


Royal Randwick Medical Centre, Randwick, Australia
Concerns about topical steroid withdrawal are causing some patients to cease long-term topical corticosteroid therapy, however, little is known about the ensuing clinical outcomes. This qualitative case series studied 10 children whose parents stopped their chronic topical corticosteroid use and subsequently developed features typically reported in adults experiencing topical steroid withdrawal. Patients were seen in an Australian general practice between April 2014 and October 2018, with follow-up periods ranging from 18 months to 4 years. Symptoms were difficult initially for the children and their families, however, all ultimately improved. At the final review, 4 of the children had clear skin and another 4 had symptoms consistent with their original, pre-treatment atopic dermatitis. More research is required into long-term topical corticosteroid use and its discontinuation, including topical steroid withdrawal, particularly in the pediatric population.
Key words: topical steroid withdrawal; red skin syndrome; atopic dermatitis; topical corticosteroids; eczema.
Accepted Feb 7, 2019; E-published Feb 8, 2019
Acta Derm Venereol
Corr: Belinda Sheary, Royal Randwick Medical Centre, 70/73-115 Belmore Road, Randwick NSW 2031, Australia. E-mail: belinda.sheary@ipn.com.au
Topical steroid withdrawal is discussed widely in social media, and some patients with a history of long-term topical steroid use are self-diagnosing this condition. There is little information in medical literature about what happens when chronic topical steroid therapy is stopped, especially in children. This study followed 10 children for between 18 months and 4 years after their parents decided to cease their topical steroid use. The children experienced typical topical steroid withdrawal symptoms for many months, however, all eventually improved.
Concerns about topical steroid withdrawal (TSW) are causing some parents of children with chronic dermatological conditions, particularly atopic dermatitis (AD), to discontinue their child’s long-term topical corticosteroid (TCS) therapy. TSW is a potential adverse effect of TCS overuse (1), most commonly seen in patients with a history of atopy, reporting prolonged TCS overuse, especially where such use has included the face and provided diminishing clinical benefit over time. TSW is widely discussed in social media (1) and with many patients (and parents) researching health issues online (2), discussing TSW is likely to become an increasingly common scenario for prescribers of TCSs (3).
Pediatric cases of TSW have been reported in the literature infrequently (1, 4–6). The incidence and prevalence of TSW is unknown (1, 7) and research is limited (6, 8–13), however, a systematic review (1) suggested TSW in children is uncommon with only 7% of reported cases occurring in patients under 18 years of age. In a recent study (12) examining patients ceasing long-term TCSs and subsequently developing TSW symptoms, 20% (14 out of 69) of patients were children. This paper examines the histories of 10 of those 14 children. They were followed up in a general practice setting for 18 months–4 years.
Little is known about what happens when children cease chronic TCS use. Patients may experience “rebound” symptoms after stopping TCSs (14) and certainly after stopping oral steroids for skin symptoms (15). However, it is not widely accepted there may be withdrawal symptoms associated with TCS discontinuation as it is with other medication (for example, selective serotonin reuptake inhibitors commonly prescribed for depression). This may be because traditionally TCSs have been recommended intermittently for flares of symptoms and long-term frequent use has not been studied. However, in practice there are patients who use TCSs regularly for years – sometimes on a continuous daily basis (12).
Confirming the diagnosis of TSW is problematic, and TSW remains controversial. Accepted diagnostic criteria for TSW do not exist (though recently some have been proposed (12)), and TCS “overuse” has never been defined. Some argue that the symptoms resulting from TCS discontinuation represent an exacerbation of the underlying skin disease, however, there are features typically reported in TSW and not in AD. On ceasing TCSs, a patient with TSW develops widespread red skin (7, 10–11) and itch, in addition to at least some of the following distinctive features: burning pain, excessive skin exfoliation, edema, skin sensitivity (1, 7, 10, 12), ‘red sleeve’ (7, 12) and/or ‘elephant wrinkles’ (12).
This case series examined the histories of patients under the age of 18, who presented to an Australian general practice with concerns about TSW, and whose cases were reported to the Therapeutic Goods Administration (for inclusion in the Australian Adverse Drug Reaction Database) between January 2015 and February 2018. These patients gave histories of increasing amounts and/or potencies of TCSs used over time, and developed typical TSW features following TCS discontinuation. Fourteen patients were identified, and their medical files were reviewed. Written consent was obtained from the parents of the 10 patients presented in this paper. Of the 4 remaining cases, one has already been published as a case report (4), and 3 had recommenced TCS use following presentation to an emergency department (after 10 days, 17 days and 3 months, respectively, of not using TCSs). Two of the children who resumed TCS use were subsequently lost to follow-up; the third remains on continuous daily TCS use 4 years later under the supervision of a pediatric dermatologist. The children described in this series were seen during the period April 2014 – October 2018.
