


Department of Dermatology, Osaka Red Cross Hospital, 5-30 Fudegasaki-cho, Tennoji-ku, Osaka 543-8555, Japan. E-mail: tomoski@kuhp.kyoto-u.ac.jp
Accepted Feb 5, 2019; E-published Feb 6, 2019
Psoriasis is a common chronic inflammatory skin disease. The current understanding of the immunopathogenesis and inflammatory cytokine pathways enables us to develop and introduce biological therapies for the treatment of moderate to severe psoriasis (1). Anti-IL-17 (anti-interleukin-17) inhibitors, such as ixekinumab (anti-IL-17A antibody), secukinumab (anti-IL-17A antibody) and brodalumab (anti-IL-17 receptor A (IL-17RA) antibody) exert excellent therapeutic effects on psoriasis. Since IL-17 is an important cytokine for preventing fungal infections, adverse skin reactions such as cutaneous candidiasis are occasionally experienced during the administration of IL-17 inhibitors (2), however little is known about other adverse skin reactions of these inhibitors.
It is known that biologics, such as tumour necrosis factor (TNF) and interleukin (IL)-12/23 (ustekinumab) blockade, can paradoxically induce psoriasiform eruptions (3–5), although the pathogenesis remains unclear (6). As for the IL-17 inhibitors, to our knowledge, there are only two reports of psoriasiform eruptions induced by secukinumab (7, 8) and no reports for ixekizumab and brodalumab.
Here, we report the first case of psoriasiform eruptions induced by ixekizumab.
A 76-year-old man (162 cm, 56 kg) was diagnosed with psoriasis vulgaris over 20 years ago. He had been treated with topical therapies (calcipotriol/betamethasone, clobetasol propionate, and other topical corticosteroids) and narrowband UVB (ultraviolet B) phototherapy; however, the psoriatic lesions were persistent on the elbows, dorsum of the hands, knees and lower limbs.
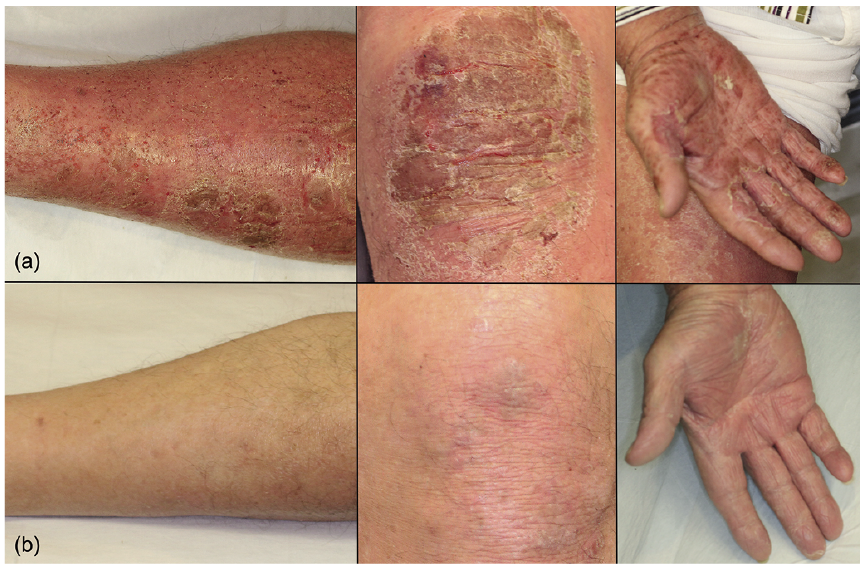
He was treated with ixekizumab (80 mg/2 weeks/body), and by 4 weeks of treatment, the psoriatic lesions disappeared, except on the knees. The fifth dose of ixekizumab was administered 8 weeks after the initiation of treatment, when mild scaly erythema developed on the lower limbs, which was not observed before. Fungal infection was negative in the lesions. Three days later, both erythema and oedema were observed on most of the body including the palms and soles (Fig. 1a), and the body temperature was up to 38.0°C. Because the skin lesions progressed to erythroderma accompanied by thick scales, the sixth dose of ixekizumab was not administered and clobetasol ointment was started. Skin biopsy from the scaly erythema on his left thigh, presented pathological findings compatible with psoriasis (Fig. 2).
