


Departments of 1Dermatology, 2Pathology and 4Internal Medicine I, Medical University of Vienna, Waehringer Guertel 18-20, AT-1090 Vienna, and 3Private Hospital Rudolfinerhaus, Vienna, Austria. *E-mail: alessandra.handisurya@meduniwien.ac.at
Accepted Jan 15, 2019; E-published Jan 17, 2019
Infections with mucosal high-risk (HR-) human papillomaviruses (HPVs) cause mucosal cancers of the anogenital and oropharyngeal tract. Furthermore, they are associated with the development of skin cancers located on the hands. Available data on viral prevalence and type spectrum in these tumours are highly variable. Some studies show detection rates of mucosal HR-HPV in up to 90% (1–5), while others fail to detect viral DNA (6, 7). Viral presence is reported to be confined to tumours on peri- and subungual sites, or predominantly on proximal phalanges rather than ungual sites (2, 3).
This study investigated cutaneous squamous cell carcinomas (SCCs) and Bowen’s diseases (BDs), an SCC in situ, located on the hands for the presence of mucosal HR-HPV and the respective genotype(s). In addition, candidate biomarkers for viral activity (p53/p16/p21) and therapeutic intervention (epidermal growth factor receptor (EGFR)) were analysed and expression correlated to papillomaviral state.
The methodology is given in Appendix S1.
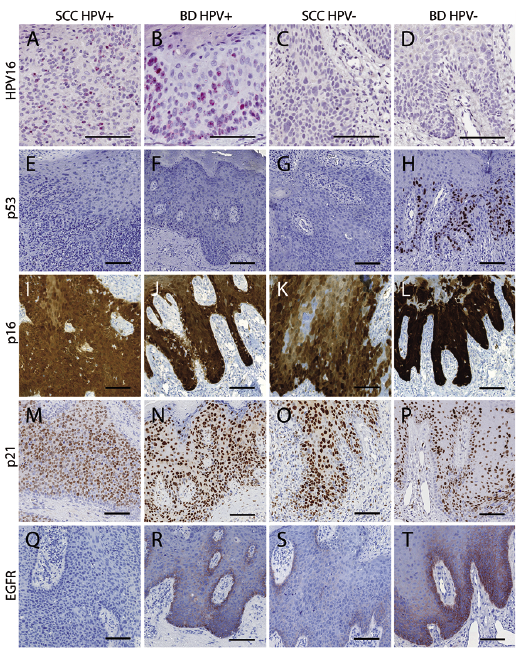
Mucosal HR-HPV DNA was detected in the majority (56.3%) of cutaneous SCCs (n = 9) and BDs (n = 28) located on the hands (Table SI). The percentage of HR-HPV-positive tumours was lower in SCCs (33.3%) compared to BDs (65.2%). Viral DNA was more frequently present in skin tumours of the nail unit (83.3%) and fingers (63.6%) than of the back of the hands (0%) or wrists (33.3%). The predominant genotype was HR-HPV16 (68.4%) followed by 33 (15.8%), 52 (10.5%) and 26 (5.3%). In the majority (94.4%) of virus-positive tumours, infection with a single virus type was identified, in one SCC (5.6%) co-infection with HPV33/52. Viral E6/E7 mRNA expression within HPV-positive, but not HPV-negative, tumours was confirmed by RNA in situ hybridization (Fig. 1A–D), indicating transcriptional activity of the viral oncogenes. Hybrid capture-2 results (Table SII) further corroborated the presence of mucosal HR-HPVs. Interestingly, viral loads in SCCs were lower (mean relative light units (RLUs) 2.7) than in BDs (mean RLUs 305.8); however, due to the small number of SCCs definite conclusions were impeded. To evaluate possible candidate biomarkers for viral activity, expression of certain HR-HPV-dependent molecules was investigated. Most tumours (91.2%) did not display positive p53-immunostaining (Fig. 1E–H). Two BDs, lacking HR-HPV DNA, showed nuclear p53-immunostaining in the basal and lower suprabasal layers (Fig. 1H), while all others and all SCCs, irrespective of viral status, were p53-negative.
In contrast, p16 expression was found in the majority (91.7%) of tumours, in 82.4% of virus-positive (Fig. 1I, J) and all virus-negative tumours (Fig. 1K, L). Both, staining intensities and numbers of p16-immunopositive cells, were similar between these 2 entities and observed differences were not significant. Only 8.3% of the samples, 1 SCC and 2 BDs, did not express p16 and these specimens were concomitantly HPV16 DNA-positive (not shown). Qualitative and quantitative expression of p16, regardless of viral presence, also did not differ between SCCs (88.9%) (Fig. 1I, K) and BDs (92.6%) (Fig. 1J, L).
