


1Department of Clinical Social Medicine, University Hospital Heidelberg, Heidelberg, and 2Department of Nephrology, DKD Helios Clinic, Wiesbaden, Germany
The GEHIS (German Epidemiological Hemodialysis Itch Study) is a representative cohort study started in 2013 with 860 haemodialysis (HD) patients in 25 German dialysis units. Chronic itch (CI) has been reported to be a poor prognostic marker for patients on HD; how-ever, this has not been investigated in a representative patient cohort. In 2017, all HD patients were contacted again to investigate mortality in those with and with-out CI and to identify its determinants. Patients’ characteristics, study instruments and CI were assessed, as in 2013. The response rate was 84.2% (n = 724). One-year mortality was 15.3%. Mortality was significantly higher in those with secondary scratch lesions compared with those with non-affected skin. This was also true after controlling for age and sex in a multivariate model. This study demonstrates a high mortality in HD patients; however, mortality depends on itch intensity, not on the occurrence of CI itself.
Key words: epidemiology; GEHIS; haemodialysis; itch; mortality; pruritus; uraemic itch.
Accepted Jan 23, 2019; E-published Jan 23, 2019
Acta Derm Venereol 2019; XX: XX–XX.
Corr: Elke Weisshaar, Department of Clinical Social Medicine, Occupational and Environmental Dermatology, University Hospital Heidelberg, Voßstr. 2, DE-69115 Heidelberg, Germany. E-mail: elke.weisshaar@med.uni-heidelberg.de
The German Epidemiological Hemodialysis Itch Study investigated chronic itch and associated factors in patients on haemodialysis. In 2013, 860 patients from 25 German dialysis units were included in the study. In 2017 the same haemodialysis patients were investigated again. During the observation period 48.1% of the haemodialysis patients had died. Mortality was significantly higher in those with secondary scratch lesions compared with those with chronic itch in normal-looking skin, which means that those with scratch lesions on the skin were more prone to die. Chronic itch itself was not associated with earlier death. Dermatologists should pay close attention to haemodialysis patients with chronic itch who have severe scratch lesions on the skin.
End-stage renal disease (ESRD)-associated itch, also called uraemic or renal itch, remains a challenge in daily clinical practice, in dermatology as well as in other fields of medicine. Due to lack of knowledge about the underlying pathophysiology of chronic itch (CI) in haemodialysis (HD), effective treatment modalities are lacking (1). To close this gap, we launched the German Epidemiological Hemodialysis Itch Study (GEHIS) in 2013 (2). In our first analyses, CI and associated factors were assessed using 3 different prevalence measures, showing that 25.2% (point prevalence) were affected by CI (2). Additional analyses of GEHIS investigated the role of, for example, haemodialysis characteristics and comorbidities (3), severity of CI and its clinical picture on the skin (4), health-related quality of life (HRQOL) (5) and the role of medications, such as loop diuretics (6).
In 1991, it was reported for the first time that renal itch is an indicator of poor outcome, and later that the mortality of HD patients may be influenced by the presence of itch (7–9). This appears to be influenced by sleep disturbance. Another study reported a 22% higher mortality rate in patients with moderate to extreme pruritus. A 2-fold increase in risk of mortality was shown in HD patients in the self-assessed “poor sleep” quality group compared with the “good sleep” group (10). However, in these studies severity and duration of itch were not clearly defined in terms of being, for example, acute or chronic (6 weeks and longer), or these studies were performed in non-representative patient populations. The aims of the follow-up study presented here were to report the mortality rate of HD patients with and without CI. Particular attention was paid to the presence and characteristics of CI and to the occurrence of sleep disturbances on the mortality of HD patients.
