


1Dermatology and Venereology Unit, Department of Medicine Solna, Karolinska Institutet and Karolinska University Hospital, and 2Department of Clinical Neuroscience, Division of Ophthalmology and Vision, Karolinska Institutet, Stockholm, Sweden
Dupilumab, the first biologic approved for treatment of atopic dermatitis, has demonstrated significant clinical effect and quality of life-enhancing capacity in clinical trials. In these, dupilumab-associated conjunctivitis where reported in a minority of patients. The present case series describe 10 patients treated with dupilumab where eye complications were very common. We have described patient characteristics, including FLG mutations, atopic history and clinical effect of dupilumab. Nine of 10 developed eye-complications, most commonly conjunctivitis (in 7/10). Other adverse events were herpes simplex virus uveitis and varicella-zoster virus meningitis. Although our case series is small, we conclude that dupilumab is an effective treatment option in severe atopic dermatitis, but that the risk of adverse events from the eyes and recurrence of herpes virus infections should be kept in mind. Close collaboration with an ophthalmologist is recommended, especially among patients with severe, long-lasting atopic dermatitis and/or previous eye disease.
Key words: atopic dermatitis; dupilumab; efficacy; ocular adverse events; safety.
Accepted Jan 16, 2019; E-published Jan 17, 2019
Acta Derm Venereol
Corr: Lina U. Ivert, Dermatology and Venereology Unit, Department of Medicine Solna, Karolinska Institutet and Karolinska University Hospital, SE-171 76 Stockholm. E-mail: lina.ivert@ki.se
Dupilumab, the first biologic approved for treatment of atopic dermatitis, has demonstrated impressive clinical effect and quality of life-enhancing capacity in clinical trials. In these, dupilumab-associated conjunctivitis was reported in a minority of patients. We describe 10 patients treated with dupilumab where eye complications where common, suggesting the importance of close collaboration with an ophthalmologist. This is especially warranted among patients with severe, long-lasting atopic dermatitis and/or previous eye disease.
Atopic dermatitis (AD) is a common chronic inflammatory skin disease characterized by a T-cell (Th2)-mediated immune response and epidermal dysfunction (1). The prevalence of AD in industrialized countries has increased over recent decades, and is currently estimated to be in the range 15–30% in children and 2–10% in adults (2). Topical therapies, such as glucocorticoids, calcineurin inhibitors and moisturizers, and phototherapy have limited efficacy in moderate to severe AD. Severe cases of AD are treated with systemic drugs, such as cyclosporine, azathioprine, methotrexate (MTX) and mycophenolate mofetil. All of these drugs are used off-label, with the exception of cyclosporine, which is approved for short-term treatment of severe AD (1). AD can be a challenge to treat, and off-label systemic treatments may be contraindicated, ineffective or induce adverse effects. Dupilumab, a new treatment recently approved in Europe for patients with moderate to severe AD, has shown promising results in clinical trials (3). Dupilumab is a human monoclonal antibody that inhibits interleukin (IL)-4 and IL-13 signalling through blockade of the shared IL-4α subunit (4). There are limited data on the efficacy and safety when switching from conventional systemic treatment to dupilumab and on long-term follow-up. We report here a case series of 10 patients with severe, long-lasting AD treated with dupilumab, in whom adverse events concerning the eyes were frequent.
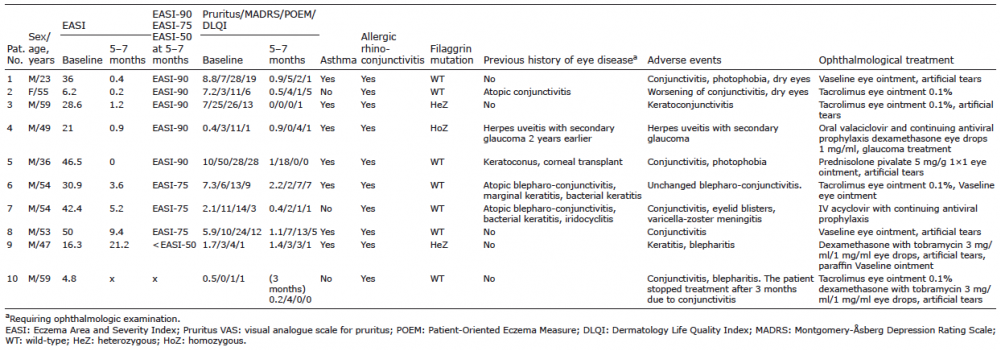
The study included a total of 10 patients (1 woman, 9 men; age range 23–59 years) with severe AD who were being treated with dupilumab (Dupixent®, Sanofi-Aventis Groupe, Paris, France) (Table I). All participants had a history of asthma and/or allergic rhinoconjunctivitis and 3 had filaggrin mutations. All had been given systemic treatment on and off for at least 4 years. Some had tried more than one systemic treatment (MTX, cyclosporine, azathioprine or psoralen plus ultraviolet A (PUVA)) due to lack of response and/or adverse effects. All had been given periodic UV treatment. Six of 10 patients had been on MTX, and 3 of 10 had been on cyclosporine before switching to dupilumab. The patients were also given concomitant topical therapy (glucocorticoids, calcineurin inhibitors, moisturizers).
