


1Internal Medicine, Hospital General Universitario Gregorio Marañón, C/. Doctor Esquerdo, 46, ES-28007 Madrid, Spain, and 2Department of of Medicine, Division of Endocrinology, Department of Medicine, Emory University, Atlanta, GA, USA. E-mail: paco.galeano.valle@gmail.com
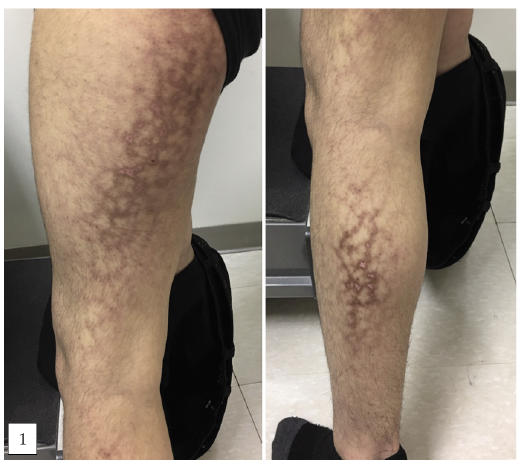
A 23-year-old transgender male (born female, male gender identity) had commenced hormone therapy consisting of intramuscular injections of testosterone in the thighs 5 months prior and intramuscular injection of medroxyprogesterone 2 months prior to presentation. He presented to the endocrinology clinic in winter after experiencing increased facial acne, voice deepening and decreased breast tissue. Additionally, he noticed a growing bruise in the lateral lower left leg that appeared one month before (Fig. 1). This bruise had spread upwards to his lateral thigh. He denied pain, pruritus, fever or swelling. Physical examination showed a reticular erythematous rash that stretched along his lateral left leg to the top of the thigh. Blood tests showed testosterone 1,241 ng/dl, estradiol 40 pg/ml. All other results including full chemistry panel and complete blood count were unremarkable.
What is your diagnosis? See next page for answer.
Fig. 1. Reticular erythematous rash that stretched along his lateral left leg to the top of the thigh.
Acta Derm Venereol
Diagnosis: Erythema ab igne
On questioning, the patient worked in a cold office and admitted to use a heater placed close to his left side. Ery-thema ab igne (EAI) occurs due to repeated or prolonged exposure to infrared radiation of sub-threshold intensity that is insufficient to cause burn and appears 2 weeks to a few months after exposure (1). This patient used a heater placed close to his left side. EAI was traditionally associated with exposure to open fires or stoves but nowadays is more often related to basic infrared heat sources like radiators and water bottles. EAI may be diagnostically challenging due to its infrequency (2, 3).
Conditions to consider in the differential diagnosis of an erythematous rash in a transgender male patient include livedo reticularis, livedo racemosa, melasma (chloasma) (1), discoid lupus erythematous (4), erythema ab igne (2, 3), erythema marginatum, autoimmune progesterone dermatitis (5), erythrocyanosis and reticular erythematous mucinosis (1). Especially, two conditions may cause a rash in a patient under hormone therapy: erythema multiforme (EM) and acne vulgaris. EM is an acute, self-limiting disease typically associated with hypersensitivity reactions to viruses, bacterial infections or drugs, but also to endogenous and exogenous sexual hormones. EM is characterized by targetoid erythematous lesions with predominant acral localization and frequently have mucosal involvement (6). Our case did not present any of these characteristics. Acne vulgaris is a chronic inflammatory dermatosis characterized by comedones and chronic inflammatory lesions, including papules, pustules, or nodules on the face and upper torso, and is a side effect that commonly appears 1-6 months after initation of masculinizing hormone therapy (7).
Exposure to heat can lead to a transient, blanchable, reticulated erythema. With chronic exposure, EAI appears as a brownish reticulated, erythematous, hyperpigmented and hypopigmented eruption, and may also present as cutaneous atrophy, telangiectasia, and subepidermal bullae. EAI is typically asymptomatic, but may cause a mild burning sensation and pruritus. Its histopathology may appear relatively normal and is reminiscent of chronic actinic damage (1–3). The prognosis for EAI is good, with removal of the offending heat source typically resulting in a gradual regression of the hyperpigmentation. In chronic cases, additional treatment options include topical retinoids, 5-fluorouracil cream, and laser treatment (2, 3).


 Click to show fullsize
Click to show fullsize