GEHIS was designed as a prospective cohort study and all baseline data were assessed in 2013. The study design and demographic characteristics of the included patients have been reported in detail elsewhere (2). GEHIS includes 860 HD patients from 25 dialysis units, which were selected randomly from a cluster-sample reflecting the regional distribution of dialysis units throughout Germany. The follow-up study was approved by the ethics committee of the University of Heidelberg (S-670/2016) and conducted in accordance with the World Medical Association’s Declaration of Helsinki (11). The results are reported in line with the “Strengthening the Reporting of Observational Studies in Epidemiology (STROBE)” recommendations (12).
All patients who had participated in GEHIS and had agreed to be contacted again were followed-up in their dialysis unit in 2017 by a research fellow or a dermatologist of the Department of Clinical Social Medicine, University of Heidelberg. For all patients who were not contacted in person or who refused participation, data on the reason for non-participation was collected (e.g. transplantation or change of dialysis unit). In deceased patients all available data on the aetiology of death were extracted from the medical charts. Patient’s information and a consent sheet were handed out at the beginning of the dialysis session. The questionnaires were subsequently distributed to all patients who had agreed to participate in the follow-up. If the patient reported experiencing CI (6 weeks and longer) at the time of questioning, or during the last year, an itch-specific questionnaire was handed out and a full-body skin examination was offered. The clinical picture of CI was classified according to the International Forum for the Study of Itch (IFSI) classification into: (i) pruritus on diseased skin, (ii) pruritus on non-inflamed skin, and (iii) pruritus with chronic secondary scratch lesions including chronic prurigo (13).
The same validated patient-reported outcome (PRO) instruments that were used in the GEHIS 2013 study were used in the follow-up (2). Sociodemographic data were assessed, including current occupational and marital status, general health, hygiene, physical activity, atopic diseases, as well as quality and duration of sleep by self-report. The Short Form 12 (SF-12), (measuring the generic quality of life in physical and mental subscales) (14) and the Hospital Anxiety and Depression scale (HADS) (15) were assessed. CI was assessed for duration and frequency, course, localization and further characteristics of CI. The intensity of itch was assessed on a visual analogue scale (VAS) ranging from 0 (no itch) to 10 (worst imaginable itch) (16). Itch-specific quality of life was measured with the ItchyQoL, which assesses impairments according to the domains of symptoms, functioning, emotions and self-efficacy (17).
The following variables were extracted from the patients’ medical charts: laboratory results (parathormone, urea, creatinine, calcium, phosphate, potassium, sodium, alkaline phosphatase, C-reactive protein (CRP), haemoglobin, transaminases, gamma-GT, serum albumin), dialysis characteristics (Kt/V, duration, membrane, type of membrane flux), medication and concomitant diseases according to the Charlson comorbidity scale adapted to ESRD (3, 18).
Questback Enterprise Feedback Suite Survey Summer Release 2017 was used for data entry. All statistical analyses were performed using SPSS (IBM, version 25) for Windows. We report descriptive data using means together with the standard deviation (SD) as well as absolute and relative frequencies together with 95% confidence intervals (95% CI). Group differences were assessed using Chi-square or Fisher’s exact test for categorical data. Differences in interval scaled data were assessed using t-test. p-values < 0.05 were considered significant, in situations where multiple testing was performed p-values were adjusted conservatively according to the Bonferroni method (19).
Univariate and multivariate logistic regressions models controlling for age and sex were calculated to identify potential factors associated with mortality. Finally, those factors were all included into 2 multivariate Cox proportional hazard models in order to estimate survival over time: (i) by total age and (ii) for time since start of dialysis. The intensity of itch was classified into “no pruritus” (VAS = 0), “mild pruritus” (0<VAS<4), “moderate pruritus” (4≤VAS<7) and “(very) severe pruritus” (VAS≥7) (16). Itch-specific variables (intensity or classification of pruritus) were not included in the above-mentioned model, because they strongly reduce sample size (only patients with CI at inclusion are available). Therefore a multivariate model was run for those variables, controlling for age and sex only.