Baseline values were assessed after a washout period of at least 2 weeks for the previous systemic treatment. The patients started with a loading dose of 600 mg dupilumab injected subcutaneously, followed by biweekly injections of 300 mg. Topical therapy was continued during washout and subsequently.
The following variables were monitored during dupilumab thera-py: Eczema Area and Severity Index (EASI) (5), visual analogue scale for pruritus (10 cm VAS), Montgomery-Åsberg Depression Rating Scale (MADRS) (6), Patient-Oriented Eczema Measure (POEM) (5) and Dermatology Life Quality Index (DLQI) (7). The reductions in EASI scores after 1, 3 and 5–7 months of treatment were expressed in terms of EASI-90, EASI-75 and EASI-50, i.e. reduction in EASI with 90%, 75% or 50%, respectively. Clinical evaluation also included blood chemistry and monitoring of adverse events. The patients were recommended to use prophylactic Vaseline eye ointment daily (Oculentum simplex®) due to the risk of developing conjunctivitis, as reported in clinical trials with dupilumab (4). All 10 patients were seen by an ophthalmologist during the treatment.
Table I. Characteristics of patients with severe atopic dermatitis treated with dupilumab
EASI. The mean score at baseline was 20.7 (range 4.8–46.5). At 1 month, 1 of 10 patients showed complete clearance of skin lesions. At 3 months, 2 of 10 patients showed complete clearance, 4 patients achieved EASI-90, and 2 patients achieved EASI-75. However, one of the cleared patients decided to stop dupilumab treatment at this time due to severe discomfort from conjunctivitis (patient number 10). After 5–7 months, 5 of the remaining 9 patients achieved EASI-90 and 3 achieved EASI-75 (see Table I). However, one patient (number 9) did not achieve EASI-50.
VAS for pruritus. The baseline mean score on the VAS was 5.1 (range 0.4–10.0). Mean scores and ranges at 3 and 5–7 months were 0.9 (range 0.1–3.8) and 0.9 (range 0–2.2), respectively.
MADRS. The mean baseline MADRS score was 11.8 (range 0–50.0). Mean scores and ranges at 3 and 5–7 months were 4.9 (range 0–14.0) and 4.6 (range 0–18.0), respectively.
POEM and DLQI. The POEM score was reduced by more than 4 points at 5–7 months in 8 of 9 patients and the DLQI score by more than 4 points in 4 of 9, i.e. minimal clinically important differences were achieved for these variables (8, 9). For detailed information, see Fig. 1.
Adverse events. These are summarized in Table I. Ophthalmological manifestations were found to be common adverse events. Artificial tears and/or Vaseline eye ointment (Oculentum simplex®) alone did not alleviate the symptoms and discomfort; one patient even stopped dupilumab due to severe discomfort from conjunctivitis (patient number 10). Therefore, all patients were seen by an ophthalmologist. Seven of 10 patients were diagnosed with conjunctivitis. Six patients showed some improvement after local treatment with tacrolimus 0.1% ointment applied daily on the border of the eyelid and/or with glucocorticoid eye drops. One patient developed uveitis due to reactivation of herpes simplex virus (HSV) and received dexamethasone eye drops and topical antiviral therapy. He had had an episode of herpes uveitis 2 years previously. Another patient developed blisters on the eyelid and, 2 days later, was diagnosed with PCR-confirmed varicella-zoster virus (VZV) meningitis. The patient was hospitalized and received intravenous acyclovir treatment. Both these patients recovered completely. Dupilumab treatment did not need to be discontinued, but concomitant antiviral prophylaxis was added.
Fig. 1. Outcome variables monitored during dupilumab treatment of 10 adults with atopic dermatitis. (A) Eczema Area Severity Index (EASI) (missing data for patient number 9 at 1 month). (B) Pruritus Visual Analogue Scale Score (VAS, 0–10 cm) (missing data for patient numbers 1, 3 and 9 at 1 month). (C) Montgomery-Åsberg Depression Rating Scale (MADRS). (D) Patient-Oriented Eczema Measure (POEM) (missing data for patient numbers 1, 3 and 9 at 1 month). (E) Dermatology Life Quality Index (DLQI) (missing data for patient numbers 1, 3 and 9 at 1 month).
Dupilumab treatment improved eczema and MADRS in the majority of patients, while DLQI was improved in most patients. However, one patient, interestingly with a filaggrin mutation, did not improve. The reason is unknown, but it is possible that the patient was a late responder, or the phenotype with extensive head and neck dermatitis is more difficult to treat, or that compliance failed. The patient remains on dupilumab and is being followed closely. One patient discontinued dupilumab due to severe conjunctivitis, but the treatment was not withdrawn in any other patients.
In all, 9 of 10 patients had eye problems (blepharitis, conjunctivitis, uveitis, keratitis) requiring examination and treatment by an ophthalmologist. The incidence of conjunctivitis in our case series was 70%, which is much higher than expected. In clinical trials, conjunctivitis has been reported in only a minority of patients (5–28%) (10, 11). In line with a recent report, conjunctivitis in dupilumab-treated patients may be alleviated with tacrolimus ointment and/or glucocorticoid eye drops (11). Severe long-lasting AD or coexisting allergic conjunctivitis are reported to be associated with increased risk of conjunctivitis during dupilumab treatment (12, 13), whereas this has not been reported in asthma and nasal polyposis dupilumab trials (10). The reason for this difference is unknown.
Other notable adverse events were recurrence of HSV uveitis and VZV meningitis. Modification of immunological signal pathways may interfere with defence against viral infections, as has been described in patients with rheumatoid arthritis and ulcerative colitis treated with JAK inhibitors (14). Interestingly, IL-4/IL-13 signalling pathways are linked to downstream JAK inhibition (15).
Although the current case series is very small and perhaps not representative, we conclude that dupilumab can be considered a safe and effective treatment option in severe AD, but that the risk of adverse events from the eyes and recurrence of herpes virus infections should be kept in mind. Therefore, we recommend close collaboration with an ophthalmologist for early diagnosis and intervention in case of eye complications. This is especially warranted among patients with severe, long-lasting AD and/or previous eye disease.


 Click to show fullsize
Click to show fullsize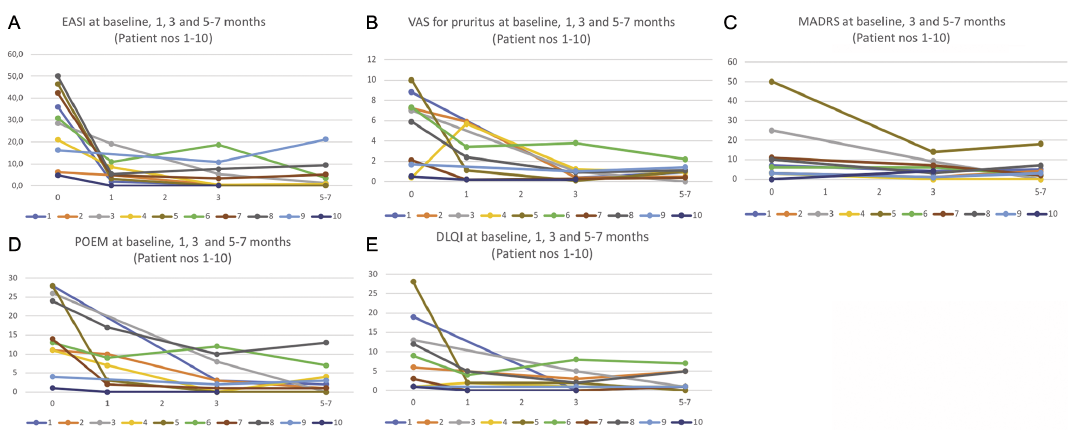 Click to show fullsize
Click to show fullsize