


Department of Dermatology, Venereology and Allergology, Wroclaw Medical University, Wroclaw, Poland
Psoriasis is a chronic inflammatory dermatosis, frequently presenting with chronic itch. This study investigated the prevalence and detailed clinical characteristics of chronic itch in 143 psoriatic patients, with regard to different age groups, comorbidities and pharmacotherapy. Chronic itch was reported by 72% of subjects. Patients aged 65 years and over presented higher 4-Item Itch Questionnaire (4IIQ) scores (8.6 ± 3.4 vs. 7.4 ± 2.5 points; p = 0.03) and rarely experienced itching at midday (p = 0.009). Chronic itch correlated with aspirin intake and xerosis intensity. 4IIQ scores were higher in patients with asthma/chronic obstructive pulmonary disease, peptic ulcer disease and those taking insulin. Logistic regression analysis found that chronic itch was positively correlated with the use of antacids, angiotensin receptor blockers, angiotensin enzyme converting inhibitors, beta-blockers, xerosis intensity and Physician’s Global Assessment score, whereas psychiatric drugs other than selective serotonin reuptake inhibitors, allopurinol, coexistence of arterial hypertension and application of emollients acted conversely. Elderly psoriatic patients present several differences in the characteristics of chronic itch, and chronic itch may be associated with comorbidities and pharmacotherapy. To the best of our knowledge, this is the first study to report possible associations between psoriatic pruritus and co-administration of drugs utilized in various systemic conditions.
Key words: itch; psoriasis; elderly; comorbidities; pharmaco-therapy.
Accepted Feb 7, 2019; E-published Feb 8, 2019
Acta Derm Venereol 2019; XX: XX–XX.
Corr: Jacek Szepietowski, Department of Dermatology, Venereology and Allergology, Wroclaw Medical University, ul. Chalubinskiego 1, PL-50-368, Wroclaw, Poland. E-mail: jacek.szepietowski@umed.wroc.pl
Psoriasis is a chronic inflammatory cutaneous disease frequently encountered in the general population. The majority of psoriatic patients experience chronic itch. The current study has extensively evaluated the prevalence and clinical characteristics of chronic itch in a cohort of psoriatic subjects. Moreover, we have investigated clinical itch-related differences between senior and non-senior groups of patients, as well as possible associations between chronic itch, systemic comorbidities and pharmacotherapy.
Psoriasis is a chronic, inflammatory cutaneous disorder affecting skin, nails and joints, often associated with various comorbidities, and posing a severe psychosocial burden in affected individuals (1, 2). Psoriasis is common in the general population, with an estimated prevalence in the general population of 1–4.4% (3–5). Clinical studies of the elderly population with psoriasis are scarce, al-though it is the 6th most common cutaneous disease in this population (6). Studies have determined the prevalence of psoriasis in elderly patients as 2.2–12.5% (7–9), whereas late onset of psoriasis was observed in approximately 3% of psoriatic individuals (6, 10).
Itch, classically described as an unpleasant feeling urging a desire to scratch (11), is classified as acute or chronic, with the latter being described as lasting 6 weeks or longer (12). Chronic itch (CI) is a frequent complaint, affecting 64–97% of psoriatic individuals, and its clinical characteristics and impact on various quality of life (QoL) domains have been studied extensively (13–17). However, few reports have provided data on itch characteristics and burden among elderly patients with psoriasis (10, 18). In addition, taking into account the abundance of pathogenic factors associated with CI (19), including coexisting systemic disorders and drug intake, this symptom in psoriatic patients may be associated with factors other than the underlying dermatosis, especially in elderly patients. The possible role of other cofactors is supported by the observation that treatment of psoriasis does not necessarily provide relief in pruritus (20).
The aim of the present study was to investigate the prevalence and detailed clinical characteristics of CI in psoriatic patients, as well as QoL and stigmatization aspects, with a particular emphasis on itch-related parameters in relation to different age groups, comorbidities and pharmacotherapy.