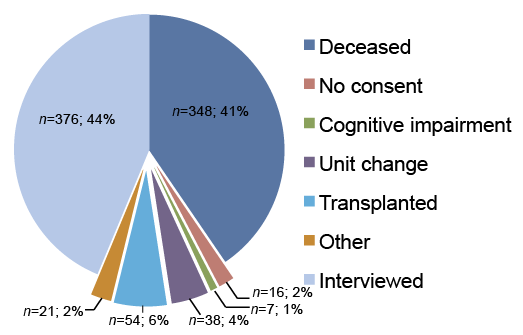
Out of 860 patients investigated in 2013, 724 were followed-up in 2017, resulting in a response rate of 84.2%. A total of 136 patients could not be followed-up for the following reasons: the major reason for non-participation was kidney transplantation (n = 54), change in the dialysis unit (n = 38). and cognitive impairment, such as dementia (n = 7). A small number of patients (n = 16) declined to participate because of, for example, feeling unwell. Twenty-one patients were not addressed for “other reasons”; mainly because they were hospitalized at the time of investigation (Fig. 1).
The mean ± SD age of the patients at baseline in 2013 (n = 724) was 68.6 ± 12.8 years, and 56.5% of the sample were males. Those who could not be followed-up (n = 136) were significantly younger at baseline in 2013 compared with those followed-up (59.3 ± 14.8 years). This was caused mainly by the group of transplanted patients who had a mean ± SD age of 53.6 ± 10.8 years. There were no significant differences in sex between those who were followed-up and those who were not followed-up.
Fig. 1. Overview of sampling results from the German Epidemiological Hemodialysis Itch Study (GEHIS) follow-up (n = 860).
Overall 348 patients (48.1%) had died since 2013; the 1-year mortality rate was 15.3%. Survivors were significantly younger at baseline (64.7 ± 13.6 years) compared with deceased patients (73.6 ± 9.7 years). Consequently, the number of retired or widowed patients was lower in this group. All demographic details of survivors and deceased patients are given in Table I.
Table I. Demographic characteristics of surviving and deceased haemodialysis patients
In Table II the survival rates are shown, together with age at death and time on HD treatment according to the aetiology of HD and comorbidities assessed. Since tests were performed for 20 comorbidities, the p-value was conservatively adjusted according to Bonferroni to p < 0.002 for all analysis concerning comorbidities. Mortality depended on the cause of the ESRD; patients with a hereditary renal disease had the highest survival rate, followed by the ones with primary chronic glomerulonephritis. ESRD due to secondary glomerulonephritis entailed the highest mortality risk.
Table II. Survival rates, age at death and duration in haemodialysis patients according to the aetiology of end-stage renal disease (ESRD) and comorbidities
The mean ± SD age of death was 75.7 ± 9.7 years. Only patients with liver disease showed a significantly younger age at death (68.7 ± 10.6 years). Survival rates were significantly lower in patients with peripheral vascular disease (PVD) (32.9%), myocardial infarction (34.1%), diabetes mellitus (DM; 41.8%) and chronic lung diseases (43.4%). For PVD and DM this was also true after controlling for age. For congestive heart failure and DM a significantly shorter time on HD treatment until death was found; this was also true after controlling for age.
There was no significant difference in survival rates in patients with CI compared with those without. It was even slightly increased (54.6%) in comparison with non-CI patients. However, mortality was associated with the mean itch intensity on VAS. Patients who reported moderate to severe itch intensity had higher mortality rates (RR=1.2; p < 0.02) compared with those with no itch or mild itch. However, this was no longer true after controlling for age and sex in a multivariate model. Patients with mild itch intensity showed slightly lower mortality rate compared with patients with no CI, albeit not significant. Mortality rates depending on the itch intensity measured by VAS and categorized according to (16) are shown in Fig. 2. Patients with CI who had chronic secondary scratch lesions and chronic prurigo (group III) showed significantly increased mortality; this was also true after controlling for age and sex in a multivariate model (Fig. 2).