Fig. 1. Clinical findings. (a) After the fifth dose of ixekizumab, both erythema and oedema were observed on most of the body, including the palms and soles. (b) Twelve weeks after the last administration of ixekizumab, the skin lesions were mostly resolved. However, the skin lesions on the knees remained. Minimal scary erythema was observed on the knees.
Fig. 2. Histopathological findings. (a) Low-magnification view (×40). Hyperkeratosis with parakeratosis was observed, and the epidermis showed acanthosis with regular elongation of rete ridges. (b) High-magnification view (×100). Neutrophils and lymphocytes infiltrated moderately in superficial dermis, and slight interface change and dilated papillary blood vessels were observed.
Three weeks after the last administration of ixekizumab, the scaly erythema and oedema improved, however, psoriatic lesions were still persistent, especially on palms, soles, and lower limbs. We therefore started oral cyclosporine (150 mg/day) treatment. One week later, these skin lesions gradually improved, and we continued the administration of cyclosporine as the patient refused further biological treatments. Twelve weeks after the last administration of ixekizumab, the skin lesions were mostly resolved. However, the skin lesions on the knees remained. Minimal scary erythema was observed on the knees. (Fig. 1b).
We experienced a case of psoriasiform eruptions that developed during treatment with ixekizumab. Because the psoriasiform eruptions in our patient flared after the administration of ixekizumab and the discontinuation of treatment improved the skin lesions, it is strongly suspected that ixekizumab paradoxically induced the psoriasiform eruptions. Certainly, it is difficult to completely rule out the possibility that ixekizumab induced an acute exacerbation of eczema in a psoriasis patient as the pathogenesis in our case is different from that of a paradoxical psoriasiform eruption induced by TNF-α blocking agents.
The occurrence of psoriasiform eruptions induced by the biologics, mainly TNF-α blocking agents, is known as a paradoxical reaction. The most popular hypothesis is due to the disequilibrium in the cytokine balance. Psoriasis involves 3 major cytokines, TNF-α, IFN type I (interferon type I) and the IL-23/Th17 axis, which are interwoven in the pathogenesis of psoriasis and are linked in a triangular interplay. Thus, targeting one of these cytokines may influence the other two axes (9). In this sense, it is known that TNF-α blocking agents increase the expression of IFN-α, and induce the psoriasiform eruptions (6). Psoriasiform eruptions have also been reported with various other biological agents, such as rituximab (10), abatacept (11), tocilizumab (12), ustekinumab, and IL-17 inhibitors. Their pathogenesis is still unclear, but possibly related to the imbalance in the cytokine pathways like the psoriasiform eruptions that are induced by the TNF-α blocking agents.
Although there are no reports on the paradoxical psoriasiform eruptions induced by IL-17RA antibody, anti-IL-17A antibody-induced psoriasiform eruptions have been reported. IL-17RA antibody, unlike anti-IL-17A antibody, blocks not only IL-17A, but also other members of the IL-17 family. The blockage of IL-17A only, may possibly provoke the activation of the other members of IL-17 families. Indeed, the other members of IL-17 families are considered to possess pro-inflammatory functions (13).
Herein, we report the first case of psoriasiform erup-tion, which was possibly induced by ixekizumab. Clinicians should therefore be aware that anti-IL-17A antibody such as secukinumab and ixekizumab may induce paradoxical psoriasiform eruptions.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize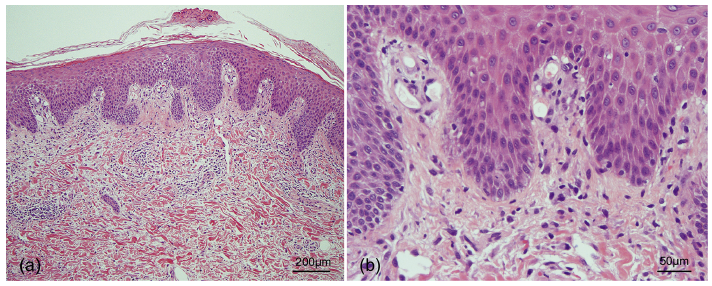 Click to show fullsize
Click to show fullsize