This cross-sectional study was conducted between January 2017 and May 2018. Among 176 dermatology inpatients diagnosed with psoriasis vulgaris, 143 (81.3%) agreed to participate in the study. Patients diagnosed with another coexistent cutaneous condition presenting with itch (e.g. urticaria, allergic contact dermatitis, etc.) were excluded. A detailed medical history was obtained, including baseline demographics, systemic comorbidities and systemic drug intake. Dermatological history included the presence of coexisting dermatoses, application of emollients (if positive, the daily frequency was noted) and the time of psoriasis onset. The results of routine laboratory blood tests performed during hospitalization were noted, including concentrations of haemoglobin (Hb; reference range 12–16 g/dl in females, 14–18 g/dl in males), C-reactive protein (CRP; reference range 0.2–5 mg/l), aspartate aminotransferase (ASPAT) (reference range 5–34 U/l), alanine aminotransferase (ALAT) (reference range 0–35 U/l), serum creatinine (reference range 0.73–1.18 mg/dl), and glomerular filtration rate (GFR; assessed by Cockcroft-Gault equation).
Physical examination assessing disease severity was performed using Psoriasis Area Severity Index (PASI; with a score of 0–72 points) (21), body surface area (BSA; percentage of the skin affected by psoriatic lesions; 0–100%) and Physician’s Global Assessment (PGA; 0–4 points). The presence of nail and joint involvement was noted, as well as the clinical type of psoriasis (I vs. II). Clinical assessment of skin xerosis was performed using a 5-point scale (0: no xerosis; 1: mild; 2: moderate; 3: severe; 4: very severe) (22). The occurrence of CI was noted, along with the location affected by the symptom. The detailed characteristics of CI (extensity, severity, frequency, sleep impairment) were assessed via 4-Item Itch Questionnaire (4IIQ) (23–27). In addition, a modified questionnaire for the description of itch (28) was completed in order to determine the presence of itch in the last 3 days; maximal itch intensity in the last 3 days was assessed via a verbal rating scale (VRS; none, mild, moderate, severe, very severe) and a numerical rating scale (NRS; 0=no itch, 10=maximal itch intensity); while an NRS was also used to assess the highest itch intensity during the course of the disease. In addition, data concerning the description of cutaneous sensations associated with itch, emotional burden of itch, sleep impairment, alteration of itch intensity due to specific factors, and impact of itch on psyche were obtained. The measurement of QoL was performed using the Dermatology Life Quality Index (DLQI) questionnaire by Finlay & Khan (29), while the 6-Item Stigmatisation Scale (6ISS) (30) was utilized to assess stigmatization.
The study was approved by the Bioethics Committee of Wroclaw Medical University (KB-124/2018).
From all the data collected (all patients population, n = 143), a subset of CI patients (n = 103) were the subject of further analyses on the detailed parameters of the disease. A total of 158 variables were drawn up, of which only 94 could have been applied to the all-patient population. Descriptive statistics were used to display the variables in age (non-senior/senior) group; and appropriate significance tests (Student’s t-test, χ2 test, Mann–Whitney test) were performed. Subsequently, an extensive correlational analysis was carried out, using Pearson correlation coefficient (cc), Spearman’s rank cc, point-biserial, rank-biserial, and the standardized contingency coefficient (C Pearson), corresponding to the type of variables tested. Finally, a logistic regression for the CI variable (as dependent) was performed, demonstrating the most meaningful impacting factors (independent variables) and their odds ratios (OR). p < 0.05 was assumed to be statistically significant. All calculations were conducted using Statistica 13 (Dell, Inc.) software.
