


1Unit of Dermatology, Department of Medicine – DIMED, University of Padova, IT-35121 Padova, and 2ULSS 6 Euganea, 3Private Dermatological Practice, and 4OUC of Histopathology, University of Padova, Padova, Italy. E-mail: michael.dennis.linder@gmail.com
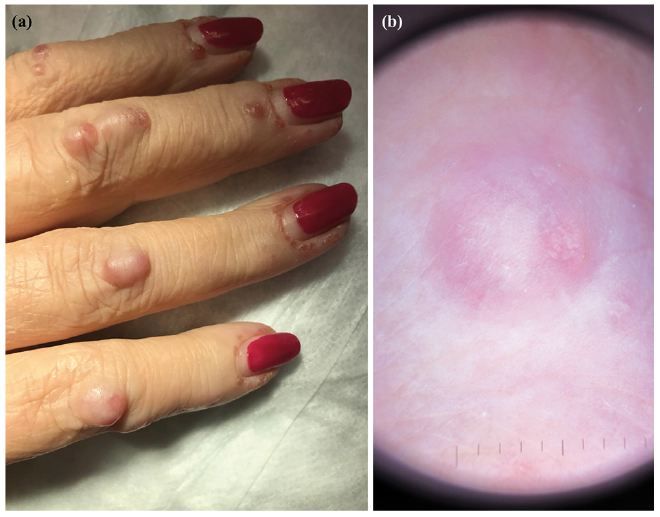
A 65-year-old Caucasian woman presented with nodular erythematous lesions on her hands. The lesions had appeared approximately 10 months previously. She reported itch and intermittent pain and swelling of the finger joints (Fig. 1). Proximal interphalangeal, metacarpophalangeal, wrist, elbow and knee arthralgias, together with magnetic resonance imaging (MRI) showing an erosive arthropathy, and a negative test for rheumatoid factor and anti-cyclic citrullinated peptide antibodies had previously led to a presumptive diagnosis of seronegative polyarthritis.
Clinical examination revealed multiple reddish-brown, firm, non-scaly, non-tender papules and nodules 2–20 mm in diameter over the dorsum and sides of the fingers. Dermo-scopy of the lesions revealed an orange-reddish background colouration with central paler yellow deposits. Around the proximal nail-folds, the papules had a “coral bead” appearance. The patient had restricted mobility; she was unable to completely open or close either hand. There were no further relevant cutaneous findings and no mucosal involvement.
Skin biopsy from a nodule on the right hand demonstrated a dermal dense infiltrate composed mainly of multiple multinucleated giant cells and histiocytes with a ground-glass aspect. These cells stained positively with CD68 (Fig. 2).
What is your diagnosis? See next page for answer.
Fig. 1. (a) Multiple reddish-brown, firm, non-scaly, non-tender papules and nodules on the right hand of a 65-year-old Caucasian woman. The lesions have a “coral bead” appearance around the proximal nail-folds. (b) Dermoscopy revealed an orange-reddish background colouration with central paler yellow deposits.
Fig. 2. Histological features: (a) dermal dense infiltrate composed mainly of multiple multinucleated giant cells and histiocytes (haematoxylin and eosin (H&E) stain 1.5×), (b) ground-glass aspect (H&E 10×).
Acta Derm Venereol 2019; XX: XX–XX.
Diagnosis: Multicentric reticulohistiocytosis
Multicentric reticulohistiocytosis (MRH) is a multisystem non-Langerhans cell histiocytosis of unknown aetiology characterized by destructive polyarthritis and papulo-nodular skin lesions (1). Since the first description of MRH by Weber & Freudenthal in 1937, nearly 200 cases have been reported in the literature. MRH mainly affects middle-aged (Caucasian) woman, but it has also been diagnosed both in children and in elderly people (2). In 18–30% of cases of MRH the skin lesions present before polyarthritis (2).
Other organs, including lungs, heart, liver, kidneys, genital tract, gastrointestinal tract and muscles, can be involved. Typically they include reddish to brown papules and nodules ranging from 1 mm to several centimetres in diameter, which most frequently appear on the dorsum of the hands and on the face, but can present on any part of the body surface (1, 2). Dermatoscopy of these lesions is reported to show 3 typical features: a homogeneous pattern with various shades of yellow, defined as a “setting-sun” pattern, brown reticular structures, and central white scar-like patches and streaks (3).
Papules overlying the periungual area often acquire a “coral beads” appearance, which constitutes a characteristic sign of MRH. Lesions are usually asymptomatic; patients occasionally report pruritus. Atypical skin lesions include macular erythema on photo-exposed areas simulating dermatomyositis, periungual telangiectasias and xanthelasma-like lesions. Oral or nasal mucosa involvement occurs in approximately half of cases (1, 2).
In approximately 40% of patients MRH presents initially with a symmetrical progressive and destructive polyarthritis, which can affect any synovial joints with a predilection for the distal interphalangeal joints; here it may evolve to mutilating arthritis, leading to “opera-glass” hands (2).
Constitutional symptoms, such as weight loss, fever and weakness, are frequently related to the disease.
An association of MRH with malignancies, including melanoma, mesothelioma, lymphoma, and carcinomas of the penis, stomach, ovary, endometrium, breast, and cervix, has been reported in approximately 25% of cases (1, 2).
Differential diagnosis may include rheumatoid arthritis, psoriatic arthritis, Reiter’s syndrome and gout in case of predominant articular involvement, but also dermatomyositis, xanthomatosis, juvenile xanthogranuloma, generalized eruptive histiocytosis, cutaneous Rosai-Dorfman disease, lepromatous leprosy, neurofibromatosis, and sarcoidosis, in case of major skin involvement.
Diagnosis is based on the histological finding of a dermal infiltrate of multinucleated giant cells with eosinophilic ground glass cytoplasm on skin or synovial biopsies. Immunohistochemistry shows positive staining for CD68 in lesional cells and is negative for S100 and CD1a (1).
MRH is sometimes reported to respond unsatisfactorily to conventional anti-inflammatory/immunosuppressive treatments, including corticosteroids, methotrexate and hydroxy-chloroquine. Anecdotal reports of successful treatments with tumour necrosis factor inhibitors or bisphosphonates are found in the literature (4).
In the case reported here, all screening investigations for malignancy were negative. It was decided to provide “conventional” treatment initially with prednisolone, 25 mg daily, and methotrexate, 5 mg weekly. The steroid was then tapered off and methotrexate was increased to 15 mg/week. At time of writing, the treatment has provided good control of both the skin lesions and the joint disease.


 Click to show fullsize
Click to show fullsize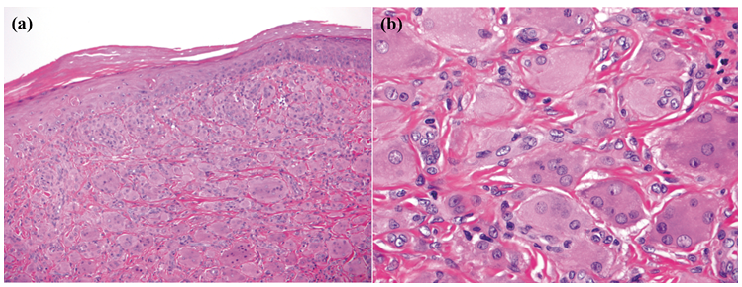 Click to show fullsize
Click to show fullsize