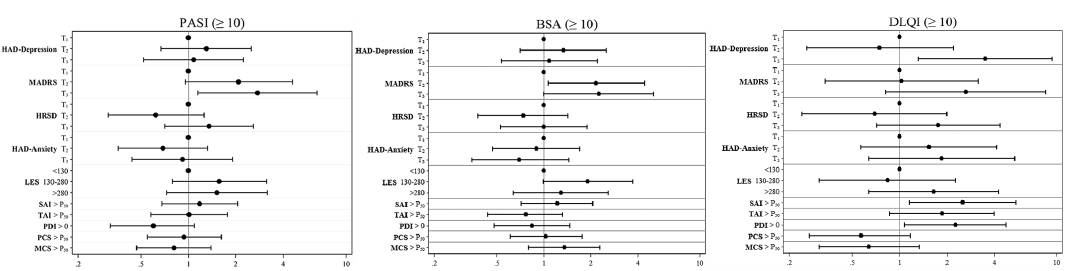 Click to show fullsize
Click to show fullsize