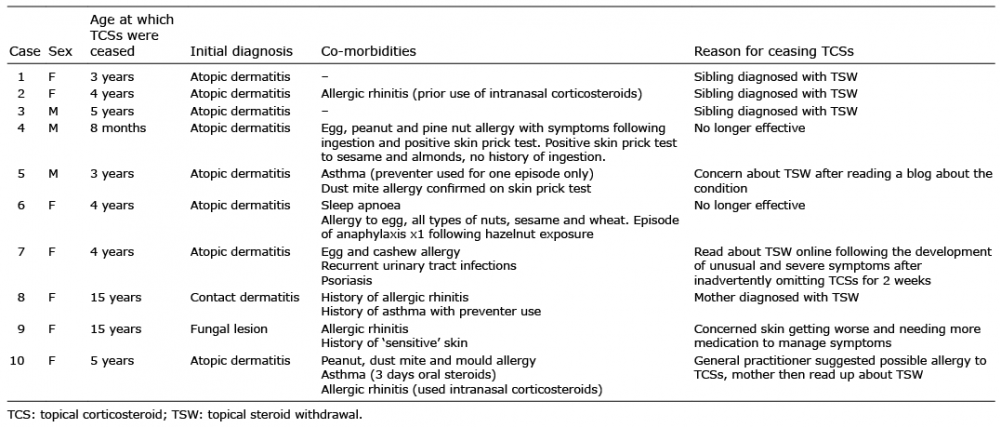
Patient demographics and reasons for ceasing TCSs are listed in Table I, and Table II details the patients’ TCS use histories and other treatments utilised prior to ceasing TCSs. Table III lists the features suggestive of TSW seen in each case, the complications encountered, new co-morbidities diagnosed and management strategies employed.
Table I. Patient details
Table II. Topical corticosteroid (TCS) use history in the 10 cases
Table III. Patient outcomes and management following cessation of topical corticosteroids
When patient 1, aged 3 years, ceased TCSs, areas of redness to her skin spread gradually, with bilateral ‘red sleeve’ apparent 3 months later (Fig. 1). Itch was severe at night and excessive skin shedding was evident on the bed clothes each morning for several months. Oozing areas to her anterior ankles took 8 months to fully clear. Her sleep remained disturbed until 22 months after stopping TCSs. At this point her eczematous areas were limited to her cubital and popliteal fossae – similar to her original, pre-treatment AD. This was still the case when seen 48 months post TCS discontinuation.
Fig. 1. Red sleeve with erythema ending abruptly at the palm in both left and right upper limbs, seen in Case 1, 3 months after cessation of topical corticosteroids.
Patient 2, who was 4 years old, experienced clear skin for 5 months after stopping TCSs – a “honeymoon” period – before AD recurred to her cubital and popliteal fossae. TCS use was not recommenced, and the eczematous areas slowly spread. Eight months after TCS cessation most of her upper and lower limbs were erythematous and she had started to complain of burning pain. Both widespread red skin and burning pain are classic features of TSW. In addition, typical of TSW, the rebound eruption extended to parts of her body where TCSs had never been applied (7). Her skin symptoms peaked in severity around 15 months post TCS discontinuation and then gradually improved; at 29 months her final skin symptom resolved – a stinging sensation with sweating/exercise. 48 months after stopping TCSs her skin was still clear and she reported only occasional mild itch.
Patient 3, aged 5 years, had only mild AD symptoms initially following TCS cessation, however, he developed ‘red sleeve’ 6 months later and subsequently ‘elephant wrinkles’ appeared to his extensor elbows. His symptoms peaked late with oozing to his face present between 16–20 months after stopping TCS therapy. He had increased exfoliation to his face up until the 28 month mark. After this, his symptoms were comparable to his original AD. On examination 48 months after ceasing TCSs, he had eczematous areas limited to his cubital and popliteal fossae.
