


Department of Dermatology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing 100730, PR China. *E-mail: mdonglai@sohu.com
A 27-year-old man presented to the dermatology clinic with an 8-year history of a pedunculated, rubbery soft, pink nodule, 10 mm in diameter, with a verrucous surface, protruding from the right side of the scrotum (Fig. 1). It was first noticed as an asymptomatic small papule and gradually developed in size. He had no known history of sexual transmitted infections or prior genital lesions. The patient’s fasting serum lipid profile was within normal limits. An aceto-whitening test was negative. The patient received a shave biopsy for histopathological analysis (Fig. 2) and immunohistochemical staining. In addition, immunolabelling with a polyclonal antibody to a common human papillomavirus (HPV) capsid antigen was performed.
What is your diagnosis? See next page for answer.
Fig. 1. Pedunculated, rubbery soft, pink nodule, 10 mm in diameter, with a verrucous surface protruding from the right side of the scrotum.
Fig. 2. (A) Hyperkeratosis, focal parakeratin plug, elongation of the rete ridges without atypia and foamy histiocytes filling papillary dermis. (B) Foamy histiocytes filling papillary dermis. (Haematoxylin-eosin stain; original magnification: (A) ×100; (B) ×200).
Acta Derm Venereol 2019; XX: XX–XX.
Diagnosis: Verruciform xanthoma
Histopathological findings revealed hyperkeratosis, focal parakeratin plug, elongation of the rete ridges without atypia and foamy histiocytes filling papillary dermis (Fig. 2). Foamy cells were positive for CD68 immunohistochemical staining. Immunolabelling with a polyclonal antibody to HPV capsid antigen was negative. Based on these findings, the diagnosis of verruciform xanthoma (VX) was made. The patient received a complete surgical excision of the lesion and no recurrence was found after one year of follow-up.
VX is a rare benign neoplasm, the exact aetiology and pathogenesis of which remains unknown. Several hypotheses have been proposed, including HPV infections, bacterial or fungal colonization, cutaneous trauma, local release of lipid by damaged keratinocytes through chronic inflammation, epithelial degeneration due to irritation and lymphedema (1–3).
VX is characterized by a solitary yellowish or reddish asymptomatic lesion with a planar, verrucous, papillary, or granular surface, with or without a pedunculated base. The lesion can be found on the oral mucosa and extraoral location. The most common extraoral location is the anogenital areas, involving the vulva, penis and scrotum (4). VX could also co-exist with other cutaneous disease, including dystrophic epidermolysis bullosa, graft-versus-host disease, lichen sclerosus, discoid lupus erythematosus, pemphigus vulgaris, and congenital hemidysplasia with ichthyosiform erythroderma and limb defects syndrome (5).
Hyperkeratosis, focal parakeratosis, verrucous acanthosis without atypia in the epidermis and xanthoma cells (foam cells) localized within the papillary dermis are diagnostic histopathological findings of VX (6). In contrast to other xanthomas, hyperlipidaemia is not typical in the reported VX cases.
The lesions could be easily misdiagnosed as condyloma acuminatum, a sexually transmitted disease associated with human papilloma virus infection, which is characteristic by being positive in aceto-whitening test and superficial koilocytes in the epidermis histopathologically. Solitary neurofibroma always presents as asymptomatic, solitary nodule and has a predilection for scalp and extremities without family history. Soft fibroma most commonly affects the areas of friction, includes neck, axilla and inguinal regions in elderly, pregnant or obese patients. Therefore, the final diagnosis of VX should be confirmed by the histopathological results.
Excision of small lesions (< 2.0 cm) was curative. Cryo-therapy, carbon dioxide (CO2) laser, radiation therapy, topical steroids and 10% povidone–iodine solution had also been applied to treat VX (7). Joo et al. (4) applied a combined therapeutic approach of shave debulking and fractionated CO2 laser, which resulted in complete resolution of scrotal VX with excellent cosmetic outcomes.


 Click to show fullsize
Click to show fullsize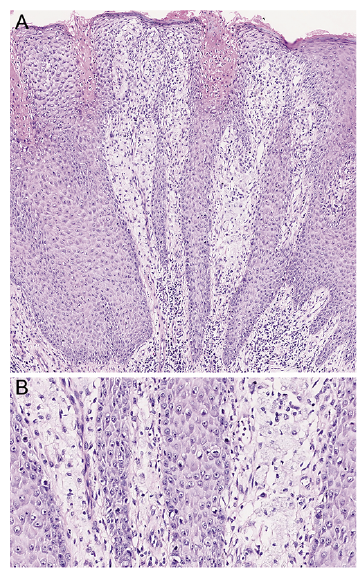 Click to show fullsize
Click to show fullsize