Drug-induced Linear IgA Bullous Dermatosis: a Case Report and Review of the Literature
Judith Lammer, Rüdiger Hein, Sophie Roenneberg, Tilo Biedermann and Thomas Volz
Department of Dermatology and Allergology, Technical University Munich, Munich, Germany
Linear IgA bullous dermatosis (LABD) is a rare subepidermal autoimmune blistering disease characterized by linear deposition of IgA along the basement membrane zone. Although most reported cases are idiopathic, there is a subset of patients with drug-induced LABD. Various drugs have been associated with the drug-induced form of the disease. This paper reviews the literature on drugs reported to elicit linear IgA dermatosis and its specific clinical presentation. In addition, a case report of a 77-year-old male patient with linear IgA dermatosis induced by vancomycin is described. The aim of this paper is to emphasize the need to include this differential diagnosis in cases of suspected adverse drug reactions, as well as to highlight the role of drugs in LABD.
Key words: drug-induced linear IgA bullous dermatosis; vancomycin; autoimmunity.
Accepted Feb 26, 2019; E-published Feb 27, 2019
Acta Derm Venereol 2019; 99: XX–XX.
Corr: Thomas Volz, Department of Dermatology and Allergology, Technical University Munich, Biedersteiner Str. 29, DE-80802 Munich, Germany. E-mail: thomas.volz@tum.de
Linear IgA bullous dermatosis (LABD) is a rare blistering autoimmune disease. Although most cases are idiopathic, numerous drugs have been identified as capable of eliciting LABD. This paper provides an overview of the pathogenesis, diagnosis and treatment of drug-induced LABD, together with a report of a representative case of vancomycin-induced LABD. In addition, the results of a comprehensive literature review are reported to provide an overview of putative culprit drugs and their frequency, in order to enable clinicians to diagnose patients with putative adverse drug reactions presenting with blistering.
Linear IgA bullous dermatosis (LABD) is a rare immune-mediated vesiculobullous disease with an incidence of 0.2–2.3 cases per million-population per year (1). LABD can occur both in children and in adults. In children it is also named chronic bullous disease of childhood, and presents, on average, at approximately 4.5 years of age (2, 3). In adults, 2 peaks are described with regard to disease onset: teenage years and the 60s (4). The childhood onset form is characterized by development of annular or polycyclic plaques and papules with blistering around the edges (string-of-pearls sign), primarily around the mouth and eyes, lower abdomen, thighs, buttocks, genitals, wrists and ankles. In contrast, the adult-onset form of LABD presents with lesions on the trunk, head and limbs (3). In both children and adults, the mucosa can be affected. The string-of-pearls sign is less common in adults in comparison to the childhood form. The subjective symptoms vary from almost none or mild pruritus to severe burning (3). Applying direct immunofluorescence to a skin biopsy, which shows the presence of linear deposition of immunoglobulin A (IgA) at the dermoepidermal junction, is mandatory to confirm the diagnosis (5–9). In addition, deposition of IgG and C3 may be detected (6). While most cases of LABD are idiopathic, an association with either drug intake or systemic autoimmune diseases, such as rheumatoid arthritis, psoriasis, systemic lupus erythematodes, Crohn’s disease and ulcerative colitis, has been reported, the latter displaying the most frequent association with LABD (10–15). Regarding the drug-induced form, drugs such as antibiotics, analgesics, antihypertensives, antiepileptics or immunosuppressants have been identified as potential causative agents (16). We report here a patient with vancomycin-induced linear IgA dermatosis and review the literature regarding drug-induced LABD by searching the PubMed database using the key words ‘’linear immunoglobulin A disease’’, ‘’linear IgA disease’’, ‘’linear IgA bullous disease’’, ‘’linear IgA bullous dermatosis’’, and ‘’LAD’’, ‘’LABD’’, both alone and in association with the terms ‘’drug’’, ‘’drug-induced’’ and ‘’drug-associated’’.
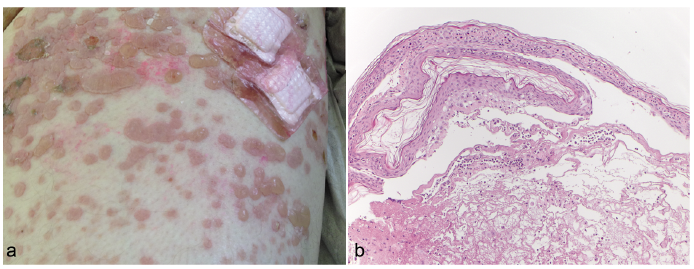
A 77-year-old man was referred to our department with a 4-day history of bullous dermatosis. Previously he underwent implantation of a hip joint endoprosthesis, complicated by prosthetic joint infection. Due to microbiological detection of multidrug resistant Gram-negative bacteria the patient was treated with vancomycin. Approximately 2 weeks after initiating intravenous vancomycin, he developed a polymorphic, erythematous vesiculobullous rash. Except for light itching at the beginning, the patient reported no other symptoms. Vital parameters were stable on presentation. Past medical history included coxarthrosis, coronary heart disease, atrial fibrillation, spastic hemiparesis and hemiplegia after subarachnoidal haemorrhage, depression and testicular hydrocele. There were no known previous allergic drug reactions. His long-term medication included citalopram, pantoprazole, bisoprolol, enalapril, acetylsalicylic acid, quetiapine, simvastatin, metamizole, tilidine and apixaban. No changes in his long-term medication, except for vancomycin and certoparin sodium instead of apixaban, had been made. Basic laboratory examination did not reveal any abnormalities and his vancomycin serum level was within normal limits. Physical examination revealed multiple tense, fluid-filled bullae, urticarial plaques and targetoid macules with central and perilesional vesicles, some of them coalescing in a herpetiform distribution (Fig. 1A). Lesions were located on the abdomen, both groins and thighs, as well as on his upper left arm. In addition, the patient had some oral mucosal erosions, whereas the ocular and genital mucosa were spared. An adverse drug-induced reaction to vancomycin was suspected. Thus, vancomycin treatment was stopped immediately on admission. Vancomycin-induced LABD, bullous pemphigoid or erythema exsudativum multiforme were considered in the differential diagnosis. Skin biopsies were taken and direct immunofluorescence (DIF) testing was performed. Histopathological examination showed a subepidermal blister formation and an inflammatory neutrophilic infiltrate (Fig. 1B). DIF of the perilesional skin demonstrated linear IgA and C3 deposition at the basal membrane zone (BMZ) without detection of IgG and IgM. Indirect immunofluorescence (IIF) was negative. No antibodies against bullous pemphigoid BP180 and BP230 could be detected using specific enzyme-linked immunoassay (ELISA). Swabs for herpes virus PCR were negative. Based on the history, histology and the DIF examination vancomycin-induced LABD was diagnosed. The patient was treated with prednisolone 80 mg i.v. and the dose decreased gradually. Skin management included antimicrobial barrier dressings and corticosteroid (betamethasone diproprionate 0.05%) ointment. The patient improved rapidly within days. Complete remission was noted after 2 weeks of therapy. Oral prednisolone was slowly tapered during the following 2 months. After stopping oral corticosteroid therapy, no new lesions have been reported. A 6-month follow-up revealed no signs of recurrence.