Patient 4, who was 8 months old at the time, developed red, itchy skin with areas of ooze three days after stopping TCSs. Typical ‘elephant wrinkles’ to his extensor elbows were noted when he was examined 10 months post TCS cessation. Fifteen months after stopping TCSs all oozing areas had cleared, and 3 months later he was sleeping through the night for the first time. Examination at this point revealed eczematous changes to his wrists and ankles only. Cervical and inguinal lymphadenopathy resolved 30 months after discontinuing TCSs, appearing to mark the end of TSW related symptoms. 41 months after TCS cessation he had a small area of eczema behind his right knee.
Aged 3 years, patient 5’s skin symptoms flared 3 days after stopping TCSs, and by the 7th day he had widespread red skin with large areas of ooze. Eight months after ceasing TCSs his symptoms improved significantly and were less severe than before TCS discontinuation. He experienced an exacerbation of skin symptoms in the two winters that followed, with lymphadenopathy present both times. Over the warmer months his skin was normal. Two and a half years after TCS cessation, ‘elephant wrinkles’ were present on his anterior knees.
Three days after ceasing TCSs, patient 6, then 4 years old, developed urticarial lesions to her abdomen, back and areas of her lower limbs where her skin had previously been clear (and TCSs had never been applied). Large areas of skin started oozing and then shedding in alternating cycles. At 22 months post cessation of TCSs enlarged cervical and inguinal lymph nodes were noted. At 27 months she had much larger areas of clear skin, though itch and burning pain remained troublesome overnight. At 36 months her skin had significantly improved. Her mother reported that a lotion she was recommended for her daughter (and subsequently used) at a hydrotherapy centre overseas may have contained undisclosed TCSs.
One week after inadvertently running out of TCSs, 4 year old patient 7 developed redness around her neck – an area never before affected by her AD. The erythema spread to cover her entire body. She complained of burning pain, had difficulty regulating her temperature (felt cold on warm days) and experienced hair loss. She developed ‘elephant wrinkles’ to her anterior knees, in addition to edema to her eyelids, hands and ankles. Her skin cycled between periods of oozing and excessive shedding. Her symptoms became a lot more manageable 9 months after TCS cessation. Twenty-eight months after stopping TCSs, she had small eczematous areas limited to her lower limbs, similar to her original, pre-treatment AD.
Patient 8 was 15 years old when she ceased TCS use. Similar to case 2, she experienced a “honeymoon” period, during which she had clear skin for 4 months. She then developed peri-orbital swelling, burning pain, redness to her face and anterior neck, oozing areas to her cheeks and periods of excessive skin exfoliation. She experienced a break from symptoms 14 months later which lasted for 2 months before her itch, burning pain and insomnia returned. Twenty-one months after stopping TCSs she was diagnosed with a cataract. At 24 months, her skin was normal.
One week after ceasing TCSs, 15 year old patient 9 noticed new areas of redness to her cubital fossae, and a few weeks later developed ‘elephant wrinkles’ to her extensor elbows. She developed excessive skin exfoliation to her face, ears and scalp, and her neck cycled through periods of oozing and skin shedding. Burning pain was difficult to manage and for a time her skin sensitivity meant she could not tolerate bathing. Her final symptom to resolve was discomfort with sweating/exercise. When examined 8 months after TCS cessation her skin was normal, and she reported only occasional pruritus to her left cubital fossa. Her skin remained clear when seen 18 months after stopping TCSs.
Within days of ceasing TCSs, patient 10, aged 4, developed widespread red skin with oozing areas to her hands, knees and feet. Her skin then cycled through periods of excessive exfoliation before again becoming erythematous. Skin sensitivity made bathing painful. Her ankles became edematous, she developed inguinal and post auricular lymphadenopathy and she experienced burning pain, hair loss and temperature dysregulation. Her parents were encouraged to recommence her TCS therapy by her immunologist but did not, and by 18 months post TCS cessation her skin had improved significantly. Twenty-nine months after stopping TCSs her skin was clear.
The demographics and history of these children was not dissimilar to those reported in adult populations where patients ceased long-term TCS therapy and developed TSW features. In a retrospective Australian study (12), 56% of the 55 adult patients were female, 76% had an initial diagnosis of AD, 84% had used TCSs on their face and 42% had taken oral prednisone for their skin symptoms. In this case series 7 of the 10 patients were female, all had a history of atopy, 8 had a history of AD, 8 had used TCSs to their face and 3 reported having taken oral prednisone for skin symptoms. All reported increasing the amount and potency of TCSs they used over time. Five of the children showed evidence of atopic march with asthma subsequently diagnosed in 4 and allergic rhino-conjunctivitis in 2.