Immunostaining of p21 was found uniformly in 100% skin tumours. No differences of qualitative or quantitative p21 expression were observed between HR-HPV DNA-positive (Fig. 1M, N) and -negative (Fig. 1O, P) tumours nor between SCCs (Fig. 1M, O) and BDs (Fig. 1N, P).
Evaluation of EGFR showed positive immunostaining in 29.4% of the skin tumours; however, viral presence did not markedly affect its expression. 20.0% of the virus-positive (Fig. 1Q, R) and 28.6% of the virus-negative tumours (Fig. 1S, T) showed positive EGFR-immunoreactivity. Quantitative assessment revealed similar numbers of EGFR-positive cells in virus-positive (mean 620/mm2) and virus-negative (mean 575/mm2) tumours (p = 0.5845). BDs stained more frequently positive for EGFR (36.0%) compared with SCCs (11.1%); however, differences were not significant.
Fig. 1. HPV16 E6/E7 mRNA was detected by RNA in situ hybridization in high-risk human papillomavirus (HR-HPV) DNA-positive squamous cell carcinomas (SCCs) (A) and Bowen’s diseases (BDs) (B), whereas HR-HPV DNA-negative SCCs (C) and BDs (D) lacked specific signals. Expression of p53 protein was restricted to a subset of virus-negative BDs (E–H). P16 expression was found in the vast majority of HR-HPV DNA-positive and -negative tumors (I–L). Nuclear immunostaining of p21 throughout the entire tumour was found uniformly in all specimens (M-P). Specific epidermal growth factor receptor (EGFR)-immunoreactivity was observed in 20.0% of HR-HPV DNA-positive and 28.6% of -negative tumours (Q–T). BDs were more frequently positive for EGFR compared with SCCs.
Detection of viral DNA and transcriptional activity provides additional evidence for a causative association of mucosal HR-HPVs in the development of a subset of skin cancers located on the hands.
At the molecular level, functional inactivation of tumour suppressor proteins p53 and pRb by viral oncogenes E6/E7 is crucial in mucosal HR-HPV-driven carcinogenesis. Immunohistochemically detectable p53 is considered a protein product of genetic mutation or nuclear protein accumulation. The rare presence of detectable p53 in our tumours, and its association with virus-negativity, may be caused by HR-HPV E6-induced degradation of wild-type p53, resulting in loss of the tumour suppressor proteins ability to regulate cell cycle arrest, DNA repair or apoptosis, thereby initiating tumorigenesis. In some virus-negative tumours UV light could have induced mutational inactivation of p53 similar to cutaneous SCCs at other localizations, where mutant p53 were detected in up to 90%. In contrast to mucosal HR-HPV-induced cervical and oropharyngeal cancers, where p16 expression correlates with the degree of virally-induced malignancy and is regarded as a valid surrogate biomarker (8), this does not apply to virally-induced skin SCCs. This is in line with studies reporting abundant p16 expression in genital and extragenital skin tumours independently of viral presence, although a previous study reported higher numbers of p16-positive cells in HPV-positive digital SCCs compared with non-HPV-induced lesions (2, 9–12). The observed p16-immunopositivity in skin tumours of the hands may reflect disturbances in the retinoblastoma pathway and/or genetic changes in pRb, unrelated to HPV infection. Demonstration of uniformly expressed p21 in HR-HPV-positive and -negative tumours reveals that this molecule does not reflect HPV-driven tumorigenesis.
EGFR inhibition strategies are recommended for treatment of several malignancies, including advanced cutaneous SCCs. Based solely on the rate of immunopositivity in our small population, this option does not appear to be promising. While tumorous cells overexpressing EGFR could be more sensitive to targeted drug therapies, determination of its expression alone may not be sufficient to predict functional responsiveness to EGFR inhibition.
Once a patient had acquired an HR-HPV infection, subsequent tumours tended to be virus-positive. Since the acquisition of viral infection was suggested to occur via genital-digital transmission, it is possible that HPV vaccination may also be effective against HR-HPV-induced epithelial malignancies of the hands, either directly by primary prevention of viral infection, or indirectly by reducing the incidence of anogenital infection, thus decreasing exposure of the hands to HR-HPVs.
The authors thank Susanne Drexler, Chris Nava, Monika Weiss and Waltraud Jerney for their excellent technical assistance.
Funding sources: This work was supported by the Anniversary Fund of the Austrian National Bank, Austria, and the Austrian Science Fund (FWF), Austria.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize