


1Department of Dermatology, University of Montpellier and INSERM U1058, and 2Department of Radiotherapy, Montpellier Cancer Institute, Montpellier, France
Optimal doses of total skin electron beam therapy for mycosis fungoides remain to be established. Clinical efficiency and adverse effects of middle-dose (25 Gy) vs. low-dose (10–12 Gy) total skin electron beam therapy were retrospectively compared in a series of 14 and 12 mycosis fungoides, respectively. Overall skin response rate was 96.2% (92.9% middle-dose and 100% low-dose; not significant (NS)). Overall complete and partial skin response rates were 57.7% (42.9% middle-dose and 75% low-dose; NS) and 38.5% (50% middle-dose and 25% low-dose; NS), respectively. All responding patients relapsed after an overall median time of 5 months (7 months middle-dose vs. 4 months low-dose; p = 0.164, NS). Tolerance was equally fair in both groups, with only grade 1 and 2 adverse events observed in 100% vs. 66.7% of patients in middle-dose and low-dose groups (NS). Although no significant difference was observed, middle-dose protocol may be recommended owing to a longer relapse-free survival for a similar tolerance.
Key words: total skin electron beam therapy; middle dose; low dose; mycosis fungoides.
Accepted Jan 16, 2019; E-published Jan 17, 2019
Acta Derm Venereol 2019; XX: XX–XX.
Corr: Olivier Dereure, Department of Dermatology, Saint-Eloi Hospital, University of Montpellier and INSERM U1058, 80 avenue Augustin Fliche, Montpellier Cedex 5, France. E-mail: o-dereure@chu-montpellier.fr
Mycosis fungoides, the most frequent primary cutaneous lymphoma, can be treated with total skin electron beam therapy, usually advocated as a second- or third-line treat-ment. However, the optimum dose protocol remains to be established. This study indirectly compared 2 dosages (low- and middle-dose) in a retrospective series. A response was obtained in almost all patients regardless of the dosage, but all responding patients relapsed after a relatively short delay. Tolerance was fair for both protocols. As relapse-free survival was almost twice as long in the middle-dose protocol compared with the low-dose, this might be the best choice for management of mycosis fungoides. However, because middle-dose total skin electron beam therapy, unlike low-dose, can be repeated only once during a patient’s disease course, maintenance treatment should be investigated in this setting.
Treatment options in mycosis fungoides (MF), the most common primary cutaneous T-cell lymphoma, mostly depend on disease stage according to 2017 European Organization for Research and Treatment of Cancer (EORTC) staging and the International Society for Cutaneous Lymphomas (ISCL) classification (1). Therapeutic recommendations have been issued recently by EORTC and clearly separate hierarchized strategies used in early (IA–IIA) vs. advanced (IIB–IVB) stages. Total skin electron beam therapy (TSEBT) has long been used in early stages of the disease and may result in complete or nearly complete and protracted response in some patients and appears as a 2nd- or 3rd-line treatment after topical steroids, topical chemotherapy with mechlorethamine and phototherapy in the 2017 EORTC recommendations. Furthermore, it may also be used as a palliative procedure in more advanced stages, although the response rates and duration are less favourable. The most commonly used TSEBT technique is the Stanford 6-dual-field protocol using a conventional 30–36 Gy dose over an 8- to 10-week period. Despite this relatively high dose, relapses are not infrequent, but further irradiation is limited by the potential risk of cumulative radiation toxicity, resulting in TSEBT rarely being administered more than twice, and most commonly once during the disease course (2). To overcome this difficulty, protocols using lower doses (10–12 Gy) have been advocated recently, with similar efficiency compared with the standard dose, but with fewer side-effects. Moreover, this innovative strategy is theoretically consistent with multiple treatment sessions (3, 4). However, middle- and long-term data regarding skin response outcome are often limited precluding an accurate evaluation of the relevance of low doses in a chronic disease for which relapse occurrence and time to relapse are crucial issues. To gain more insight into this issue, a retrospective study was conducted to evaluate the benefit/risk ratio on skin response of middle-dose (25 Gy) vs. low-dose (10–12 Gy) TSEBT in a series of patients with MF treated in the same academic tertiary referral centre over a 20-year period. Relapse areas and possible predictive factors related to response achievement and duration were also investigated.
All patients over 18 years old with a biopsy-confirmed MF and treated in our institution with 25-Gy (middle-dose group) or 10–12 Gy (low-dose group) TSEBT between 1997 and 2017 were included. Files were retrieved from the records of both the Department of Dermatology of Montpellier University and the Department of Radiotherapy of Montpellier Cancer Institute, the facility where the irradiation was implemented. Patients were staged upon treatment initiation using the standard TNMB-classification system based on the clinical type and the extent of skin lesions (T-stage) and the presence of lymph nodes, blood and/or visceral involvement (NMB-stage) (disease staging was retrospective for patients treated before 2007). In all cases the following baseline data were also retrieved from files: sex, patient’s age at TSEBT implementation, number and nature of prior lines of treatment(s), elapsed time between confirmed MF diagnosis and TSEBT initiation, histological subtype of MF (merely classical vs. at least partially folliculotropic MF) and overall duration of follow-up after TSEBT completion.
TSEBT was adapted from the 6-dual-field classical Stanford technique and used a CGR Saturne linear accelerator that provided a 6 MeV electron beam directed to the patient lying on a bed. The patient was installed in 4 different positions during treatment: dorsal decubitus, ventral decubitus, right lateral decubitus and left lateral decubitus. Lead shields were used to protect the eyes. Dose uniformity distribution was verified using an anthropomorphic radiological phantom. All patients were treated in the same facility using the same accelerator and the same treatment protocol (except for total dosage) and dosage choice was based only on time-related data and not on disease severity (i.e. patients treated before 2014 received middle dose, whereas patients treated between 2014 and 2017 received low dose).
All patients in the middle-dose group received a total dose of 25 Gy delivered 3 times a week in fractions of 1 Gy for a total of 25 sessions during an overall period of 8–9 weeks. Patients in the low-dose group received a total of 10 or 12 Gy in fractions of 1 Gy during an overall period of 3–4 weeks.
All concomitant systemic treatments were discontinued during TSEBT regardless of dosage to avoid radiosensitization and until initial response evaluation, but patients may occasionally use superpotent or potent topical steroids. In order to allow a more accurate appraisal of the genuine effect of TSEBT itself, especially regarding response duration, no systemic treatment was resumed or introduced to maintain the response in patients experiencing complete response (CR) or partial response (PR), but superpotent or potent topical steroids were used on a regular basis along with moisturizing creams and ointments.
The primary endpoint was the initial skin response rate, as clinically evaluated by the treating physician at least 2 months after treatment completion. Initial skin response was evaluated using modified Severity Weighted Assessment Tool (mSWAT) scoring change for patients treated after 2008, according to the publication introducing this objective evaluation tool based on total body involved surface and clinical subtype (patches, plaques or tumours) of lesions (5); for these patients, CR, PR and absence of response (NR) were defined as 95–100%, 50–95%, and less than 50% score improvement, respectively. For patients treated until 2008, initial skin response was rated as complete (total or almost total clearance of lesions), partial (clearance of the majority of lesions, but not total or almost total disappearance) or unsatisfying, considered as a failure (no response at all or minor response), using a pragmatic response classification. Secondary endpoints included the relapse rate in responding patients, the median relapse-free survival (in months) defined as the time interval between initial response achievement (CR or PR) and recurrent disease and treatment-related safety data based on the Common Terminology Criteria for Adverse Events. Actuarial Kaplan–Meier relapse-free survival curves were built for responding based on overall and dose-specific data. Response evaluation on non-cutaneous targets (mainly lymph nodes or blood if applicable) was beyond the primary purpose of this retrospective study, which focused on skin response.
Baseline characteristics of patients, initial clinical response, outcome and safety data were compared between middle- and low-dose TSEBT groups using Mann–Whitney test, when appropriate, for quantitative data and Fisher’s exact test for categorical data. In an attempt to identify predictive parameters possibly related to initial clinical response and outcome (response rates and response duration), early-stage (IA to IIA) vs. advanced-stage (IIB to IVA) patients and folliculotropic vs. classical, non-folliculotropic MF were also compared using Mann–Whitney test or Fisher’s exact test. Actuarial relapse-free survival curves were compared using the log-rank test between the different cohorts.
Overall, 26 patients were retrospectively included, 14 in the middle-dose cohort and 12 treated with low doses. All patients in the middle-dose cohort were male and the median age was 66 years (range 39–88). Disease stage distribution at the time of TSEBT was 7 early diseases (2 IA, 4 IB, 1 IIA) and 7 advanced diseases (4 IIB, 2 IIIB, 1 IVA2); folliculotropism was present in 4 cases. Median time from confirmed MF diagnosis to TSEBT initiation was 5 years (range 1–14). All patients had received several other treatments prior to TSEBT, with a median number of 3.5 previous therapeutic lines per patient (range 1–5). In all but 4 middle-dose patients initial skin response was evaluated using mSWAT score variation. In the low-dose group, M/F sex ratio was 8/4 and median age was 71 years (range 31–84). Disease stage distribution at the time of TSEBT initiation included 8 early diseases (7 IB, 1 IIA) and 4 advanced diseases (2 IIB, 1 IIIA, 1 IVA2); folliculotropism was identified in 3 patients. Median elapsed time from confirmed MF diagnosis to TSEBT initiation was 9.5 years (range 1–27). All patients had received several other lines of treatment prior to TSEBT, with a median of 3 previous therapies per patient (range 1–8). Initial skin response was evaluated using mSWAT score variation in all low-dose patients. Initial demographic and staging data, along with details of prior therapies, are summarized in Table SI for both dosage subsets.
Baseline characteristics of middle- and low-dose groups were similar overall, with no significant difference regarding age (p = 1.000, Mann–Whitney test), elapsed time between diagnosis and TSEBT implementation (p = 0.052, Mann–Whitney test), presence of folliculotropism (p = 0.073, Fisher’s exact test) and the total number of prior lines of treatment (p = 0.124, Mann–Whitney). Conversely, sex distribution was different between the 2 groups. Median post-TSEBT follow-up was 3 years (range 1–6 years) in the middle-dose group vs. 2 years (range 0–3 years) in the low-dose subset, and the difference was statistically significantly (p = 0.008, Mann–Whitney test).
In the middle-dose group, all patients received a total dose of 25 Gy delivered 3 times a week in fractions of 1 Gy, as initially planned. In the low-dose group, 10 patients received 10 Gy vs. 12 Gy for 2 patients (median dose 10 Gy); the dose was delivered 3 times a week in fractions of 1 Gy, as initially planned. As already stated, all concomitant systemic treatments were discontinued during TSEBT to avoid radiosensitization and until initial response evaluation.
Among the 14 patients who received middle-dose TSEBT, CR and PR were observed in 6 (42.9%) and 7 (50%) patients, respectively, for an overall response (OR) rate of 92.9% (13/14). One patient (7.1%) with advanced disease showed no significant response. No progression was observed. No significant difference was identified between early-stage and advanced-stage patients as for overall (7/7 (100%) vs. 6/7 (85.7%); p = 0.286 Fisher’s exact test), complete (2/7 (28.6%) vs. 4/7 (57.1%); p = 0.592) and partial (5/7 (71.4%) vs. 2/7 (28.6%); p = 0.286) response rates, even though the CR/PR ratio was surprisingly higher in advanced vs. early stages among responding patients (2 vs. 0.4). Overall, a higher percentage of responding patients experienced CR vs. PR in IA patients compared with IB patients (75% vs. 50%), but the difference was not significant (Fisher’s exact test; p = 1.000). During follow-up, a clinical relapse was observed in all (14/14) responding patients after a median relapse-free survival of 7 months (range 1–36 months; interquartile range (IQR) 3.75–9.75). Median relapse-free survival was slightly shorter in advanced (6 months; range 2–36 months; IQR 4.5–9.5) vs. early stages (9 months; range 1–18 months; IQR 4.75–11.25), but the difference did not reach statistical significance (p = 0.700, Mann–Whitney test). On another hand, the median relapse-free survival duration was not significantly different for CR and PR patients (p = 0.474, Mann–Whitney). In line with percentage analysis, the log-rank test applied to actuarial relapse-free survival curves identified no statistical difference between early-stage and advanced-stage patients regarding the onset and timing of recurrence (Fig. 1).
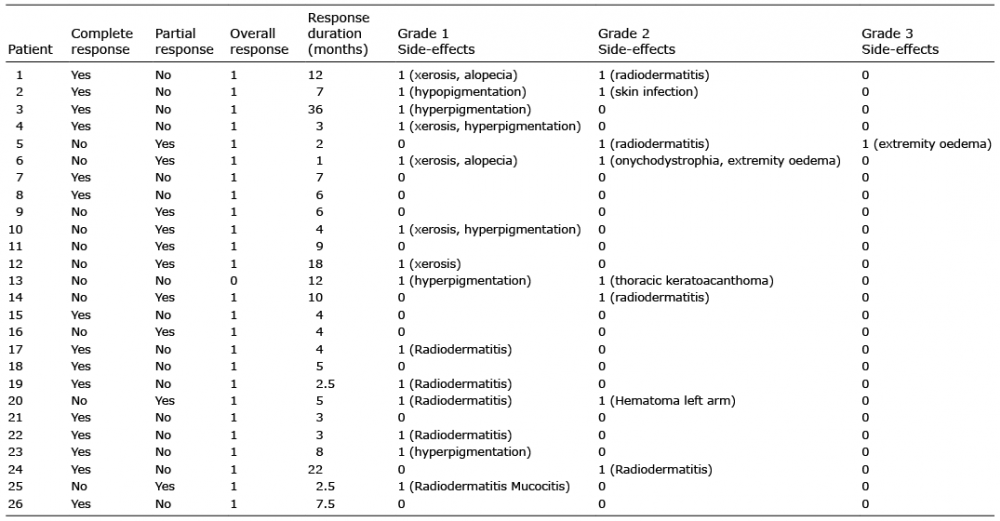
Table I. Clinical response, outcome and safety data
Fig. 1. Actuarial curve of relapse-free survival of patients with early- vs. advanced-stage mycosis fungoides treated with middle-dose total skin electron beam therapy.
In 12 patients from the low-dose group, overall response rate was 100%, with CR and PR observed in 9 (75%) and 3 (25%) patients, respectively. All CR but one were obtained in early-stage patients, whereas all PR were achieved in stage IIB or more (2 IIB and 1 IVA2). In this subset, CR rate was significantly higher for early-stage compared with late-stage patients (8/8 (100%) vs. 1/4 (25%); p = 0.018, Fisher’s test). A clinical relapse was observed in all (12/12) responding patients after a median relapse-free survival of 4 months (range 2.5–22 months; IQR 3–5.6). As for middle-dose TSEBT, median relapse-free survival was slightly shorter in advanced (3.5 months; range 2.5–5 months; IQR 2.8–4.25) vs. early stage (4.5 months; range 2.5–22 months; IQR 3.75–7.6), but the difference did not reach statistical significance (p = 0199, Mann–Whitney test) as confirmed by log-rank test applied to actuarial relapse-free survival curves in early- vs. advanced-stage patients (p = 0.184 (Fig. 2)). The median relapse-free survival duration was also not significantly different for CR and PR patients (p = 0.574, Mann–Whitney test).
Fig. 2. Actuarial curve of relapse-free survival of patients with early- vs. advanced-stage mycosis fungoides treated with low-dose total skin electron beam therapy.
When comparing initial TSEBT efficiency and response outcome depending on delivered dose, statistical analysis did not show any significant difference regarding initial response rates (OR 92.9% vs. 100%, p = 1.00; CR 42.9% vs. 75%, p = 0.248; PR 50% vs. 75%; p = 0.411; Fisher’s exact test), frequency of relapse (100% of responding patients in each dose subset) and median relapse-free survival regardless of disease stage (7 vs. 4 months; p = 0.164, Mann–Whitney test). Actuarial curves of relapse-free survival according to TSEBT dose are depicted in Fig. 3, taking in account overall and dose-specific results. In line with raw figures analysis the log-rank test identified no statistical difference between the 2 doses as to onset and timing of recurrence (p = 0.149).
Fig. 3. Actuarial curve of relapse-free survival of patients with mycosis fungoides treated with middle-dose vs. low-dose total skin electron beam therapy.
Regarding the influence of possibly predictive markers of efficiency on response rates and duration regardless of TBEST dose, overall analysis did not identify a significant difference between early-stage and advanced-stage patients as for overall (100% vs. 90.9%; p = 0.423 Fisher’s exact test), complete (66.7% vs. 50%; p = 0.226 Fisher’s exact test) and partial (33.3% vs. 50%; p = 0.226 Fisher’s exact test) response rates. Median relapse-free survival was overall slightly shorter in advanced (5 months; range 2–36; 4–9.75) vs. early stages (7 months; range 1–22; 4–9.5), but the difference did not reach statistical significance either (p = 0.277, Mann–Whitney test) and log-rank test applied to relapse-free survival curves confirmed this data, p = 0.739 (Fig. 4). Similarly, no significant difference was observed between folliculotropic and non-folliculotropic MF as for overall (100% vs. 94.7%; p = 1, Fisher’s exact test), complete (57.1% vs. 55.5%; p = 1, Fisher’s exact test) and partial (42.9% vs. 38.9%; p = 1, Fisher’s exact test) response rates. Conversely, a strong tendency was identified regarding a longer median response duration in folliculotropic (9 months; range 4–36; IQR 4.5–20) vs. non-folliculotropic MF (4.5 months; range 1–12; IQR 3–7) (p = 0.052, Mann–Whitney test) and the log-rank test applied to relapse-free survival curves confirmed that this difference reached statistical significance using this approach (p = 0.028) (Fig. 5).
The cutaneous sites of relapse were diverse and no statistically significant over-representation of a specific location was identified, despite the theoretically lower dose received by some areas owing to greater skin thickness or difficult-to-treat regions, such as axilla, groin or soles.
Fig. 4. Actuarial curve of relapse-free survival of patients with early- (IA–IIA) vs. advanced- (IIB–IVA) stage mycosis fungoides with total skin electron beam therapy – induced response.
Fig. 5. Actuarial curve of relapse-free survival of patients with folliculotropic vs. non-folliculotropic mycosis fungoides with total skin electron beam therapy – induced response.
Tolerance was overall good, with a total rate/middle-dose specific rate/low dose specific rate of 53.8%/57.1%/50% grade 1 adverse events (AE), 30.8%/42.8%/16.7% grade 2 AE, and 3.8%/7.1/0% grade 3 AE. No grade 4 AE was recorded. The most common treatment-related AE were transient and sometimes painful radiation dermatitis (erythema, desquamation and blistering), most often spontaneously improving in 2–4 weeks with topical moisturizers and subsequent hyperpigmentation. There was no significant difference regarding overall incidence of side-effects between middle- vs. low-dose TSEBT (p = 1 for grade 1–2 and p = 1 for grade 3, Fisher’s exact test). AE are listed in Table I. None of these AE was limiting nor resulted in premature termination of TSBET with reduced total dose as a consequence. One patient treated with 25 Gy developed a keratoacanthoma on the chest 9 months after TSEBT completion, but the specific relationship with TSEBT remains dubious owing to the prior use of both psoralen plus ultraviolet A (PUVA) and narrow-band ultraviolet B (NB UVB) for MF treatment.
Comparison of initial clinical efficiency, response outcome and benefit/risk ratio of middle-dose (25 Gy) vs. low-dose (10–12 Gy) TBEST in patients with MF has not been reported previously. No significant advantage regarding initial efficiency (OR rate and achievement of CR vs. PR), response outcome or safety was identified depending on whether one dose or another was used in our series, but the percentage of patients with advanced disease achieving CR was higher with the 25-Gy dose. Furthermore, median time to relapse was nearly twice as long in the middle-dose group (7 vs. 4 months) al-though the difference did not reach statistical significance (p = 0.164), perhaps owing to the limited size of the sample and the related lack of robustness. This difference could not be explained by an excess of advanced stages, nor by a higher number of prior therapies in low-dose subset, but the influence of a longer elapsed time between MF diagnosis and TBEST (5 years for middle-dose vs. 9.5 years for low-dose) in patients receiving a low dose cannot be ruled out. In addition, rather surprisingly, clinical performance appears to be similar regardless of disease stage in both dose subsets.
A direct comparison of our results with literature data is complex, owing to the heterogeneity of procedures, patients’ characteristics and administered doses. More particularly, no study has specifically investigated the benefit/risk ratio of middle-dose TBEST.
Fourteen series evaluating the results of standard, high-dose TBEST in MF were reported between 1985 and 2014 (3, 4, 6–17), all of them using the 6-dual field technique and including between 40 and 180 patients. Most surveys only mention overall response, with no specific report of CR or PR, and disease stages is not always specified; furthermore, adverse effects are not described, except in one report (13). In these reports, the response rate was quite variable, rated between 44% and 98%. More specifically, a response was obtained in 86% to 98% of stage I–II patients vs. 100% in our patients receiving low-doses and 92.9% for those receiving middle-doses. For advanced stages, overall response rate (ORR) was comprised between 44% (T3) (9) and 83% (T3) (11) vs. 85.7% (6/7) for stages IIB–IVA patients treated by middle-dose TBEST in our survey. On the other hand, median response duration appears to vary widely in high-dose TBEST, ranging from 4 months (4) to 49.3 months (range 26–60 months) (12) vs. 7 months (range 1–36 months) for middle-dose in our series. Accordingly, middle-dose TBEST as used in our patients seems to result in initial clinical control rate comparable to higher doses; however, it cannot be ruled out that response duration might be shorter, but a direct comparison is not relevant on account of methodological discrepancies. On the other hand, comparison of safety data is of limited relevance as well, owing to limited data from high-dose TBEST reports, but it should be noted that middle-dose tolerance was fair in our series. Compared with standard, high-dose procedures, previous reports of middle-dose TBEST in MF are rare. Elsayad et al. (18) used a median dose of 20 Gy (range 12–28 Gy) in 12 stage IB–IVB patients, with an overall response of 71% and a median relapse-free survival of only 3 months vs. 92.9% and 7 months in our middle-dose group. Overall, 25 Gy-dose TBEST thus seems to offer a valuable alternative to high doses with a favourable benefit/risk ratio. Moreover, a second TBEST is theoretically possible in case of relapse after a protracted response.
More recently, low-dose TSEBT (4–10 Gy) has been proposed in MF and supported by a number of reports (19–26). Three of these are prospective studies and 4 are retrospective for a total of 286 patients. All of them reported consistent response rates close to 90% (range 71–95% vs. 100% in our series) and a median CR rate of 27% (range 16–70% vs. 72.7% in our study). When response outcome was specified, all responding patients relapsed (Table SII) after a median relapse-free survival of 8.8 months (range 2.7–16.3 vs. 4 months in our survey). This less favourable result regarding response duration in our patients compared with literature data might be explained by their older age (median age 71 vs. 63 years in prior reports) and a higher percentage of patients with advanced diseases (33.3%) although median relapse-free survival was very close in patients with early- and advanced-stage disease in our survey (4.5 vs. 3.5 months).
A retrospective study by Agar et al. (27) attempted to determine independent predictive factors regarding overall survival and the risk of disease progression in MF and identified disease stage, male sex, advanced age, elevated lactate dehydrogenase, and the presence of a folliculotropic component, as unfavourable parameters. Few studies, however, have sought to determine which clinical or histological markers may specifically portend TSEBT efficiency. In our 26 patients no significant difference was observed regarding initial TSEBT efficacy or relapse-free survival according to disease stage (IA–IIA vs. IIB–IV) regardless of the dose, even though median RFS appeared to be longer in early (9 months) vs. advanced (6 months) stages in patients treated with 25 Gy (p = 0.700, NS). As to histological subgroups (folliculotropic vs. non folliculotropic MF) no significant difference was observed as to response rates and CR achievement, but median relapse-free survival was longer in folliculotropic MF with a trend to statistical significance (9 (range 4–36 months) vs. 4.5 months (range 1–12 months); p = 0.052). It is doubtful that this more protracted result might be related to younger age in folliculotropic MF (median age 63 vs. 71 years); conversely, a deep infiltrate might be a particularly amenable target for accelerated electrons that partially deliver their energy to sites lower than superficial dermis.
As already mentioned, TSEBT-related side-effects are seldom clearly described in reports. Desai et al. (28) investigated the relationship between frequency and nature of cutaneous side-effects (radiodermatitis and its grade, partial or complete alopecia, onychodystrophy, onycholysis or bullous lesions) and the administered dose (comprised between 10 and 36 Gy), Interestingly, 100% of patients experienced partial or complete alopecia and 38% complete onycholysis with the 36 Gy dose. Onychodystrophy was noted for 48% of the patients from doses of 20 Gy and upwards. These side-effects engaging body appearance may explain the absence of female patients in our 25-Gy subgroup, compared with 33.3% women in the low-dose population. The presence of tumours or erythroderma increases the risk of cutaneous ulcerations during TSEBT (29, 30). Repeated or multiple treatments (PUVA, TSEBT or chemotherapy) may increase the risk of skin carcinoma (31), and it is interesting to note that one of our patients developed a keratoacanthoma at the end of TBEST even though a direct causal relationship is unlikely for timing reasons.
TBEST compares favourably with other first-line therapies currently recommended in MF by EORTC guidelines, owing to a favourable benefit/risk ratio with high response rates associated with a relatively low toxicity and middle-dose procedure appears to be of particular interest in this perspective (1). Indeed, the ORR was evaluated at 58.5% and 70% for mechlorethamine 0.02% gel (32) and PUVA, respectively (1), in early-stage MF with a median duration of response of 5 months for the latter treatment. Similarly, low-dose methotrexate (15–25 mg/week) is credited with an OR of 55% (22% CR, 33% PR) with a 15-month median duration of response (33). On account on the high rate of relapse following initial response obtained with TBEST and the relatively short median relapse-free survival regardless of total dose, subsequent, post-TBEST use of a systemic therapy as a response maintenance strategy after frontline successful TSEBT might be of interest. Few trials have studied the possible benefits of such a systemic maintenance therapy after initial response obtained by a frontline treatment and only one for TBEST specifically. Wilson et al. investigated such a strategy after CR obtained by extracorporeal photochemotherapy or doxorubicin/cyclophosphamide polychemotherapy (8); no clear effect was observed on overall or relapse-free survival, although this study might have lacked sufficient robustness. In a trial by Quiros et al. (13), patients received PUVA during 3–6 months 2 months after completion of a 36-Gy TSEBT with no influence on 5-year survival, but with a few months’ increase in median disease-free survival.
Recent reports on low doses (10–12 Gy) have restored the interest in TSEBT owing to a favourable benefit/risk ratio and the potential opportunity of re-treatment. In accordance with the current study, 25 Gy doses may be an even more interesting compromise regarding skin response. Further larger-scale and prospective studies are warranted to further establish the most adequate protocol. In addition, combined strategies using post-TSEBT maintenance therapies should be investigated to circumvent the main shortcoming of TSEBT, i.e. a high relapse rate and a relatively short response duration in most patients.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize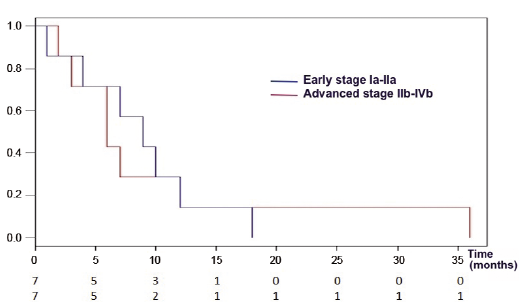 Click to show fullsize
Click to show fullsize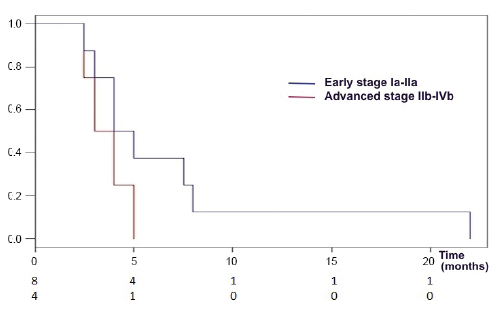 Click to show fullsize
Click to show fullsize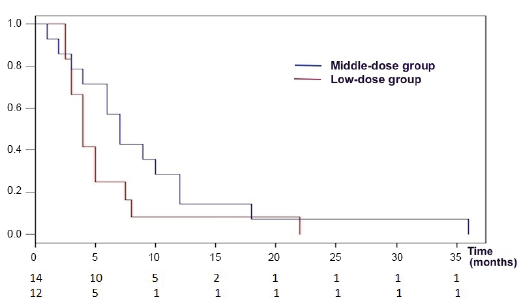 Click to show fullsize
Click to show fullsize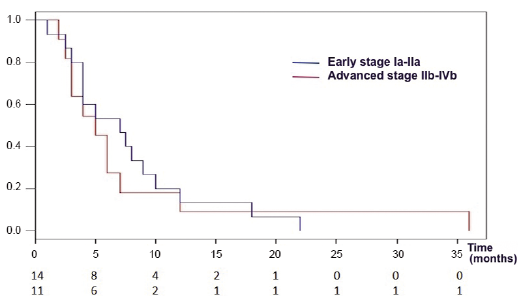 Click to show fullsize
Click to show fullsize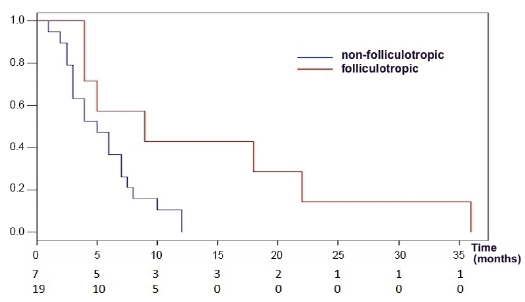 Click to show fullsize
Click to show fullsize