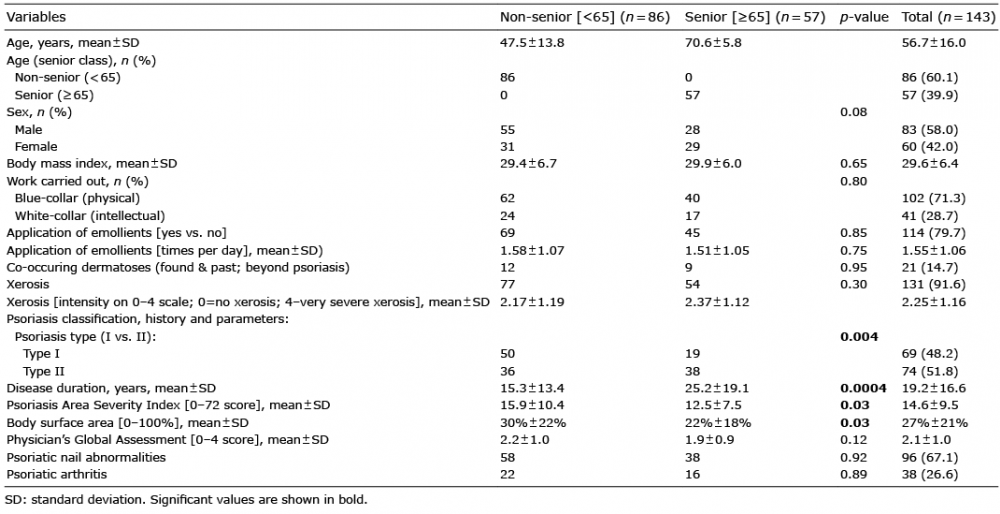
The study included 143 patients; 83 males and 60 females (58% vs 42%). The clinical characteristics of the examined individuals displayed in non-senior (< 65 years) vs. senior (≥ 65 years) groups are listed in Table I. The age of the examined individuals ranged from 19 to 88 years (mean ± standard deviation (SD) 56.7 ± 16.0 years). Fifty-seven subjects (39.9%) were aged 65 years or older. The most common comorbidities included hypertension (44.1%), obesity (44.1%), diabetes mellitus (21.7%), joint diseases (17.5%) and anaemia (14.7%). Basic laboratory evaluation included haemoglobin concentration (mean ± SD 14.1 ± 1.6 g/dl), serum creatinine (0.92 ± 0.86 mg/dl), GFR (106.2 ± 43.1 ml/min), ASPAT (26.2 ± 20.6 U/l), ALAT (28.2 ± 20.2 U/l) and CRP concentration (10.5 ± 21.8 mg/l). The majority of patients used systemic pharmacotherapy (71.2%), with the most common being angiotensin converting enzyme inhibitors (ACEI) and angiotensin receptor blockers (ARB) (32.2%), diuretics (22.4%), calcium-blockers (20.3%), statins (16.8%) and metformin (16.1%). Among antipsoriatic drugs, methotrexate was applied most commonly (5.6%), followed by biological drugs (3.5%), cyclosporine A and acitretin (1.4% each).
Table I. Clinical characteristics of the examined patients in age groups
Nearly 80% of subjects reported daily application of emollients, with the frequency of application 1.55 ± 1.06 times a day. Skin dryness (xerosis) was observed in 91.6% of individuals, whereas the mean level of xerosis was 2.25 ± 1.16 points. The proportion of type I and II psoriasis was similar (48.2% vs. 51.8%). Mean disease duration was 19.2 ± 16.6 years. Regarding disease severity, mean values for PASI, BSA and PGA were 14.6 ± 9.5 points, 27% ± 21%, and 2.1 ± 1.0 points, respectively. Psoriatic nail abnormalities were present in 67.1%, while 26.6% of patients also had psoriatic arthritis.