Fig. 2. Mortality rates of the German Epidemiological Hemodialysis Itch Study (GEHIS) cohort (n = 724) according to the occurrence of chronic itch and (a) its intensity and (b) according to the clinical IFSI classification of itch (n refer to patients who underwent clinical examination of the skin).
A better physical health state (Physical Component Score; PCS) at baseline was reported according to SF-12 in survivors (PCS 38.9 ± 10.1) compared with deceased patients (PCS 32.1 ± 9.9). No differences were found on the mental health scale (Mental Component Score; MCS) of the SF-12. However, a significantly higher depression score on the HADS was found at baseline in the deceased (HADS-D 6.3 ± 4.2) compared with the survivors (HADS-D 4.9 ± 4.1), although no differences were found on the anxiety scale. Laboratory HD parameters for survivors and deceased patients are shown in Table III. Because of multiple testing the p-value was set to p < 0.004 for all analysis of those parameters. Survivors showed significantly higher serum creatinine levels (8.5 ± 2.9 mg/dl), while CRP was higher in deceased patients (1.6 ± 2.2 mg/dl). No significant differences were found in all other parameters including time since onset of dialysis, hours of HD per week, and sleep quality, as well as sleep duration.
All variables that showed a univariate significant association with mortality were included in a multivariate Cox regression model. For increasing serum creatinine values assessed at baseline a decreased risk of dying (RR=0.89; p < 0.001) was found, while higher CRP values were associated with increased mortality risk (RR=1.07; p > 0.05). The risk for patients to die since dialysis started was 1.7-fold for patients with PVD (RR=1.68; p < 0.007). While univariate significant associations were found, there was no significant effect any longer for lung diseases or arterial obstructive diseases on survival in the multivariate Cox regression model on total life expectancy.
Table III. Haemodialysis (HD) parameters at baseline for survivors and deceased patients
This follow-up study demonstrated a high mortality in HD patients. The study investigated whether this mortality is influenced by the occurrence of CI. No influence was found, but the study showed that those HD patients with secondary scratch lesions on the skin (IFSI clinical III) had a higher mortality. In addition, the study showed that those HD patients who also had peripheral vascular disease (PVD) or secondary glomerulonephritis as the underlying disease causing ESRD and leading to HD had the highest mortality. PVD and the laboratory values for creatinine and CRP were the only significant predictors for mortality in a multivariate model. The strengths of the current study are the high follow-up rate of 84.2% and the representative study design (2).
Despite medical progress, the life expectation of ESRD patients on haemodialytic therapy is much lower than that of their counterparts in the general population (20). The 1-year mortality rate of 15.3% found in the current study is comparable to previous reports (21, 22). The Dialysis Outcome and Pattern Study (DOPPS) showed that the crude 1-year mortality rate in the European centres was 15.6% (23). It was reported that the mortality of HD patients may be influenced by the presence of itch. DOPPS revealed that the mortality risk of patients with moderate to extreme pruritus is increased by 17% in comparison with those without itch. However, this effect was no longer statistically significant when adjusted for sleep variables suggesting that elevated mortality rate in HD patients with itch may be explained by sleep disturbance (8). However, itch may be the primary cause of sleep disturbance, and thus related to increased mortality. It was reported that higher intensity of itch was associated with poor sleep quality (9). A tendency for increased mortality was found in HD patients with severe CI; however, no association with sleep quality or duration was found. In the current study, survival was lower in HD patients with less than secondary education. Interestingly, no survival advantage was found for women, as observed in a previous study (24). This may be due to various reasons. Women have been found to be less likely to be listed for transplantation and to receive less transplantation DOPPS (25).