LABD can be subclassified into an idiopathic and a drug-induced variant. Drug-induced cases represent approximately 37.5% of LABD in adults (1). Since the first publication reporting drug-induced LABD in 1981, more than 100 cases have been published associating different drugs, with vancomycin being the most frequent (16, 17). Other drugs include different classes of drugs, such as antibiotics, non-steroidal anti-inflammatory agents, antiepileptic agents or antihypertensives. The most commonly reported drugs except for vancomycin were phenytoin and trimethoprim/sulfamethoxazole (16). Recently, the anti-TNF antibody infliximab has also been implicated in triggering an outbreak of linear IgA dermatosis as a paradoxical effect in patients with inflammatory bowel disease (18, 19). Table I gives an updated non-exhaustive list of drugs associated with LABD published in the scientific literature. Their frequency distribution is shown in Fig. 2.
The pathogenesis of drug-induced LABD is yet to be fully elucidated. Drug-specific T cells and their cytokines may play an important role, as interleukins IL-4, IL-5, IL-6, IL-10 and transforming growth factor β increase IgA synthesis (20). Yawalkar et al. characterized different cytokines involved in drug-induced LABD using the supernatant of lymphocyte transformation test (LTT) cultures (21). Their data showed significantly increased levels of IL-5 and interferon (IFN)-γ in the supernatant of LTT cultures exposed to the suspected drugs compared with negative controls. Cytotoxic CD8+ lymphocytes are assumed to play an important role provoking initial autoantigen recognition in drug-induced cases (21). In idiopathic LABD, LAD285, BP180 and BP230 have been identified as major target antigens. BP180 in particular, either the NC16A domain, or the soluble 120kDA/97kDa ectodomain, is considered to contain the major target of IgG and IgA antibodies in bullous pemphigoid, LABD, and other immunobullous diseases (22). In drug-induced LABD IgA antibodies against LAD285 and BP180 as in idiopathic LABD were identified (23). Involved drugs may cause an autoimmune response by cross-reaction with target epitopes, by altering the conformation of epitopes, or by exposing previously sequestered antigens to the immune system (24–26). Despite positive DIF findings, indirect immunofluorescence results are often negative. Circulating IgA antibodies in these patients have either low concentrations or they are not reactive to BMZ antigens in their native form. In patients with vancomycin-induced LABD it was demonstrated recently that co-incubation of patient’s sera with vancomycin renders IgA reactive with the BMZ, as demonstrated by indirect immunofluorescence (27). Furthermore, COL7 was identified as the major autoantigen targeted by these IgA antibodies. In addition, some authors suggest that infections and subsequent treatment may serve as cofactors in the pathogenesis of drug-induced LABD. With regard to idiopathic LABD, studies show associations with upper respiratory tract and gynaecological infections, typhoid, brucellosis, tetanus, varicella-zoster and tetanus (2, 8, 28, 29). In our patient, the blistering eruption occurred 2 weeks after initiating vancomycin therapy. The disease occurred probably because of 2 factors: drug and infection together. The majority of patients with reported drug-induced LABD also had other diseases, such as neoplasia (1, 7, 30–34), diabetes (1, 30, 35–38), heart and lung diseases (1, 36, 39–42), rheumatoid arthritis (43–45) or ulcerative colitis (18, 19). Concomitant diseases may also be implicated in triggering the onset of suspected drug-induced LABD (30). To prove an exclusive role for newly administered drugs in induction of drug-induced LABD, there must be a definite time-relationship between drug intake and subsequent onset of the rash as a direct association of LABD with bladder cancer, rheumatoid arthritis or ulcerative colitis has been described (11, 14, 15, 46).
Patients with drug-induced LABD tend to be older than adult patients with idiopathic LABD and are more likely to be male (1, 16, 39). Lings & Bygum compared drug-induced with idiopathic cases, showing that the mean age at disease onset in drug-induced LABD was 66.5 years compared with a mean age of 51 years in the idiopathic group, and the male-to-female ratio was 1.0 vs. 0.5 (1). However, it must be considered that the probability of having an internal disease and of taking medications increases with age. In addition, the fact that an elderly patient takes more than one medication could account for an increased likelihood of a hypersensitivity reaction (16). Until now, typical clinical, histological or immunological features of the drug-induced subtype have not been identified. Idiopathic and drug-induced LABD can be clinically polymorphic, mimicking dermatitis herpetiformis, bullous pemphigoid, pemphigus vulgaris, erythema multiforme and toxic epidermal necrolysis (TEN) (5, 6, 47). Mucocutaneous manifestations of patients with drug-induced LABD did not differ from those with the idiopathic form (23, 48). Reported cases of drug-induced LABD describe vesiculobullous eruptions, erythematous plaques, target or target-like lesions or string-of-pearls (9, 23). The most common sites involved were upper and lower limbs, including palms and soles, followed by trunk, buttock, and face/neck (23, 36). Some authors suggest that in drug-induced LABD, mucosal or conjunctival lesions were lacking, while up to 40% of patients with idiopathic LABD have mucosal involvement (49, 50). In contrast, a recent case series did not support these findings and showed no difference in mucosal involvement between the 2 groups (51). However, drug-induced LABD tends to be more severe, extensive and atypical than the idiopathic form. Positivity of Nikolsky’s sign and appearance of large erosions were significantly more frequent in these patients, sometimes clinically mimicking TEN. Indeed, several cases of drug-induced LABD clinically resembling TEN or Stevens-Johnson syndrome/toxic epidermal necrosis (SJS/TEN) overlap have been reported (33, 39, 47, 51–55). Because drug-induced LABD may sometimes be life-threatening, early direct immunofluorescence examination is recommended for all patients with positivity of Nikolsky’s sign and large skin erosions (51). A histological comparison of spontaneous LABD and of drug-induced LABD demonstrated no difference between the 2 types regarding histological patterns. Skin biopsies usually reveal subepidermal blisters containing inflammatory cells, mainly neutrophils and, occasionally, eosinophils. Focal necrotic keratinocytes were more frequent in drug-induced LABD, but the difference did not reach statistical significance (51). DIF reveals linear IgA deposits along the basement membrane. In more than 30% of idiopathic cases this is accompanied by IgG deposits (56). In drug-induced LABD almost one-third of the cases show additional linear deposition of C3 at the BMZ, as well as the DIF pattern, as presented by our patient (49, 57). However, there are no specific immunofluorescence patterns to differentiate with certainty between idiopathic and drug-induced LABD (51). In the majority of drug-induced cases, indirect immunofluorescence on monkey oesophagus failed to identify circulating antibodies (40, 57–61). The rate of indirect immunofluorescence positivity may be low because of the heterogeneity of target antigens (24).