CI was reported by 72% of examined individuals, with no significant difference between non-senior and senior groups (70.9% vs. 73.7%; p = 0.72). Detailed data concerning CI are listed in Table II. Patients reported that CI was present mostly on the lower limbs (66%), followed by the back (49.5%), upper limbs (47.6%) and head (27.2%). Generalized itch was reported by 17.5% of subjects. In the majority (77.7%) of individuals CI was limited to the pathologically changed skin, while in 22.3% the symptom was present both on pathologically changed and unchanged skin. Ninety-nine percent of patients reported itch during the last 3 days, whereas mean 4IIQ score was 7.9 ± 3.0 points. Single itch episodes lasted for more than 10 min in 45.6% of affected individuals, while 36.9% and 17.5% reported shorter (< 1 and 1–10 min, respectively). In general, patients experienced CI during the evening (92.2%), although the symptom was also common at other times of day (morning 77.7%; midday 74.8%, night 60.2%). Itch severity (VRS) was assessed as moderate by 35.9% of individuals; severe, mild and very severe intensity was reported by 26.2%, 20.4% and 15.5%, respectively. Mean NRS itch intensity during the last 3 days was reported as 5.8 ± 2.3 points (similar to 5.4 ± 2.9 points following a mosquito bite), whereas maximal NRS score during the course of CI was 7.4±2.6 points. Isolated itch sensation was reported by 36.9% of subjects with CI; associated sensations such as burning (36.9%), tingling (23.3%), tweaking (21.4%), and prickling (19.4%) were also noted. Itch was described as irritating (77.7% of patients with CI), burdensome (76.7%), unbearable (51.5%) and worrisome (37.9%). Nearly half of the CI population (47.6%) reported night awakenings, 41.7% reported difficulty falling asleep and 16.5% reported the need to use soporifics. Among factors increasing itch intensity, sweating was mentioned as the most frequent (65% of patients with CI), followed by heat (55.3%), stress (49.5%), hot water (37.9%), diet (32%), physical activity (26.2%), dry air (21.3%), sleep (19.4%), fatigue (13.6%), cold water (4.8%) and cold ambient temperature (3.9%). Conversely, cold water and cold ambient temperature most often provided relief of itch (in 38.8% of patients), followed by sleep (34%), physical activity (28.2%), hot water (21.4%), dry air (16.5%), while fatigue, stress, sweat, heat and diet were of minor importance (4.9%, 3.9%, 2.9%, 0%, respectively). Regarding CI characteristics, the older age group presented higher 4IIQ scores (8.6 ± 3.4 vs. 7.4 ± 2.5 points; p = 0.03, older first) and less frequently reported the presence of itch at midday (p = 0.009).
Table II. Clinical characteristics of chronic itch patients in age groups
Mean QoL score was 8.6 ± 5.9 points (within all-patients population), with no statistically significant difference between the sexes (8.2 ± 5.7 points for males, 9.1 ± 6.2 for females; p = 0.39). Clearly significant difference in DLQI scores was noted when comparing CI group (9.6 ± 5.9 points) with patients free from itch (6.0 ± 5.0 points) (p = 0.0008). Concerning stigmatization, the mean 6ISS score was 3.9 ± 3.5 points and did not differ between the sexes (3.9 ± 3.2 points for males, 4.0 ± 3.9 points in females; p = 0.97) and CI status (3.9 ± 3.4 points in patients free from itch, 3.9 ± 3.5 points for CI patients; p = 0.98).
The presence of CI was positively correlated with aspirin intake (cc = 0.24; p = 0.04), xerosis intensity (cc = 0.31; p = 0.003), BSA (cc = 0.21; p = 0.01), PGA (cc = 0.23; p = 0.01) and DLQI (cc = 0.28; p = 0.001) scores. Higher 4IIQ scores were observed in patients with asthma/chronic obstructive pulmonary disease (cc=0.29; p = 0.003), peptic ulcer disease (cc = 0.27; p = 0.006), as well as in those using insulin (cc = 0.38; p = 0.0001). It is notable that insulin was also strongly associated with itch episodes occurring at night (cc = 0.66; p = 0.009), difficulties in falling asleep (cc = 0.71; p = 0.002) and awakenings (cc = 0.77; p = 0.002) due to itch. In addition, the use of any pharmacotherapy was associated with longer episodes of itch (cc = 0.26; p = 0.04). Lower Hb concentrations were associated with higher scores of NRS in the last 3 days (standardized Pearson’s C = –0.23; p = 0.03) and maximal NRS (standardized Pearson’s C = –0.23; p = 0.03). Finally, chronic heart failure was associated with itch episodes lasting more than 10 min (standardized Pearson’s C = 0.34; p = 0.02) and anxiety due to itch (standardized Pearson’s C = 0.4; p = 0.02). Coexistence of psoriatic arthritis predicted higher itch intensity during the last 3 days, as measured by VRS (cc = 0.36; p = 0.003).