Mortality rates were found to be significantly higher in patients with PVD. Others also reported that the presence of arteriosclerotic diseases decreased the cumulative 4-year probability of survival in HD patients from 73% to 53% (26). The results of the current study show that patients with concomitant liver disease had a significantly younger age at death (mean ±SD 68.7 ± 10.6 years). Increased mortality rate of ESRD patients with concurrent liver cirrhosis was observed previously in Korean patients. Those patients had also higher liver-related mortality and were a mean of approximately 4 years younger at the time of the enrollment (27). This may be because those patients have many comorbidities, which can increase the risk of death. The current study again showed significantly higher serum values of creatinine (3), being a waste product of muscle-turnover, as a direct indicator of the muscle mass and energy house-hold in mammals. Its production in catabolic states is diminished. Since a mutual dependence exists between muscle mass and body mass index (BMI), this finding is in line with the results of several other studies, one quoted here, which have found that higher BMI values in HD patients correlate with lower relative mortality rates (28). When investigating the question of whether CRP is associated with the prevalence of CI the current study did not find any significant differences between HD patients with and without CI (3). However, the results of this follow-up study confirm the results of other studies, that elevated CRP values are predictive for mortality, as found previously in Japanese HD patients (29, 30) and HD patients from other countries (31). Our study did not confirm the findings of other studies on high levels of serum albumin or haemoglobin, which were shown to correlate positively with survival (32). Bone mineral parameters (parathyroid hormone (PTH), phosphate) also did not influence survival in our cohort, which does not correspond with other findings (33). Kt/V-values overall met the