In the present report, chronology (first lesions 14 days after vancomycin introduction, and resolution after discontinuation) is in accordance with time-frames reported in the literature. The onset of cutaneous manifestations in patients with LABD induced by vancomycin ranged from 2 to 21 days upon administration of the drug. The latency periods in other drugs than vancomycin ranged from 1 to 780 days (16).
Drug-induced LABD is usually characterized by spontaneous remission after discontinuation of the causative agent (24, 36, 50, 60). However, in contrast to previous assumptions, Fortuna et al. showed that, although in the majority of cases reported up to 2010 the suspected drug was withdrawn, up to 50% of the patients required additional therapy to avoid amplification of the disease by the immunological signal, resulting in a self-maintaining immune response (16). Administration of dapsone, sulphonamides, colchicine, topical and oral corticosteroids or intravenous immunoglobulins (IVIG) has been reported for therapy (5–7, 30). In contrast to idiopathic LABD, long-term immunosuppression seems not to be necessary in drug-induced LABD (16). To distinguish drug-induced LABD from the idiopathic subtype, the onset within the time of drug administration is the most important characteristic. The temporal sequence is also the most important clinical data to determine the causal drug (30). The cause–effect relationship is based on the onset of the rash upon initiation of the suspected drug (challenge), followed by withdrawal of the drug (dechallenge), and evaluation of spontaneous resolutions of lesions (48, 60).
Recently, the concept of drug-induced LABD has been questioned. Despite a considerable number of cases reporting associations between LABD and medications, there is poor evidence of proven causality in most of them (16). The majority of patients were exposed to multiple concurrent medications. Because of this polypharmacy a confident distinction was not always possible. Thus, establishing a cause–effect relationship may be challenging. As provocation tests are not usually performed in these patients, absolute proof of the relationship of LABD with the suspected drug cannot be obtained (4, 48). Only a few cases were confirmed by a dechallenge-rechallenge procedure, which showed positive results (the lesions recurred after rechallenge) (17, 30, 62–64). A challenge-dechallenge-rechallenge testing protocol should be the gold-standard procedure confirming the diagnosis of drug-induced LABD. However, patients rechallenged with the offending drug might have a severe recurrence, including a shorter latency and a longer disease course, and LABD in these patients may be life-threatening (8, 9). To establish the diagnosis of drug-induced LABD, already available algorithms might be helpful to reach a correct ‘’causality assessment’’ between the suspected drug and the adverse event, LABD (65). Over the past 30 years, several algorithms for causality assessment in adverse drug reactions (ADR) have been suggested (55, 66). Currently, one of the most general and widely accepted is the Naranjo score (Table II), as this offers a simple methodology (51, 67). According to the Naranjo probability scale and previous conclusive reports on this reaction, the relationship of vancomycin treatment with the cutaneous eruption in our patient is likely. Unfortunately, few authors use algorithms for causality assessment in reporting drug-induced LABD (1, 30, 35, 51). The majority of these cases were assigned the probability score “possible ADR”. Imputability scores might be helpful, but, notably, they have never been validated for LABD (68).
In conclusion, drug-induced LABD is an uncommon condition, in which LABD is triggered by medication. The list of medications implicated in drug-induced LABD development has grown in recent years, with vancomycin being the most common drug involved. Due to the rise of highly resistant beta-lactam Gram-positive bacteria, vancomycin use has increased considerably. Therefore, it is important to recognize LABD as a potential hypersensitivity reaction, which can be life-threatening without early identification. It is important to be aware that drug-induced LABD can mimic TEN. This report aims to draw attention to the possibility of LABD being an adverse drug reaction, and to emphasize the need for a biopsy and direct immunofluorescence staining. Early diagnosis is important for its management, because discontinuing the causative drug is most crucial. It may be challenging to identify the causative agent of LABD, because many patients are treated with multiple drugs. Clinicians must be cautious in establishing causality. The use of algorithms to estimate the probability of ADR can help in establishing the correct diagnosis.
The authors have no conflicts of interests to declare.
- Lings K, Bygum A. Linear IgA bullous dermatosis: a retrospective study of 23 patients in Denmark. Acta Derm Venereol 2015; 95: 466–471.
View article Google Scholar - Wojnarowska F, Marsden RA, Bhogal B, Black MM. Chronic bullous disease of childhood, childhood cicatricial pemphigoid, and linear IgA disease of adults. A comparative study demonstrating clinical and immunopathologic overlap. J Am Acad Dermatol 1988; 19: 792–805.
View article Google Scholar - Venning VA, Taylor CJ, Ting A, Wojnarowska F. HLA type in bullous pemphigoid, cicatricial pemphigoid and linear IgA disease. Clin Exp Dermatol 1989; 14: 283–285.
View article Google Scholar - Fortuna G, Marinkovich MP. Linear immunoglobulin A bullous dermatosis. Clin Dermatol 2012; 30: 38–50.
View article Google Scholar - Wilson BD, Beutner EH, Kumar V, Chorzelski TP, Jablonska S. Linear IgA bullous dermatosis. An immunologically defined disease. Int J Dermatol 1985; 24: 569–574.
View article Google Scholar - Baden LA, Apovian C, Imber MJ, Dover JS. Vancomycin-induced linear IgA bullous dermatosis. Arch Dermatol 1988; 124: 1186–1188.
View article Google Scholar - Whitworth JM, Thomas I, Peltz SA, Sullivan BC, Wolf AH, Cytryn AS. Vancomycin-induced linear IgA bullous dermatosis (LABD). J Am Acad Dermatol 1996; 34: 890–891.
View article Google Scholar - Klein PA, Callen JP. Drug-induced linear IgA bullous dermatosis after vancomycin discontinuance in a patient with renal insufficiency. J Am Acad Dermatol 2000; 42: 316–323.
View article Google Scholar - Jones DH, Todd M, Craig TJ. Early diagnosis is key in vancomycin-induced linear IgA bullous dermatosis and Stevens-Johnson syndrome. J Am Osteopath Assoc 2004; 104: 157–163.
View article Google Scholar - Horiguchi Y, Ikoma A, Sakai R, Masatsugu A, Ohta M, Hashimoto T. Linear IgA dermatosis: report of an infantile case and analysis of 213 cases in Japan. J Dermatol 2008; 35: 737–743.
View article Google Scholar - Paige DG, Leonard JN, Wojnarowska F, Fry L. Linear IgA disease and ulcerative colitis. Br J Dermatol 1997; 136: 779–782.
View article Google Scholar - Cooke N, Jenkinson H, Wojnarowska F, McKenna K, Alderdice J. Coexistence of psoriasis and linear IgA disease in a patient with recent herpes zoster infection. Clin Exp Dermatol 2005; 30: 643–645.
View article Google Scholar - Tobon GJ, Toro CE, Bravo JC, Canas CA. Linear IgA bullous dermatosis associated with systemic lupus erythematosus: a case report. Clin Rheumatol 2008; 27: 391–393.
View article Google Scholar - Hayakawa K, Shiohara T, Yagita A, Nagashima M. Linear IgA bullous dermatosis associated with rheumatoid arthritis. J Am Acad Dermatol 1992; 26: 110–113.
View article Google Scholar - De Simone C, Guerriero C, Pellicano R. Linear IgA disease and ulcerative colitis. Eur J Dermatol 1998; 8: 48–50.
View article Google Scholar - Fortuna G, Salas-Alanis JC, Guidetti E, Marinkovich MP. A critical reappraisal of the current data on drug-induced linear immunoglobulin A bullous dermatosis: a real and separate nosological entity? J Am Acad Dermatol 2012; 66: 988–994.
View article Google Scholar - Gabrielsen TO, Staerfelt F, Thune PO. Drug-induced bullous dermatosis with linear IgA deposits along the basement membrane. Acta Derm Venereol 1981; 61: 439–441.
View article Google Scholar - Hoffmann J, Hadaschik E, Enk A, Stremmel W, Gauss A. Linear IgA bullous dermatosis secondary to infliximab therapy in a patient with ulcerative colitis. Dermatology 2015; 231: 112–115.
View article Google Scholar - Bryant KD, DeNunzio MJ, Ford MJ. Linear IgA dermatosis after infliximab infusion for ulcerative colitis. JAAD Case Rep 2016; 2: 448–450.
View article Google Scholar - Briere F, Bridon JM, Chevet D, Souillet G, Bienvenu F, Guret C, et al. Interleukin 10 induces B lymphocytes from IgA-deficient patients to secrete IgA. J Clin Invest 1994; 94: 97–104.
View article Google Scholar - Yawalkar N, Reimers A, Hari Y, Hunziker T, Gerber H, Muller U, et al. Drug-induced linear IgA bullous dermatosis associated with ceftriaxone- and metronidazole-specific T cells. Dermatology 1999; 199: 25–30.
View article Google Scholar - Allen J, Wojnarowska F. Linear IgA disease: the IgA and IgG response to dermal antigens demonstrates a chiefly IgA response to LAD285 and a dermal 180-kDa protein. Br J Dermatol 2003; 149: 1055–1058.
View article Google Scholar - Palmer RA, Ogg G, Allen J, Banerjee A, Ryatt KS, Ratnavel R, et al. Vancomycin-induced linear IgA disease with autoantibodies to BP180 and LAD285. Br J Dermatol 2001; 145: 816–820.
View article Google Scholar - Paul C, Wolkenstein P, Prost C, Caux F, Rostoker G, Heller M, et al. Drug-induced linear IgA disease: target antigens are heterogeneous. Br J Dermatol 1997; 136: 406–411.
View article Google Scholar - Guide SV, Marinkovich MP. Linear IgA bullous dermatosis. Clin Dermatol 2001; 19: 719–727.
View article Google Scholar - Zone JJ, Pazderka Smith E, Powell D, Taylor TB, Smith JB, Meyer LJ. Antigenic specificity of antibodies from patients with linear basement membrane deposition of IgA. Dermatology 1994; 189 Suppl 1: 64–66.
View article Google Scholar - Yamagami J, Nakamura Y, Nagao K, Funakoshi T, Takahashi H, Tanikawa A, et al. Vancomycin mediates IgA autoreactivity in drug-induced linear IgA bullous dermatosis. J Invest Dermatol 2018; 138: 1473–1480.
View article Google Scholar - Godfrey K, Wojnarowska F, Leonard J. Linear IgA disease of adults: association with lymphoproliferative malignancy and possible role of other triggering factors. Br J Dermatol 1990; 123: 447–452.
View article Google Scholar - Thune P, Eeg-Larsen T, Nilsen R. Acute linear IgA dermatosis in a child following varicella. Arch Dermatol 1984; 120: 1237–1238.
View article Google Scholar - del Pozo J, Martinez W, Yebra-Pimentel MT, Almagro M, Pena-Penabad C, Fonseca E. Linear immunoglobulin A bullous dermatosis induced by gemcitabine. Ann Pharmacother 2001; 35: 891–893.
View article Google Scholar - Ruiz-Rivero J, Hernandez-Aragues I, Pulido-Perez A, Suarez-Fernandez R. Linear IgA Bullous dermatosis presenting as toxic epidermal necrolysis. Actas Dermosifiliogr 2017; 108: 880–882.
View article Google Scholar - Prieto-Barrios M, Velasco-Tamariz V, Tous-Romero F, Burillo-Martinez S, Zarco-Olivo C, Rodriguez-Peralto JL, et al. Linear immunoglobulin A dermatosis mimicking toxic epidermal necrolysis: a case report of etanercept treatment. Br J Dermatol 2018; 178: 786–789.
View article Google Scholar - Tran D, Kossard S, Shumack S. Phenytoin-induced linear IgA dermatosis mimicking toxic epidermal necrolysis. Australas J Dermatol 2003; 44: 284–286.
View article Google Scholar - Kang MJ, Kim HO, Park YM. Vancomycin-induced linear IgA bullous dermatosis: a case report and review of the literature. Ann Dermatol 2008; 20: 102–106.
View article Google Scholar - Pena-Penabad C, Rodriguez-Lozano J, del Pozo J, Garcia-Silva J, Fonseca E. Linear IgA bullous dermatosis induced by angiotensin receptor antagonists. Am J Med 2003; 114: 163–164.
View article Google Scholar - Cerottini JP, Ricci C, Guggisberg D, Panizzon RG. Drug-induced linear IgA bullous dermatosis probably induced by furosemide. J Am Acad Dermatol 1999; 41: 103–105.
View article Google Scholar - Choudhry SZ, Kashat M, Lim HW. Vancomycin-induced linear IgA bullous dermatosis demonstrating the isomorphic phenomenon. Int J Dermatol 2015; 54: 1211–1213.
View article Google Scholar - Vinnakota S, Salonen BR. Linear IgA bullous dermatosis: a rare manifestation of vancomycin hypersensitivity. Ann Allergy Asthma Immunol 2018; 120: 101–102.
View article Google Scholar - Waldman MA, Black DR, Callen JP. Vancomycin-induced linear IgA bullous disease presenting as toxic epidermal necrolysis. Clin Exp Dermatol 2004; 29: 633–636.
View article Google Scholar - Onodera H, Mihm MC, Jr., Yoshida A, Akasaka T. Drug-induced linear IgA bullous dermatosis. J Dermatol 2005; 32: 759–764.
View article Google Scholar - Jha P, Swanson K, Stromich J, Michalski BM, Olasz E. A Rare case of vancomycin-induced linear immunoglobulin A bullous dermatosis. Case Rep Dermatol Med 2017; 2017: 7318305.
View article Google Scholar - Pereira AR, Moura LH, Pinheiro JR, Pasin VP, Enokihara MM, Porro AM. Vancomycin-associated linear IgA disease mimicking toxic epidermal necrolysis. An Bras Dermatol 2016; 91: 35–38.
View article Google Scholar - Hernandez N, Borrego L, Soler E, Hernandez J. Sulfasalazine-induced linear immunoglobulin A bullous dermatosis with DRESS. Actas Dermosifiliogr 2013; 104: 343–346.
View article Google Scholar - Coelho S, Tellechea O, Reis JP, Mariano A, Figueiredo A. Vancomycin-associated linear IgA bullous dermatosis mimicking toxic epidermal necrolysis. Int J Dermatol 2006; 45: 995–996.
View article Google Scholar - Bouldin MB, Clowers-Webb HE, Davis JL, McEvoy MT, Davis MD. Naproxen-associated linear IgA bullous dermatosis: case report and review. Mayo Clin Proc 2000; 75: 967–970.
View article Google Scholar - Rodenas JM, Herranz MT, Tercedor J, Concha A. Linear IgA disease in a patient with bladder carcinoma. Br J Dermatol 1997; 136: 257–259.
View article Google Scholar - Kakar R, Paugh H, Jaworsky C. Linear IgA bullous disease presenting as toxic epidermal necrolysis: a case report and review of the literature. Dermatology 2013; 227: 209–213.
View article Google Scholar - Collier PM, Wojnarowska F. Drug-induced linear immunoglobulin A disease. Clin Dermatol 1993; 11: 529–533.
View article Google Scholar - Kuechle MK, Stegemeir E, Maynard B, Gibson LE, Leiferman KM, Peters MS. Drug-induced linear IgA bullous dermatosis: report of six cases and review of the literature. J Am Acad Dermatol 1994; 30: 187–192.
View article Google Scholar - Nousari HC, Kimyai-Asadi A, Caeiro JP, Anhalt GJ. Clinical, demographic, and immunohistologic features of vancomycin-induced linear IgA bullous disease of the skin. Report of 2 cases and review of the literature. Medicine (Baltimore) 1999; 78: 1–8.
View article Google Scholar - Chanal J, Ingen-Housz-Oro S, Ortonne N, Duong TA, Thomas M, Valeyrie-Allanore L, et al. Linear IgA bullous dermatosis: comparison between the drug-induced and spontaneous forms. Br J Dermatol 2013; 169: 1041–1048.
View article Google Scholar - Khan I, Hughes R, Curran S, Marren P. Drug-associated linear IgA disease mimicking toxic epidermal necrolysis. Clin Exp Dermatol 2009; 34: 715–717.
View article Google Scholar - Dellavalle RP, Burch JM, Tayal S, Golitz LE, Fitzpatrick JE, Walsh P. Vancomycin-associated linear IgA bullous dermatosis mimicking toxic epidermal necrolysis. J Am Acad Dermatol 2003; 48: S56–57.
View article Google Scholar - Adler NR, McLean CA, Aung AK, Goh MS. Piperacillin-tazobactam-induced linear IgA bullous dermatosis presenting clinically as Stevens-Johnson syndrome/toxic epidermal necrolysis overlap. Clin Exp Dermatol 2017; 42: 299–302.
View article Google Scholar - Mofid MZ, Costarangos C, Bernstein B, Wong L, Munster A, Nousari HC. Drug-induced linear immunoglobulin A bullous disease that clinically mimics toxic epidermal necrolysis. J Burn Care Rehabil 2000; 21: 246–247.
View article Google Scholar - Wiadrowski TP, Reid CM. Drug-induced linear IgA bullous disease following antibiotics. Australas J Dermatol 2001; 42: 196–199.
View article Google Scholar - Neughebauer BI, Negron G, Pelton S, Plunkett RW, Beutner EH, Magnussen R. Bullous skin disease: an unusual allergic reaction to vancomycin. Am J Med Sci 2002; 323: 273–278.
View article Google Scholar - Wos-Oxley ML, Plumeier I, von Eiff C, Taudien S, Platzer M, Vilchez-Vargas R, et al. A poke into the diversity and associations within human anterior nare microbial communities. ISME J 2010; 4: 839–851.
View article Google Scholar - Pol H, Devaux S, Tournier E, Fortenfant F, Paul C. Buprenorphine-induced linear IgA bullous dermatosis “down the rail”. J Am Acad Dermatol 2013; 69: e106–107.
View article Google Scholar - Camilleri M, Pace JL. Drug-induced linear immunoglobulin-A bullous dermatosis. Clin Dermatol 1998; 16: 389–391.
View article Google Scholar - Tashima S, Konishi K, Koga H, Hashimoto T. A case of vancomycin-induced linear IgA bullous dermatosis with circulating IgA antibodies to the NC16a domain of BP180. Int J Dermatol 2014; 53: e207–209.
View article Google Scholar - McWhirter JD, Hashimoto K, Fayne S, Ito K. Linear IgA bullous dermatosis related to lithium carbonate. Arch Dermatol 1987; 123: 1120–1122.
View article Google Scholar - Kano Y, Kokaji T, Shiohara T. Linear IgA bullous dermatosis in a patient with acute lymphocytic leukemia: possible involvement of granulocyte colony-stimulating factor. Eur J Dermatol 1999; 9: 122–125.
View article Google Scholar - Avci O, Okmen M, Cetiner S. Acetaminophen-induced linear IgA bullous dermatosis. J Am Acad Dermatol 2003; 48: 299–301.
View article Google Scholar - Edwards IR, Aronson JK. Adverse drug reactions: definitions, diagnosis, and management. Lancet 2000; 356: 1255–1259.
View article Google Scholar - Kelly WN. The quality of published adverse drug event reports. Ann Pharmacother 2003; 37: 1774–1778.
View article Google Scholar - Farcas A, Bojita M. Adverse drug reactions in clinical practice: a causality assessment of a case of drug-induced pancreatitis. J Gastrointestin Liver Dis 2009; 18: 353–358.
View article Google Scholar - Benahmed S, Picot MC, Dumas F, Demoly P. Accuracy of a pharmacovigilance algorithm in diagnosing drug hypersensitivity reactions. Arch Intern Med 2005; 165: 1500–1505.
View article Google Scholar - Riemenschneider K, Diiorio DA, Zic JA, Livingood MR, Fine JD, Powers JG, et al. Drug-induced linear IgA bullous dermatosis in a patient with a vancomycin-impregnated cement spacer. Cutis 2018; 101: 293–296.
View article Google Scholar - Nguyen JK, Koshelev MV, Gill BJ, Boulavsky J, Diwan AH, Dao H, Jr. A toxic epidermal necrolysis-like presentation of linear IgA bullous dermatosis treated with dapsone. Dermatol Online J 2017; 23.
View article Google Scholar - Pinho A, Cardoso JC. [Generalized bullous eruption during treatment with vancomycin]. Acta Med Port 2017; 30: 586 (in Portuguese).
View article Google Scholar - Castellanos-Gonzalez M, Marzal-Alfaro MB, Diaz-Sanchez A, Martos MG. Linear IgA bullous dermatosis due to vancomycin and cutaneous necrosis due to terlipressin in the same patient. Indian J Dermatol Venereol Leprol 2016; 82: 723–726.
View article Google Scholar - Gameiro A, Gouveia M, Tellechea O, Goncalo M. Vancomycin-induced linear IgA bullous dermatosis: associations. Dermatol Online J 2016; 22. pii: 13030/qt8k63322n.
View article Google Scholar - Winn AE, Spillane EL, Peterson DJ, Sperling LC, Meyerle JH. False-negative direct immunofluorescence testing in vancomycin-induced linear IgA bullous dermatosis: a diagnostic pitfall. J Cutan Pathol 2016; 43: 802–804.
View article Google Scholar - Kim JS, Choi M, Nam CH, Kim JY, Park BC, Kim MH, et al. Concurrent drug-induced linear immunoglobulin A dermatosis and immunoglobulin a nephropathy. Ann Dermatol 2015; 27: 315–318.
View article Google Scholar - Nasr J, Ammoury A, Chouairy C, Megarbane H, El Habr C. Drug-induced linear IgA bullous dermatosis simulating toxic epidermal necrolysis. J Med Liban 2014; 62: 176–179.
View article Google Scholar - Ingen-Housz-Oro S, Valeyrie-Allanore L, Chanal J, Chosidow O, Wolkenstein P. Linear immunoglobulin A disease and vancomycin: letter in reply. Br J Dermatol 2014; 171: 1602–1604.
View article Google Scholar - Zenke Y, Nakano T, Eto H, Koga H, Hashimoto T. A case of vancomycin-associated linear IgA bullous dermatosis and IgA antibodies to the alpha3 subunit of laminin-332. Br J Dermatol 2014; 170: 965–969.
View article Google Scholar - Selvaraj PK, Khasawneh FA. Linear IgA bullous dermatosis: a rare side effect of vancomycin. Ann Saudi Med 2013; 33: 397–399.
View article Google Scholar - Jawitz RS, Krach K, Schapiro B. A vesiculobullous eruption in a hospitalized patient. Diagnosis: Drug-induced linear IgA bullous dermatosis (LAD) with eosinophils. Arch Dermatol 2011; 147: 1443, 1448.
View article Google Scholar - Bohm NM, Wong JG. Bullous dermatosis associated with vancomycin extravasation. Am J Med Sci 2012; 343: 177–179.
View article Google Scholar - Perez-Bustillo A, Sanchez-Sambucety P, Rodriguez-Prieto MA. A morbilliform variant of linear IgA dermatosis: a new case. Int J Dermatol 2011; 50: 1528–1530.
View article Google Scholar - Jheng-Wei L, Yi-Chin S, Wen-Hung C. Vancomycin-induced linear IgA bullous dermatosis mimicking toxic epidermal necrolysis. Indian J Dermatol Venereol Leprol 2011; 77: 537.
View article Google Scholar - McDonald HC, York NR, Pandya AG. Drug-induced linear IgA bullous dermatosis demonstrating the isomorphic phenomenon. J Am Acad Dermatol 2010; 62: 897–898.
View article Google Scholar - Walsh SN, Kerchner K, Sangueza OP. Localized palmar vancomycin-induced linear IgA bullous dermatosis occurring at supratherapeutic levels. Arch Dermatol 2009; 145: 603–604.
View article Google Scholar - Billet SE, Kortuem KR, Gibson LE, El-Azhary R. A morbilliform variant of vancomycin-induced linear IgA bullous dermatosis. Arch Dermatol 2008; 144: 774–778.
View article Google Scholar - Eisendle K, Bonatti H, Sepp N, Hopfl R. Vancomycin-induced linear IgA bullous dermatosis in an immunosuppressed transplant recipient. J Eur Acad Dermatol Venereol 2007; 21: 996–997.
View article Google Scholar - Navi D, Michael DJ, Fazel N. Drug-induced linear IgA bullous dermatosis. Dermatol Online J 2006; 12: 12.
View article Google Scholar - Brinkmeier T, Angelkort B, Frosch PJ, Herbst RA. Vancomycin-indizierte lineare IgA-Dermatose. J Dtsch Dermatol Ges 2003; 1: 212–214.
View article Google Scholar - Joshi S, Scott G, Looney RJ. A successful challenge in a patient with vancomycin-induced linear IgA dermatosis. Ann Allergy Asthma Immunol 2004; 93: 101–103.
View article Google Scholar - Solky BA, Pincus L, Horan RF. Vancomycin-induced linear IgA bullous dermatosis: morphology is a key to diagnosis. Cutis 2004; 73: 65–67.
View article Google Scholar - Ahkami R, Thomas I. Linear IgA bullous dermatosis associated with vancomycin and disseminated varicella-zoster infection. Cutis 2001; 67: 423–426.
View article Google Scholar - Bernstein EF, Schuster M. Linear IgA bullous dermatosis associated with vancomycin. Ann Intern Med 1998; 129: 508–509.
View article Google Scholar - Richards SS, Hall S, Yokel B, Whitmore SE. A bullous eruption in an elderly woman. Vancomycin-associated linear IgA dermatosis (LAD). Arch Dermatol 1995; 131: 1447–1448, 1450–1441.
View article Google Scholar - Geissmann C, Beylot-Barry M, Doutre MS, Beylot C. Drug-induced linear IgA bullous dermatosis. J Am Acad Dermatol 1995; 32: 296.
View article Google Scholar - Carpenter S, Berg D, Sidhu-Malik N, Hall RP, 3rd, Rico MJ. Vancomycin-associated linear IgA dermatosis. A report of three cases. J Am Acad Dermatol 1992; 26: 45–48.
View article Google Scholar - Friedman IS, Rudikoff D, Phelps RG, Sapadin AN. Captopril-triggered linear IgA bullous dermatosis. Int J Dermatol 1998; 37: 608–612.
View article Google Scholar - Combemale P, Gavaud C, Cozzani E, Nicolas JF, Guennoc B, Dusseau JY. Dermatose à IgA linéaire (DIAL) induite par pénicilline G. Ann Dermatol Venereol 1993; 120: 847–848.
View article Google Scholar - Wakelin SH, Allen J, Zhou S, Wojnarowska F. Drug-induced linear IgA disease with antibodies to collagen VII. Br J Dermatol 1998; 138: 310–314.
View article Google Scholar - Santos-Juanes J, Coto Hernandez R, Trapiella L, Caminal L, Sanchez del Rio J, Soto J. Amoxicillin-associated linear IgA bullous dermatosis. J Eur Acad Dermatol Venereol 2007; 21: 992–993.
View article Google Scholar - Low L, Zaheri S, Wakelin S. Amlodipine-induced linear IgA disease. Clin Exp Dermatol 2012; 37: 649–651.
View article Google Scholar - Ho JC, Ng PL, Tan SH, Giam YC. Childhood linear IgA bullous disease triggered by amoxicillin-clavulanic acid. Pediatr Dermatol 2007; 24: E40–43.
View article Google Scholar - Schroeder D, Saada D, Rafaa M, Ingen-Housz-Oro S, Valeyrie-Allanore L, Sigal ML. Dermatose à IgA linéaire induite par le vérapamil: présentation inhabituelle à type de nécrolyse épidermique toxique. Ann Dermatol Venereol 2011; 138: 302–306.
View article Google Scholar - Shimanovich I, Rose C, Sitaru C, Brocker EB, Zillikens D. Localized linear IgA disease induced by ampicillin/sulbactam. J Am Acad Dermatol 2004; 51: 95–98.
View article Google Scholar - Schafer F, Echeverria X, Gonzalez S. Linear IgA bullous dermatosis induced by ampicillin/sulbactam. Indian J Dermatol Venereol Leprol 2012; 78: 230.
View article Google Scholar - Primka EJ, 3rd, Liranzo MO, Bergfeld WF, Dijkstra JW. Amiodarone-induced linear IgA disease. J Am Acad Dermatol 1994; 31: 809–811.
View article Google Scholar - Pastuszczak M, Lipko-Godlewska S, Jaworek AK, Wojas-Pelc A. Drug-induced linear IgA bullous dermatosis after discontinuation of cefuroxime axetil treatment. J Dermatol Case Rep 2012; 6: 117–119.
View article Google Scholar - Konig C, Eickert A, Scharfetter-Kochanek K, Krieg T, Hunzelmann N. Linear IgA bullous dermatosis induced by atorvastatin. J Am Acad Dermatol 2001; 44: 689–692.
View article Google Scholar - Acostamadiedo JM, Perniciaro C, Rogers RS, 3rd. Phenytoin-induced linear IgA bullous disease. J Am Acad Dermatol 1998; 38: 352–356.
View article Google Scholar - Hughes AP, Callen JP. Drug-induced linear IgA bullous dermatosis mimicking toxic epidermal necrolysis. Dermatology 2001; 202: 138–139.
View article Google Scholar - Gonul M, Kulcu Cakmak S, Yayla D, Unal T. Linear IgA bullous dermatosis induced by moxifloxacin. Clin Exp Dermatol 2014; 39: 78–80.
View article Google Scholar - Baltazard T, Dhaille F, Duvert-Lehembre S, Lok C, Chaby G. Trimethoprim-sulfamethoxazole-induced linear IgA bullous disease presenting as toxic epidermal necrolysis. Dermatol Online J 2017; 23.
View article Google Scholar - Nantel-Battista M, Al Dhaybi R, Hatami A, Marcoux D, Desroches A, Kokta V. Childhood linear IgA bullous disease induced by trimethoprim-sulfamethoxazole. J Dermatol Case Rep 2010; 4: 33–35.
View article Google Scholar - Vaatainen N, Fraki JE, Hyvonen M, Neittaanmaki H. Purpura with a linear epidermo-dermal deposition of IgA. Acta Derm Venereol 1983; 63: 169–170.
View article Google Scholar - Sanke S, Kumar A, Chander R. Linear IgA bullous dermatosis induced by diclofenac sodium. Indian J Dermatol Venereol Leprol 2018; 84: 496–497.
View article Google Scholar - Tranvan A, Pezen DS, Medenica M, Michelson GC, Vogelzang N, Soltani KM. Interleukin-2 associated linear IgA bullous dermatosis. J Am Acad Dermatol 1996; 35: 865–867.
View article Google Scholar - Guillaume JC, Escudier B, Espagne E, Roujeau JC, Prost C, Domart P, et al. Dermatose bulleuse avec depots lineaires d’IgA le long de la membrane basale au cours d’un traitement par l’interferon gamma et l’interleukine-2. Ann Dermatol Venereol 1990; 117: 899–902.
View article Google Scholar - Kocyigit P, Akay BN, Karaosmanoglu N. Linear IgA bullous dermatosis induced by interferon-alpha 2a. Clin Exp Dermatol 2009; 34: e123–124.
View article Google Scholar - Petit D, Borradori L, Rybojad M, Morel P. Linear IgA bullous dermatosis after heart transplantation. J Am Acad Dermatol 1990; 22: 851.
View article Google Scholar - Concha-Garzon MJ, Perez-Gala S, Solano-Lopez G, Fraga J, Ishii N, Hashimoto T, et al. Ketoprofen-induced lamina lucida-type linear IgA bullous dermatosis. J Eur Acad Dermatol Venereol 2016; 30: 350–352.
View article Google Scholar - Plunkett RW, Chiarello SE, Beutner EH. Linear IgA bullous dermatosis in one of two piroxicam-induced eruptions: a distinct direct immunofluorescence trend revealed by the literature. J Am Acad Dermatol 2001; 45: 691–696.
View article Google Scholar





 Click to show fullsize
Click to show fullsize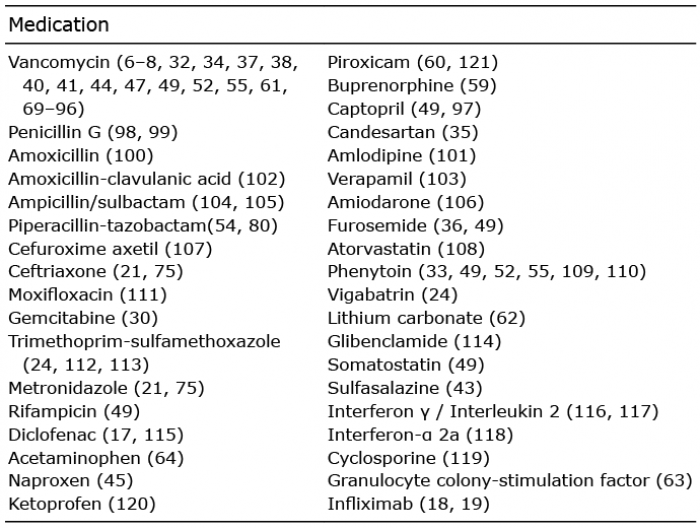 Click to show fullsize
Click to show fullsize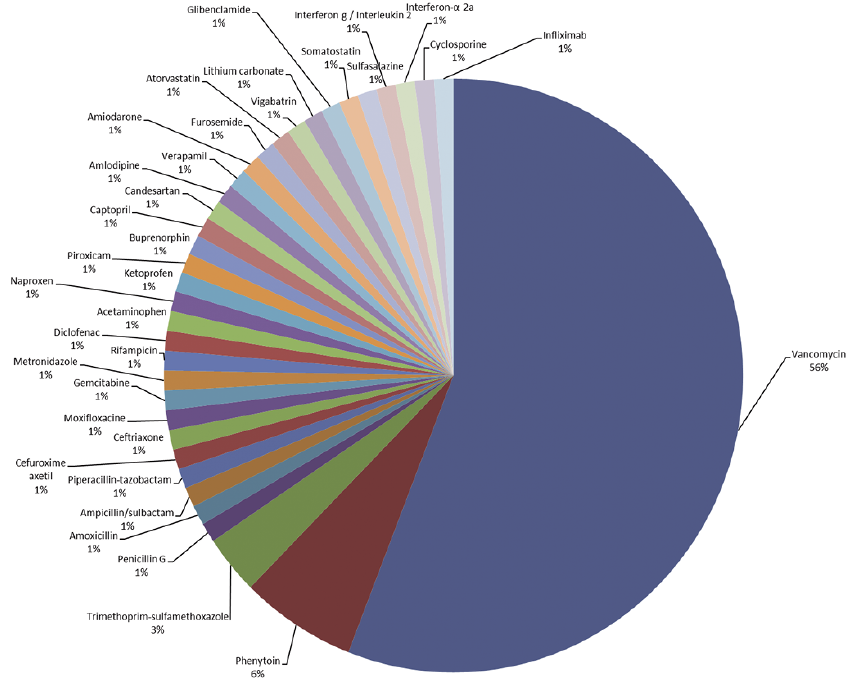 Click to show fullsize
Click to show fullsize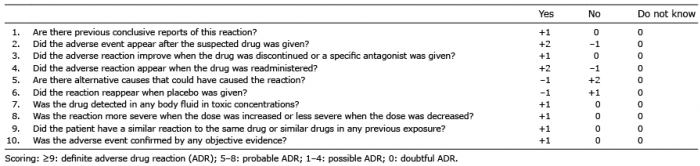 Click to show fullsize
Click to show fullsize