Logistic regression analysis was performed for CI as a dependent variable (effect) (Table III). The most relevant factors determining the presence of CI included the use of antacids (OR 45.1), ARB (OR 20.9), ACEI (OR 2.5) and beta-blockers (OR 6.1), along with xerosis intensity (OR 1.8), PGA score (OR 1.7), whereas the application of psychiatric drugs other than SSRIs (OR 0.015), allopurinol (OR 0.06), coexistence of arterial hypertension (OR 0.09) and the use of emollients (OR 0.29) reduced the probability of occurrence of CI.
Table III. Logistic regression parameters for chronic itch as an effect
This study revealed that the prevalence of CI (72.0%) in psoriatic patients was similar to that found in previous reports (13, 31). Mean itch intensity in the last 3 days assessed by NRS was 5.8 ± 2.3 points; previous studies reported itch intensity assessed by visual analogue scale (VAS) as approximately 4.2–6.4 points (17, 32). In our study non-senior and senior groups experienced CI in approximately 70% of patients, with no statistical differences. It must be noted that psoriasis was less severe in our elderly patients as evaluated by PASI and PGA scores, whereas systemic comorbidities and pharmacotherapy were more prevalent compared with patients aged below 65 years. Few reports specifically mentioned itch in elderly psoriatic patients. Sampogna et al. (18) revealed that 68.2% of patients aged 60 years and over experienced itch; no differences were observed compared with younger age groups (p = 0.355). In a study by Kwon et al. (10) performed among 129 elderly-onset psoriatic subjects itch bothered 74.6% of subjects. No statistical differences were noted compared with middle age-onset groups. In our study, however, elderly patients presented higher 4IIQ scores and rarely developed itch at midday.
Patients with CI demonstrated higher levels of xerosis, along with higher BSA, PGA and DLQI scores. Xerosis was reported as a major aggravating factor for psoriatic itch in several studies (15, 32). Taking into account its high prevalence in the literature regarding geriatric dermatology (values exceeding 50%) (8, 9, 33) it seems likely that this symptom is closely associated with CI in psoriasis, especially in elderly patients (although the impact of xerosis on CI was found to be mediocre, as demonstrated by the OR 1.839 in logistic regression analysis).
Systemic comorbidities are possible underlying causes of systemic itch (class III according to IFSI) (12), although the exact mechanisms warranting their association with CI in our psoriatic cohort are not known. Interestingly, studies have revealed that itching may occur as a prodromal symptom of asthmatic attack (34, 35). Anaemia is mentioned as another possible cause of CI (19), while our study demonstrated that lower haemoglobin concentration is associated with higher itch intensity (NRS during the last 3 days and maximal NRS during the course of the disease). We speculate that the coexistence of anaemia with psoriasis might exacerbate itch.
In addition, aspirin intake was more common in the CI group (than within non-itch psoriatic patients), although a causal relationship is difficult to establish. Subsequently, the presence of peptic ulcer disease displayed an association with 4IIQ scores. Indeed, a report has associated Helicobacter pylori infection with CI (36); therefore we speculate that a subset of patients might have had coexistent H. pylori infection, subsequent ulcer disease, and exacerbation of psoriatic itch. Moreover, patients with higher 4IIQ scores clearly used insulin more often. Insulin intake was also strongly associated with itch episodes occurring at night and strongly correlated with higher itch severity in the last 3 days (assessed by VRS), difficulty in falling asleep, and awakenings. The role of diabetes in eliciting itch is unclear; a possible role of diabetic polyneuropathy was suggested (37). In the current study, insulin was used in patients with advanced diabetes, which might partly account for the aforementioned findings.
The interpretation of logistic regression model for CI (as a dependent variable) stimulates discussion. It implied a “protective” role of emollients, presence of hypertension, intake of allopurinol and psychiatric drugs other than SSRIs; while, on the other hand, antacids, ARB, ACEI and beta-blockers strongly favoured the occurrence of CI in psoriatic patients. Such a powerful impact of antacids and ARB intake (both strong positive), as well as of psychiatric drugs other than SSRIs and allopurinol intake (both strong negative) on CI occurrence within psoriatic patients needs further and more detailed research, focusing not only on measuring the power of association between CI and its influencing factors, but also, and especially, on their causality. Numerous drugs may account for drug-induced pruritus (38); analysis of their role in eliciting or promoting CI in a “classic” itchy dermatosis, such as psoriasis, is awkward. In addition, none of these drugs reached statistical significance when tested individually in the context of CI. Nonetheless, these findings support widely acknowledged multifactorial pathogenesis of CI and raise the question as to whether concomitant pharmacotherapy and polypharmacy might play a role in psoriatic itch, possibly due to drug interactions. It must be emphasized that psoriasis is currently regarded as a systemic disease with various cardiometabolic comorbidities and widespread inflammatory state (39). Acknowledging the present findings, which demonstrate a high influence of comorbidities and pharmacotherapy on pruritus, we hypothesize that they are relevant factors, in addition to cutaneous inflammation, influencing its development in psoriasis. Moreover, to the best of our knowledge, the current study is the first to report possible associations between psoriatic pruritus and the co-administration of drugs utilized in managing various coexisting systemic conditions.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize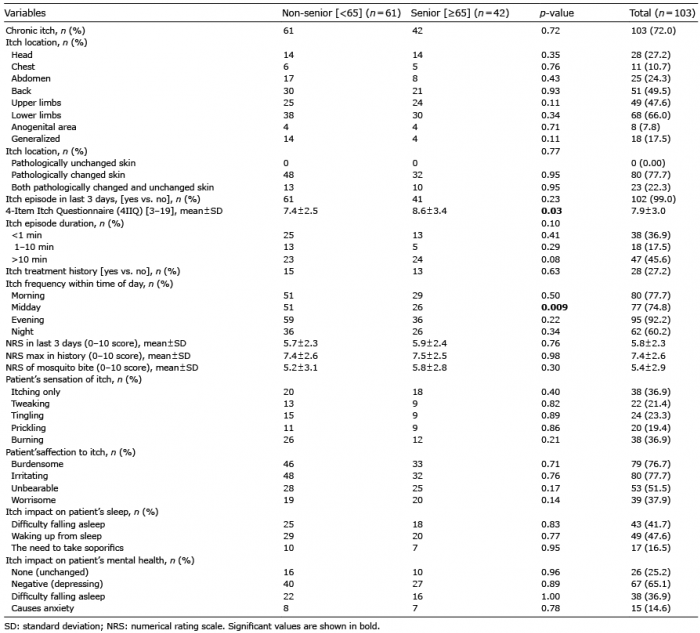 Click to show fullsize
Click to show fullsize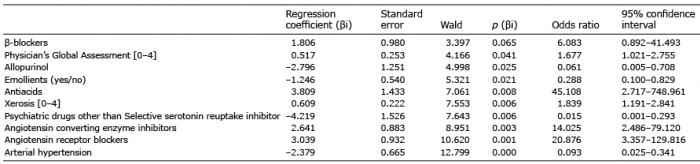 Click to show fullsize
Click to show fullsize