Ceasing TCSs in these children resulted in similar symptoms and signs as those reported in adults experiencing TSW, suggesting any diagnostic criteria developed for adults with TSW (12) may also be applicable to pediatric patients. All the patients developed diffusely red skin, and either ‘elephant wrinkles’ or ‘red sleeve’ (or both) were seen in 8 out of 10 children. The headlight sign was seen in one child. Four children developed lymphadenopathy; this was not listed as a reported sign in a systematic review of TSW (1) though it has been described in a pediatric case report (4).
While TSW was considered the most likely diagnosis in these children, confirmation was not possible partly due to the fact diagnostic criteria for TSW did not exist when they were first assessed, and partly due to the inability to completely exclude all differential diagnoses. In particular, allergic contact dermatitis could not be excluded due to poor access to patch testing services. An infectious cause was considered unlikely with children systemically well despite often large areas of erythematous skin in addition to an absence of local signs such as tenderness and warmth (though it is noted that two children were treated for skin infections on several occasions). A flare of the underlying dermatological condition could have been possible, at least in some of the cases, but as time progressed the patients developed symptoms described in TSW and not in AD (that is, burning pain, excessive skin exfoliation, edema, skin sensitivity, ‘red sleeve’ and ‘elephant wrinkles’). Nevertheless, case 4 (seen by an immunologist regarding food allergies), case 5 (seen by his pediatrician) and case 10 (managed by her immunologist) continued to be regarded as having “severe eczema” – differential diagnoses were never entertained. When they subsequently improved it was attributed to their “outgrowing” AD. While traditional teaching did create an expectation for the majority of children to “outgrow” AD (16), how likely this is to occur, particularly in severe cases, is less clear (17–20).
Hajar and colleagues (1) suggested “confluent ery-thema” occurs within “days to weeks” of ceasing TCSs in TSW; however, while typical TSW symptoms occurred in all the children, they were delayed in cases 1–3 and 8. The reason for this was unclear. Did they experience a recurrence of their original skin condition or was it TSW? If it was disease recurrence, why did their new symptoms mimic TSW? Steroid injections negatively impact long term outcomes seen in tennis elbow (21, 22) – could the natural history of AD be similarly affected by TCS use? A common feature in their histories is noted: these children ceased TCSs because a family member was diagnosed with TSW, and not because TCSs had become ineffective for them personally (however, they were requiring increasingly frequent applications of TCSs to manage their skin symptoms.) Their total TCS use is thus likely to be less significant than that used by patients with more commonly described TSW presentations. Research is needed into timelines for patients experiencing TSW with differing TCS use histories.
Management of TSW symptoms in these patients included previously reported symptomatic measures and psychological input, in addition to other therapies. Emollients, over the counter antihistamines, ice packs and hydroxyzine (10) were used with some relief by these children. Alternative treatments utilised included traditional Chinese medicine, dietary changes/supplements and hydrotherapy. One child received monthly IV immunoglobulin infusions for 12 months. Treatments described in the literature not employed by patients in this case series included doxepin (12), gabapentin (11), immunosuppressants (11,12) (particularly cyclosporine), phototherapy (10) and dupilumab (13). In addition, tetracycline antibiotics (1) and calcineurin inhibitors (1) have been used in patients with the papularpustular type of TSW. Tapering TCS use is not generally recommended (7,11) and was not trialled by patients in this case series.
It has been reported at the completion of TSW, patients experience either clear skin or their original eczema symptoms (7). In this case series 4 had clear skin at their last review, and 4 of the remaining 6 children had similar symptoms to their original, pre-treatment dermatitis.
The underlying pathophysiology of TSW is unknown, and a greater understanding in the future may help explain the prolonged nature of the symptoms. While Rapaport & Lebwohl (23) reported durations of TSW symptoms lasting from 1–30 months, a protracted duration is considered implausible by a number of dermatologists (personal communication). TCSs have an anti-inflammatory, immunosuppressive, anti-proliferative and vasoconstrictor action and so it is conceivable a range of molecular changes occur when chronic TCS use is discontinued. Rapaport & Lebwohl proposed the mechanism for widespread erythema following TCS cessation was secondary to the release of accumulated nitric oxide stores causing hyper-dilation of blood vessels (23) (TCSs suppress nitric oxide in the endothelium). Fukaya (24) proposed cortisol production by keratinocytes is suppressed by TCSs and so on cessation of TCSs there is relative cortisol insufficiency giving rise to some of the symptoms seen in TSW. It is possible disturbances at a cellular level – of which there may be several considering the multifactorial mode of action of TCSs – take considerable time to normalise.