international standards and its value was more than 1 in both the deceased and the surviving patients. It has been noticed that Kt/V above 1 does not confer any survival advantage. From the laboratory values considered in the current study, only CRP and serum creatinine were more predictive for mortality than the PCS of SF-12. Interestingly, in the full model, which included multiple laboratory and clinical variables, diabetes was no longer associated with mortality, which corresponds to others. We found a significant association of the PCS of the SF-12 and mortality rates in our study. This corresponds to a previous study that assessed the SF-36 in a 6-month follow-up of HD patients. It predicted mortality, with the physical domain being much lower than assessed in the general population and the scores for mental domain being lower than in the general population, but not so low as in patients with depression (34).
Severely ill patients and those with more comorbidities were more likely to die between the 2013 baseline and the follow-up study; therefore it must be considered that the patients in the follow-up study were overall more healthy and had fewer comorbidities. On the other hand, the age of the patients who could not be addressed in the follow-up study was slightly lower than those who could be addressed, which indicates fewer comorbidities and higher survival for this group.
The authors thank all the HD patients for their participation and all participating haemodialysis units, including their medical doctors and nurses for their support. The authors thank Natalie Plewig for her great help in obtaining and entering the data.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize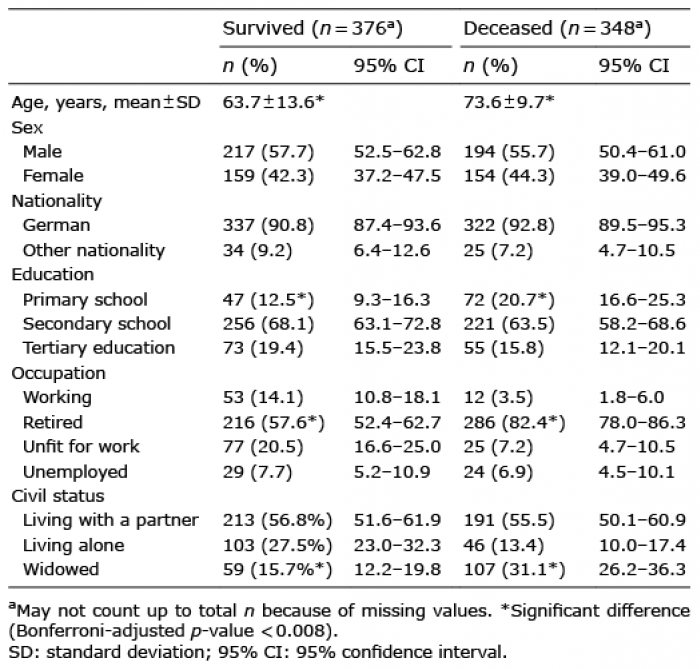 Click to show fullsize
Click to show fullsize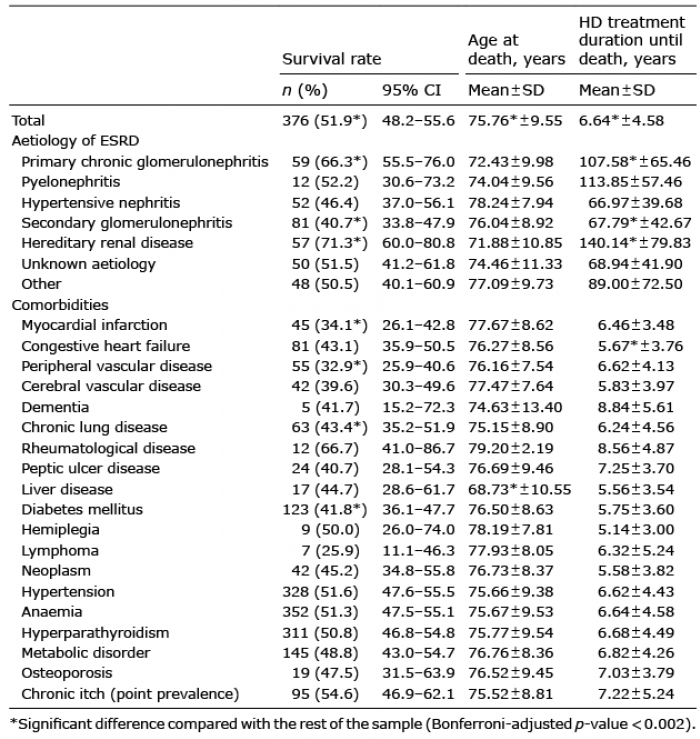 Click to show fullsize
Click to show fullsize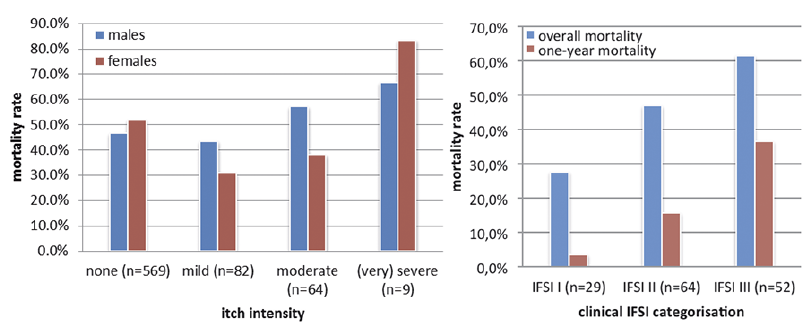 Click to show fullsize
Click to show fullsize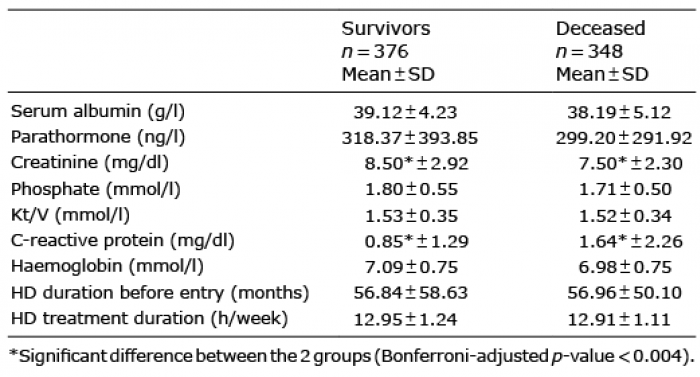 Click to show fullsize
Click to show fullsize