


1Department of Dermatology, University of Groningen, University Medical Centre Groningen, PO Box 30.001, NL-9700 RB Groningen, and 2Department of Dermatology, Meander Medical Centre, Amersfoort, The Netherlands. E-mail: a.l.v.rondags@umcg.nl
Accepted Jan 23, 2019; E-published Jan 23, 2019
Hidradenitis suppurativa (HS) is a chronic, debilitating, inflammatory skin disease that mainly affects body folds (e.g. axillae and groin) (1). Primary lesions include deep-seated inflammatory nodules, abscesses, and sinus tracts (1). The diagnosis of HS can be made easily due to its clear, distinct clinical presentation.
Deckers et al. (2) have reported that patients with HS can score their own disease severity according to the original Hurley classification. However, the purpose of the Hurley classification was to assess HS in a single affected body region in order to guide surgical intervention (3). It was not intended to classify HS disease activity and severity in the whole patient and to assist in extensive treatment plans including, for example, anti-inflammatory options (3, 4).
Therefore, a modification of the Hurley classification was proposed by a Dutch HS expert group in 2017: the “refined Hurley classification” (5). In contrast to the original Hurley classification, the 7-stage refined Hurley classification assesses not only the presence of sinus tracts, but also inflammatory symptoms and the extensiveness of the disease (3, 5). Refined Hurley stages I and II are subdivided into A, B and C, corresponding to mild, moderate and severe disease. Stage III is not subdivided and corresponds to severe HS disease. This was recently confirmed by a construct validation study (6). Furthermore, a comprehensive treatment ladder is added to the flow chart (5).
The aim of this study was to develop and investigate the reliability of a patient self-assessment questionnaire corresponding to the items addressed in the refined Hurley classification, in order to derive the refined Hurley stage.
Consecutive patients with HS were recruited at the dermatology outpatient clinic of the University Medical Centre Groningen (UMCG), a tertiary referral centre for HS. Subjects were eligible if they were diagnosed with HS by a dermatologist, were older than 18 years, and were capable of completing the questionnaire in Dutch.
A patient symptom self-assessment questionnaire was developed by HS experts based on the refined Hurley classification flow chart. Following a pilot study performed with 16 patients (Appendix SI), several modifications were applied to the concept questionnaire. Patients with HS were requested to complete the definitive questionnaire (the refined Hurley classification questionnaire for patients with HS (Appendix SII)) before their regular consultation at the dermatologist. The refined Hurley stage was derived following the flowchart by an investigator (RV) (5). The dermatologists were requested to report a detailed dermatological examination and report the refined Hurley classification, as they also do in daily clinical practice. The percent agreement of data entry between 2 investigators (RV and AR), based on a sample of 10 out of 75 (13.3%) randomly chosen subjects, was 97.2%. No formal sample size calculation can be performed for this type of study. Based on literature on methodology and similar studies in the same field, the aim was to include 75 subjects in the final cohort testing (2, 7). For this type of study, medical ethics committee approval is not required under Dutch law.
Descriptive statistics were used to describe the study population. The inter-rater agreement and reliability between the HS patient’s derived refined Hurley stages and physician’s reported refined Hurley stages were calculated. Next, the inter-rater agreement and reliability of the presence of sinus tracts and HS disease severity, defined by the refined Hurley classification, was calculated. For the inter-rater agreement, percentages of agreement between physicians and patients were calculated manually. Because the refined Hurley classification is a nominal scale, a Krippendorff’s alpha (α) is suitable to determine the inter-rater reliability (8). Statistical analysis was performed using IBM SPSS Statistics 23.0 for Windows (SPSS, Chicago, USA). p-values ≤ 0.05 were considered statistically significant.
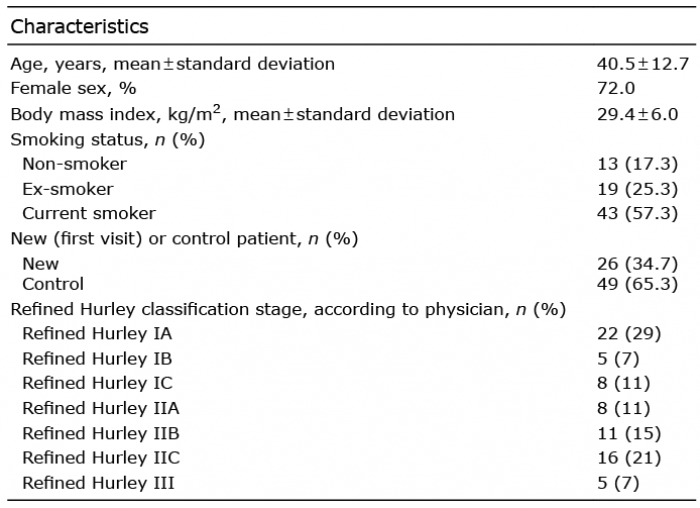
A total of 75 subjects participated in this study. An overview of the patients’ characteristics is shown in Table I. Approximately one-third were patients visiting the dermatology outpatients clinic (UMCG) for the first time.
Table I. Patients’ characteristics (n = 75)
The derived refined Hurley stages and disease severity (based on the refined Hurley classification) from the patient’s answers to the questionnaire vs. the physician’s dermatological examination report are shown in Table SI and Table SII. The inter-rater agreement between patient’s derived and physician’s reported refined Hurley stages was 78.7% (59/75). The inter-rater reliability resulted in an α of 0.737 (95% confidence interval [CI] 0.622–0.852) (Table SIII). Similar results were found for inter-rater agreement and reliability regarding HS disease severity (82.7%, α=0.733 (95% CI 0.589–0.856) (Table SIII). Concerning the assessment of sinus tracts, inter-rater agreement was 89.2% and reliability of α=0.785 (95% CI 0.650–0.919).
In this study, we developed a patient symptom self-assessment questionnaire based on the refined Hurley classification algorithm for HS. We investigated whether the derived refined Hurley stages from the patient questionnaire correspond to the physician’s dermatological examination and given refined Hurley stage. It was found that a substantial inter-rater agreement and reliability, indicating that, in most cases, the same refined Hurley stage could be extracted from the patients’ answers to our questionnaire as assigned by the physician.
Notably, in contrast to the flow chart of the refined Hurley classification, we found in the current study that it is important to first ask patients with HS about the presence of abscesses/inflammatory nodules, prior to the presence of sinus tracts. This might be due to the chronological order in which HS mostly develops: the first signs of HS are usually recurrent inflammatory nodules and/or abscesses, and in a later stage sinus tracts might develop. Furthermore, the reliability of the questionnaire is enhanced by educating the patient about the main HS lesions, by providing a concise description with prototypical pictures of these lesions.
One of the main items in the original as well as in the refined Hurley classification that has to be determined is the presence of sinus tracts. We have shown that the inter-rater agreement and reliability regarding the presence of sinus tracts is especially high. However, as stated previously, the original Hurley classification lacks valuable information to assess symptoms and severity in an entire individual (4). Recently, we have shown that the sub-stages of the refined Hurley classification correlated significantly with patient-reported quality of life and physician-assessed disease severity (6). In the current study we showed that patients and physicians also agree on the level of disease severity.
Furthermore, compared with the study by Deckers et al. (2) and another study (9) regarding self-assessment of disease severity of other skin diseases (acne, psoriasis, and atopic eczema), our results are the highest.
A limitation of the current study is that it was conducted in a single university hospital with HS expertise. This might have biased the results. Patients with HS seen at our department might have a longer duration of disease and are usually extensively informed about their disease. This could indicate that these patients are more familiar with the symptoms of HS than are patients treated in primary and secondary healthcare centres. However, besides inclusion of patients coming for follow-up consultation, new referrals were also included.
In conclusion, the symptom self-assessment questionnaire described here is an accurate instrument for deriving the correct refined Hurley stage within patients with HS and might be useful for daily clinical practice, as well as for future epidemiological and clinical studies in HS. We recommend investigating the usefulness of this questionnaire further in other/multiple treatment centers, including sub-analyses, such as the results of new vs. follow-up patients, presence of inflammatory nodules/abscesses, and involved anatomical region.
The authors are grateful for the participation of all the patients with HS in this study.
Conflict of interests: ICJ reports a research grant from Abbvie. BH reports fees from AbbVie, Novartis, UCB Pharma, Solenne BV and Janssen-Cilag for consultation/advisory, scientific research, congress and courses, and fees from Novartis for consultation/advisory, scientific research and congress outside the submitted work. The other authors have no conflicts of interests to declare.


 Click to show fullsize
Click to show fullsize