In conclusion, parental concerns about TSW may lead to cessation of long-term TCS use in children. While TSW has been more frequently reported in adults, it can occur in children too. Further research into TSW is needed to establish consensus diagnostic criteria and evidence-based management guidelines. A better understanding of TSW will require research into the effects of chronic TCS use and its discontinuation.


 Click to show fullsize
Click to show fullsize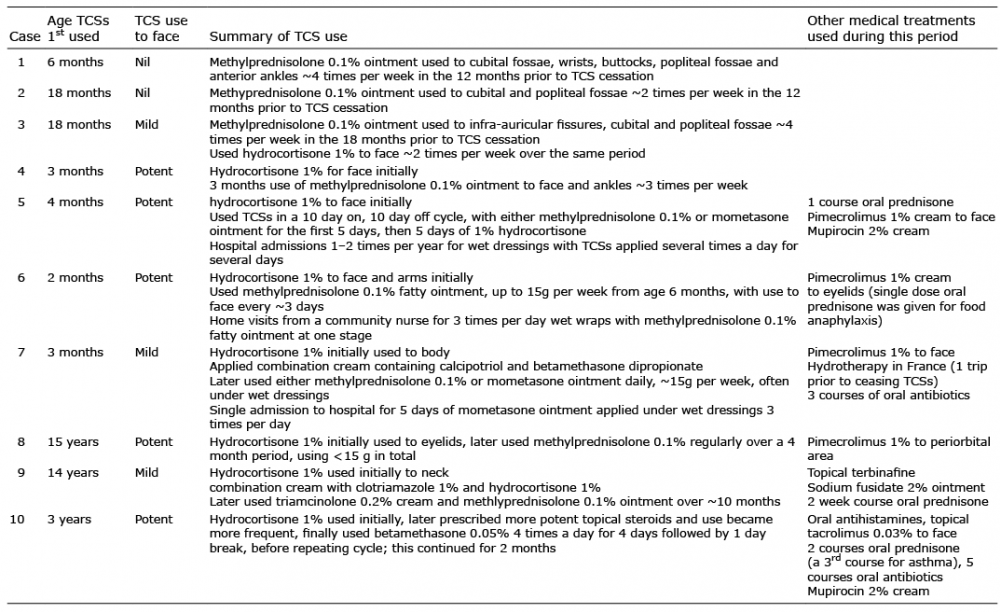 Click to show fullsize
Click to show fullsize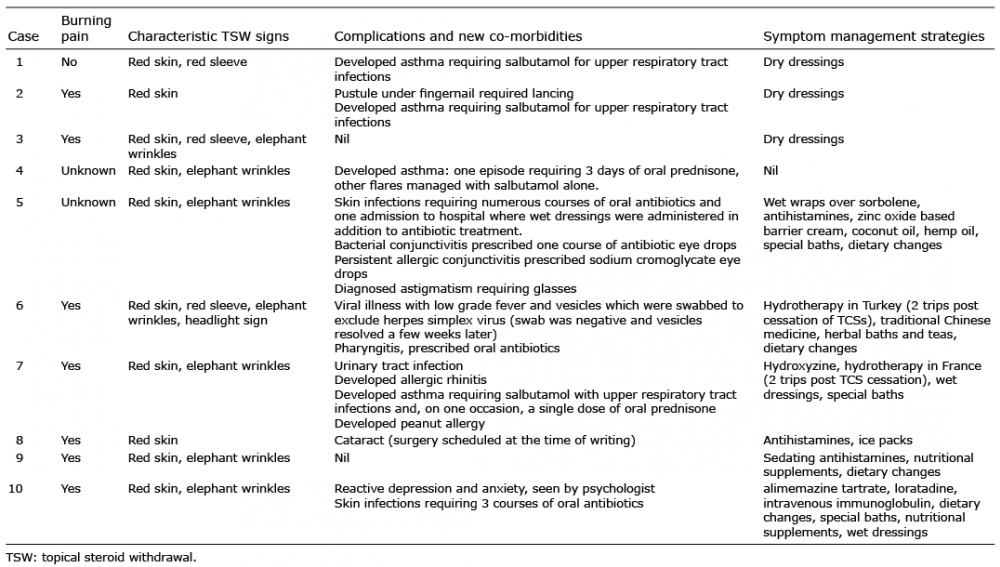 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize